Role of Non Cultured Keratinocyte Graft with Sucralfate in Second Degree Scald Burns
Normal wound healing is a complex process involving three phases namely inflammatory, proliferating and remodeling. Studies have shown that sucralfate has beneficial effect on ulcers, skin lesions, burn wounds by promoting healthy granulation thereby preparing the wound bed. Whereas non cultured kertinocyte graft has proven to promote epithelialization of the wound. In this study we used non cultured keratinocyte graft with sucralfate in a paediatric patient with burn wounds on face.
Introduction
Wound healing is a physiological response of a living being to physical, chemical, mechanical or thermal injury. The wound healing process consists of several phases: homeostasis, inflammation, proliferation/granulation, and remodeling/maturation. Still, when the healing course deviates from the normal path, the healing does not advance past the inflammatory phase and becomes a chronic healing wound. This impairment is due to changes in one or more of the components that aid in wound healing like growth factors, cytokines, associated comorbidities like diabetes, infection etc [1]. In case of burns, they are complicated wounds to manage with a relative high mortality rate in especially large area burns and elderly patients [2].
Therefore to aid the process of wound healing we used sucralfate to promote healthy granulation so that the wound bed is prepared [3, 4, 5] for grafting with non-cultured keratinocytes which promotes epithelialization of the wound [6, 7, 8]. Therefore a synchronized beneficial effect towards better wound healing is provided.
Materials and Methods
This study was conducted in Tertiary Care Centre in Department of Plastic Surgery after getting the department ethical committee approval. Informed consent was obtained. The subject was a 1yr - old female child who had accidental second degree scald burn injury which involves her left side of face, pinna and retro auricular region, left arm and forearm (Figure 1). She was taken to nearby hospital within 30min- inadequate initial resuscitation. Child developed blistering and swelling around left eye next day and presented to our center after a delay of 12hrs. She was admitted in tertiary burn care unit and initial resuscitation with intravenous fluids, analgesics and prophylactic antibiotics started. After tangential excision on post burn day 5, non-cultured keratinocyte graft with sucralfate ointment is applied over the deeper areas of burn over the side of face and scalp.


Under all aseptic precautions, a 3cm x 1cm area of scalp region adjacent to burn wound was marked (Figure 2) and Local anaesthesia (2% xylocaine) was given. The donor area was derma braded (Figure 3) after the application of mupirocin ointment. The paste, containing dermabraded cells, was collected, homogenized, and was applied along with sucralfate ointment over the wound (Figure 4). A non-adherent dressing was placed on it followed by gauze dressing. The wound was inspected on the 7th day and thereafter weekly. Remnant raw area was calculated on each dressing.


Results
Intraoperative and post-operative periods were uneventful for the patient. On post-operative day 7, dressing was opened and it showed significant areas of re- epithelialization and healing (Figure 5). All second degree superficial burn wound healed completely and islands of re- epithelization appeared in deep second degree burns areas. No complications and side effects were noted during entire procedure.

Discussion
The normal pace of wound healing and epithelialization is at the rate of 1mm/day. Optimum recovery requires the wound bed and the patient to be fit. To assist with implementing the concept of wound bed preparation, the TIME acronym was developed in 2002 by a group of wound care experts, as a practical guide for use when managing patients with wounds [9]. The TIME table summarizes the four main components of wound bed preparation:
- Tissue management
- Control infection and inflammation
- Moisture imbalance
- Advancement of epithelial edge of the wound The advanced wound healing therapies aim to hasten the process of wound healing by expediting the advancement of epithelial edge of the wound. Many growth factors have been used to advance the epithelialization. As sucralfate promotes healthy granulation in wound bed and non- cultured keratinocytes provide epithelialization of the wound, a synchronized beneficial effect is achieved in wound healing process.
The epidermis is predominantly formed by highly specialized cells called keratinocytes, which play a key role in epidermal restoration following injury through proliferation and re-epithelialization (Figure 6) and mostly heal without scarring [7, 8].
Application of cultured keratinocytes appears to promote healthy granulation tissue formation within the wound bed. The graft, when applied as a sheet, act as an occlusive dressing, preventing wound dehydration and maintaining a moist environment. The majority of evidence suggests that cultured epidermal allografts do not survive indefinitely after transplantation [10]. Their brief contact with the wound, however, seems sufficient to stimulate re- epithelialization, particularly when dermal tissue is present in the wound bed. This may be due to the release of growth factors by keratinocytes which may favourably influence wound healing. In addition to this, there is a release of several growth factors by keratinocytes that promote wound healing [11]. It is known that cultured keratinocytes release various factors that enhance the growth of other cells in vitro including keratinocytes, fibroblasts, and melanocytes. Identified factors include interleukin-1, other interleukins, and transforming growth factor-alpha.
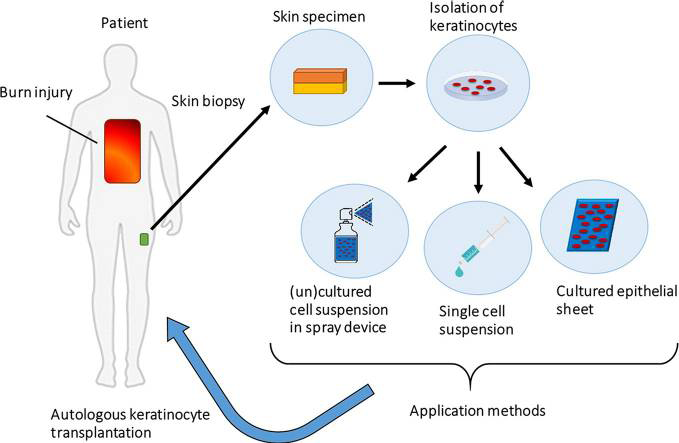
These keratinocytes may be autologous or allogenic in origin. These cells are separated from skin graft by using trypsin or other methods. After separation, these are cultured in appropriate media to form a sheet. These sheets are used as graft to cover the wound. In our case, we have used autologous non-cultured, non trypsinised keratinocytes cells to promote the healing. We observed favourable result in terms of formation of healthy granulation tissue and rapid epithelialization of the wound from the margins [12].
The mechanism of action by which sucralfate helps in wound healing is multifaceted. Sucralfate increases growth factors bioavailability and prostaglandins and decreases the production of oxygen free radicals synthesis, thus potentiating angiogenesis, granulation tissue, and re- epithelialization. It increases the bioavailability of growth factors, particularly of FGF. It increases the production of prostaglandins and inhibits oxygen free radicals [13].
In our case, we have used Sucralfate cream locally and non-cultured keratinocyte graft over the second degree scald burns. We have observed rapid healing in terms of reduction in necrotic tissue and faster appearance of granulation tissue along with epithelialization of the wound. As the commercially available sucralfate cream also contains xylocaine that helps in pain relief also. No adverse effect was noted with its application.
Due to small sample size statistical analysis could not be done. A randomized control study with adequate sample size with wounds of different etiology is desirable to substantiate the results.
Conclusion
The application of non-cultured keratinocyte graft with sucralfate in the treatment of second degree scald burns has been proven effective in this study. It hastens the overall healing time of second degree superficial and deep wound to within a week. Thus minimizing the total hospital stay and infection rates.
References
-
Wlaschek M, Kochanek KS (2005) Oxidative Stress in Chronic Venous Leg Ulcers. Wound Repair and Regeneration 13(5): 452-461.
-
Jackson PC, Hardwicke J, Bamford A, Nightingale P, Wilson Y, et al. (2014) Revised Estimates of Mortality from the Birmingham Burn Centre, 2001-2010: A Continuing Analysis Over 65 Years. Ann Surg 259(5): 979-984.
-
Banati A, Chowdhury SR, Mazumder S (2001) Topical Use of Sucralfate Cream in Second and Third Degree Burns. Burns 27(5): 465-469.
-
Tsakayannis D, Li WW, Razvi S, Spirito N (1994) Sucralfate and Chronic Venous Stasis Ulcers. Lancet 343(8894): 424-425.
-
Tumino G, Masuelli L, Bei R, Simonelli L, Santoro A, et al. (2008) Topical treatment of chronic venous ulcers with sucralfate: A placebo controlled randomized study. Int J Mol Med 22(1): 17-23.
-
Gauthier Y, Benzekri L (2012) Non-Cultured Epidermal Suspension in Vitiligo: From Laboratory to Clinic. Indian J Dermatol Venereol Leprol 78(1): 59-63.
-
Pastar I, Stojadinovic O, Yin NC, Ramirez H, Nusbaum AG, et al. (2014) Epithelialization in Wound Healing: A Comprehensive Review. Adv Wound Care 3(7): 445-464.
-
Levy V, Lindon C, Zheng Y, Harfe BD, Morgan BA (2007) Epidermal Stem Cells Arise from the Hair Follicle After Wounding. FASEB J 21(7): 1358-1366.
-
Schultz G, Sibbald G, Falanga V, Ayello EA, Dowsett C, et al. (2003) Wound Bed Preparation: A Systematic Approach to Wound Management. Wound Regen 11(S1): S1-S28.
-
Shukla VK, Tiwary SK, Barnwal S, Gulati AK, Pandey SS (2010) Effect of Autologous Epidermal Cell Suspension Transplantation in Chronic Nonhealing Wounds: A Pilot Study. Can J Surg 53(1): 6-10.
-
Jiang CK, Tomic-Canic M, Lucas DJ, Simon M, Blumenberg M (1995) TGF Beta Promotes the Basal Phenotype of Epidermal Keratinocytes: Transcriptional Induction of K#5 And K#14 Keratin Genes. Growth Factors 12(2): 87- 97.
-
Chen P, Parks WC (2009) Role of Matrix Metalloproteinases in Epithelial Migration. J Cell Biochem 108(6): 1233- 1243.
-
Masuelli L, Tumino G, Turriziani M, Modesti A, Bei R (2010) Topical Use of Sucralfate in Epithelial Wound Healing: Clinical Evidence and Molecular Mechanisms of Action. Recent Patents on Inflammation & Allergy Drug Discovery 4(1): 25-36.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey