Pressure Wound Healing The Three Pillar Protocol
In the "steady state", wounds show simultaneous granulation tissue deposition and autolysis activity associated with all three zones. They are the center, edge, and neocicatrix. At any given time, there is phagocytosis, epithelization, angiogenesis, matrix synthesis, contraction and remodeling. Multiple cell types under the influence of cytokines, growth factors and matrix metalloproteinases (MMPs) are orchestrated to clean up necrotic tissue, only then will there be a “fill in” of granulation tissue and epithelialization of the surface. The task of the wound care nurse is to understand/support healing activity and eliminate the perpetuating elements sustaining inflammation. Biofilm must be removed.
Introduction
To the wound care nurse, the successful practice of wound healing is not isolated to selection of a dressing, device, or surgical protocol. Rather it is a balance between three independent but interdependent variables. In 2013 Medicare called for innovative protocols to improve healing and cost efficacy. Relying on decades of experience. THE THREE PILLAR PROTOCOL was developed. The first pillar is offloading pressure. The second is to address skin failure due to micronutrient deficiency, which is often overlooked but easily diagnosed at the bedside. For example, Vitamin C deficiency produces collagen deficits resulting in thin dermis, purpura and skin tears. It has been observed that all patients with pressure wounds have scurvy first. Vitamin C is required for collagen maintenance and wound healing. Third, peri wound tissues must be cleared of necrotic and bacteria laden biofilm which produces proinflammatory cytokines and stalls macrophages and fibroblasts healing activity.
Three Pillar Protocol Efficacies
Case Presentations
Case 1: When the Three Pillar Protocol was begun a nursing home with 245 beds had 56 patients with over 250 wounds. A wound care nurse was using state of the art techniques. The protocol did not however include the bed side diagnosis (pillar II) of key micro nutrient deficiencies and therapeutic nutrient supplementation. Neither did it include weekly serial conservative bedside debridement (pillar III) i.e., the mechanical removal of necrotic tissue by a physician using surgical instruments or curettage of soupy biofilm during regular dressing changes by the wound care nurse. Effective relief was inconsistent. Outcome was poor.
One to two weeks following implementation of the Three Pillar Protocol necrotic debris, odor and drainage was replaced by clean and dry peri wound skin and healthy wound granulation tissue. Unless the patient was at the end stage of life or blood flow severely compromised, wounds healed or routinely made progress toward healing. By the 20th week, following implementation of the Three Pillar Protocol, the number of patients with wounds decreased from 56 to 24. Total wound count decreased from 250 to 46 healing wounds.
These improvements in outcome were without the need for topical enzymatic treatments or the transport of the patient to the hospital for flaps or debridement, hyperbaric oxygen or use of vacuum devices, cultures/antibiotics, even if bone was exposed.
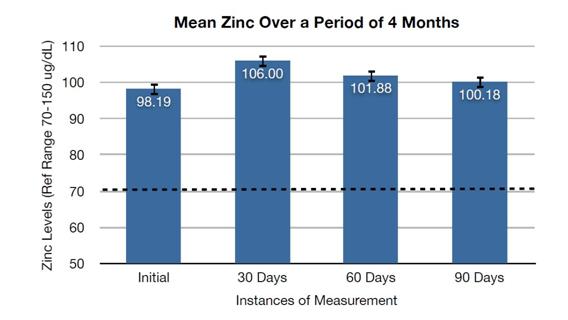
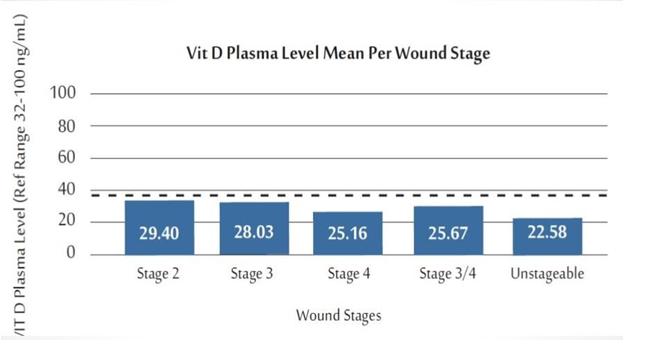
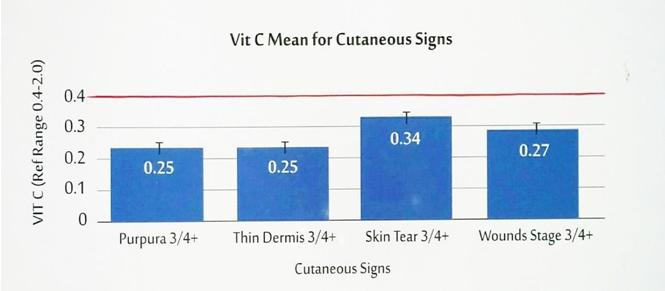
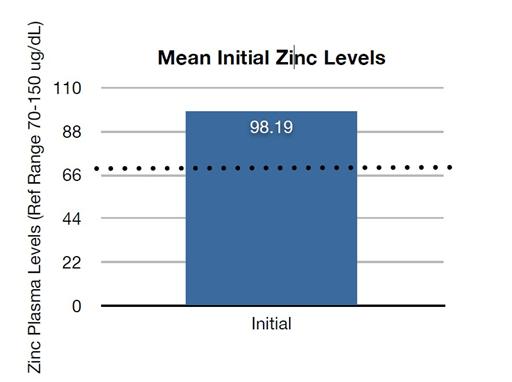
It was found that one critical aspect of the second pillar, nutrition, had been entirely overlooked. i.e., the need for micro nutrient supplementation despite the cutaneous signs of obvious vitamin and zinc deficiencies found on physical exam. Serum/plasma was routinely sent for analysis of vitamin C, D3 and zinc at the time of consult (Figures 1-3). The lab results confirmed deficiencies diagnosed on physical exam. For example, in patients with a transparent dermis on the dorsum of the hand, purpura or skin tears, mean plasma vitamin C was below normal. Similar deficiencies in lab values were noted for Vitamin D3 (Figures 4-6). On the other hand, Zinc lab values were consistently found above normal despite the fact that the patients were clinically deficient based on the zinc oral taste test. Hypogusia is a reliable functional test for zinc deficiency. Future work is needed to reconcile why a patient with clinical zinc deficiency will still have a normal serum level (Figure 3). In any case, the full array of cutaneous support micronutrients was started if a pressure wound was present.
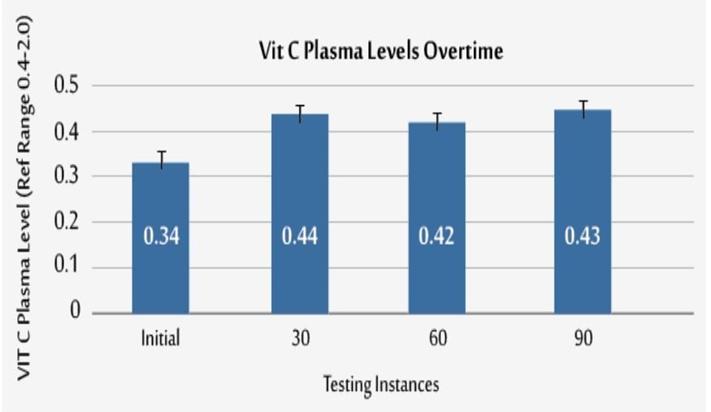
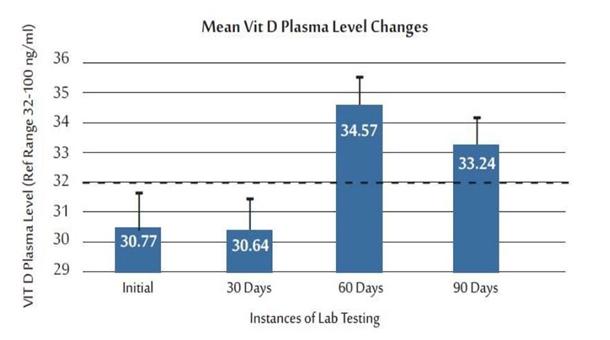
Case 2: The same protocol followed in example 1, except vitamin C, D and zinc levels were measured at the start of therapy 30, 60 and 90 days.
What was discovered was that all patients at the time of wound consult had scurvy, vitamin D deficiency, and hypogusia indicating a zinc deficiency. A vitamin C deficiency is the easiest to diagnose at the bedside because the physical signs are easy to recognize dermal atrophy, purpura, and skin tears.
Recall, skin failure was present at the time of initial wound care consult for patients with pressure wounds. This answers the question for wound care like: What comes first, the chicken or the egg? Answer: the patient develops skin failure due to micronutrient deficiencies before pressure wound develops.
Results
In five months following initiation of this protocol, there was a consistent reduction in drainage and odor across the board. The number of treatments/dressings the wound care nurse stocked decreased from over a dozen to four. As part of the three pillars principles, serial conservative bed side debridement by the physician and regular biofilm curettage by the nurse was employed. Gauze dressing was replaced with non-adhesive dressings because of the observation that placing any form of cotton on the wound seems to create a foreign body reaction. As a result, drainage and odor was reduced, there was no need for hospital transfer for debridement, grafts, flaps or hyperbaric oxygen therapy and no need for exogenous enzymes, vacuum devices or routine cultures and antibiotics.
Conclusion
The strict adherence and integration of the three basics of pressure ulcer wound care, resulted in superior clinical and economic efficacy.
These articles will describe specifics regarding implementation of each of the three pillars.
The three-pillar protocol represents an organization of thought in planning therapy just as a S.O.A.P. note facilitates organization and communication. Once mastered, this process results in healing wounds, not simply ordering and changing dressings. To be successful, the wound care nurse must be knowledgeable and disciplined, focusing on one pillar at a time when constructing the wound care plan.
Pillar I: Stop the Wounding Process
The wound care RN knows there is a difference between a violent traumatic wound and a pressure wound. The first is over in an instant and the victim is usually not malnourished. However, in the nursing home pressure wound patients are malnourished, and scurvy along with its associated collagen deficit is the rule, not the exception. Under these conditions, constant pressure from objects will cause capillary collapse, microvascular thrombosis and injury. Further, a pressure wound cannot heal if there is continued pressure, even if that pressure is from an expensive seat or inflatable overlay. Once a successful system of wound flotation is devised it must be constantly checked for competence. To get universal acceptance and implementation of this very simple concept can amount to the wound care nurse changing the culture of the wound care physician, institution and CNA. It is not easy. "We know that a person cannot be weightless and so cannot be completely free of pressure" is quote from the National Pressure Ulcer Advisory Panel (NPUAP) Support Surface Standards Initiative's, Terms and Definitions Related to Support Surfaces report [1, 2, 3]. However, there are circumstances where pressure persists due to misapplication of a device. For example, even if custom foam seating has been carved for a contracted patient, leaving the patient in the transfer sling will tighten across the wound when the patient is placed on the chair, compromise circulation and cause continued pressure.
The NPUAP report listed terms and materials used in the ever changing field of designs and devices. After the first test for pressure relief (demonstrable space between the wound and the offending surface) has been met, the wound should begin healing if Pillar II, III detailed below are adhered to.
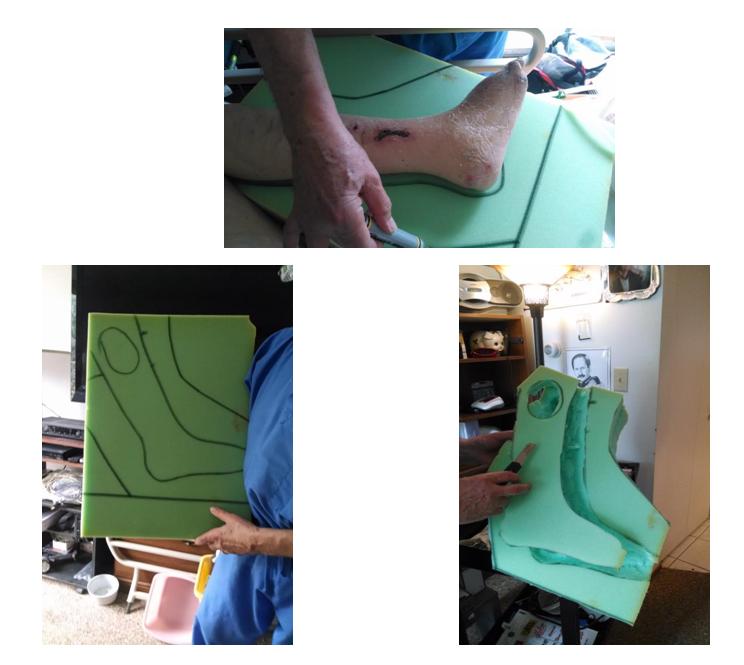
When commercially available devices fail, it is time for the wound care nurse to be creative. The commonly used 6" foam mattress, which is the standard in nursing homes, or 4” memory foam available at large retail stores, have proven to be excellent and inexpensive material for custom carving pressure relief devices. The material used meets health and fire codes.
Overemphasis of the "turning schedule" may distract from an effective analysis of Pillar I effective prevention. The RN and her CNA must be sure that the bandaged wound is separated from pressure and not just simply add a pillow as is often ordered. It is not unusual to find the wound placed on a pillow creating more compression force on the wound rather the pressure relief.
Pressure Redistribution over the Back. The Custom Carved Mattress
When pressure relief over an unusual wound on the back or buttock, especially in the contracted patient is required, custom carving foam to float the wound is indicated. The first consideration however is to use surfaces that are designed to prevent uneven pressure over a bony excrescence such as the sacrum, hips or protruding vertebral body spines etc. As soon as a Stage I wound is observed the cause must be effectively corrected. This can be accomplished by replacing the standard mattress with one designed for pressure distribution or use of overlays. They are least expensive and often rated by the manufacturer as certified for the prevention of Stage I and II pressure wounds.
There are air mattresses that automatically rotate the patient. When working properly they are superior and do not require the usual turning schedule. A word of caution. As the device gets more complex, the CNAs attention to the basics may decrease. The nurse's CNA becomes the most important member of the wound care team. The air pump settings are to be constantly checked to avoid over or under inflation. It is not just deployment of the device, rather it is constant confirmation it is working. For example: If a bed of healthy granulation tissue now shows the telltale purplish blotch of capillary thrombosis, it was caused by pressure. This requires action by the wound care nurse to solve the problem.
Pressure Redistribution, the Seat
Adequate pressure relief while sitting is frequently overlooked. When transferring a patient with a sacral wound from a flotation mattress to chair, a cushion that has a space that floats the sacrum is essential. Specialized cushions are always required for meals, social activities and above all, dialysis. For example, an inexpensive cushion with a “V” cut into the back is available at large chain pharmacies (Figure 7). If an additional overlay such as a pillow case is used, it must be tucked into the “V” defect in the cushion in order to prevent it tightening causing pressure when the patient is in the sitting position. Never use a Turkish towel, it holds heat and moisture. The seat cushion needs to be checked during rounds as a routine part of the daily clinical visit.

The Gold Standard of Pillar I Is Pressure Elimination
The Guideline Technical Report published by the Health and Human Services of the U.S. Government Treating Pressure Ulcers, Volume 1 restated the simple principle: "Avoid positioning patients on a pressure ulcer. Use positioning devices to raise a pressure ulcer off the support surface [4, 5]." As the ideal, there should be a demonstrable space between the wound and an offending surface. This is possible where the wounds are on heels, feet and ankles, hands and elbows, where anatomy vs mattress or a kissing ulcer due to limb contractures as one limb crushes the skin of adjacent anatomy. Continued wound contact cannot be tolerated. Sacral, buttock and ischial wounds are caused when the patient is in the sitting position. Always check for effectiveness. Ordering a pressure relieving device does not mean it will be adequate for an individual patient.
Pressure Relief of Wounds on Heels and Feet
Commercially available devices are sometimes advertised as "one size fits all". However, they generally fail when used for the foot or contracted knee. Tightening the hook and mesh straps across the front of the boot can cause wounds. Most of these boot like devices do not protect the lateral boney prominences of the foot/ankle in patients that are chronically in the frog leg position. Figure 8 illustrates an example of a custom carved device used for these wounds.
The AHCPR guidelines “Prevention and Treatment of Pressure Wounds” recommends pillows. Unfortunately, they rarely stay in place. The calf, not the foot, must be is rested on a surface that is neither too soft allowing the heel to sink nor too firm causing wedge pressure to the Achiles/distal calf encouraging foot drop. The wound must float. Placing the heels on the pillow continues pressure and is to be avoided. Pillar II, Nutrition focuses on micronutrients rather than macronutrients.
Healing Pressure Wounds – Micronutrient Deficiencies
Pillar II: Nutrition
Introduction
A physical diagnosis of micronutrient deficiencies which cause skin failure and predispose to pressure wounds can be easily made at the bedside.
Malnutrition is traditionally described as a deficiency of both the somatic and visceral protein compartments. The macro nutrients are carbohydrate, fat and protein, which sustain the somatic protein compartment consisting largely of muscle, skin and bones. The visceral protein compartment is comprised of all organs, circulating blood and the immune system.
To overlook the role of micronutrients (vitamins and minerals) when it comes to skin failure is a common error. Micronutrient malnutrition precedes skin failure and a pressure wound [6]. Therefore, the wound care nurse must be ready to defend and refute inappropriate comments such as “all that you are doing is making expensive urine”. Nothing could be further from the truth.
The wound care nurse must play the role of teacher as the following illustrates.
Function, Diagnosis, and Supplementation of Micro Nutrients in Patients with Deficiencies and Pressure Wounds
Diagnosis of Oral and Cutaneous Signs of Vitamin B, C, D, Zinc and Fatty Acid Deficiencies Can Be Made At the Bedside
Images of glossitis (B deficiencies), magenta tongue and angular stomatitis (B2), transparent plastic wrap skin, purpura and skin tears (C, Chronic Scurvy), and superficial "thin ice" epidermal cracking with fine wrinkling / crape paper appearance (B3, Pellagra). Also, "snow flake" dandruff on the extremities starting with the lower legs (essential fatty acid), and the Zinc Taste Test (a functional test for zinc deficiency) are presented. (Figures 8-14) [7].
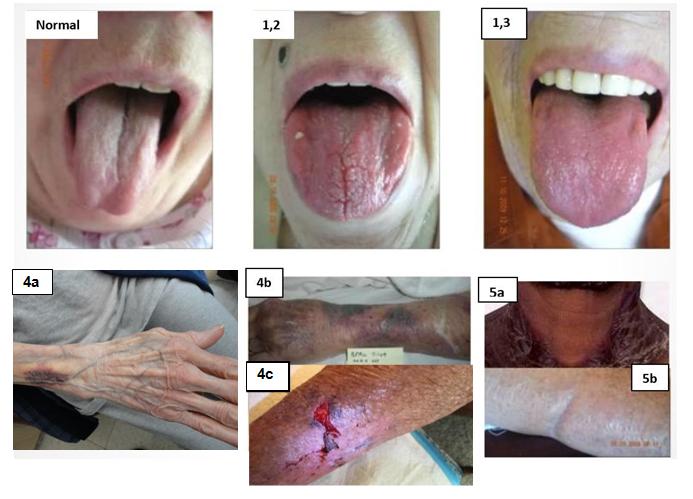

For comparison, actinic keratosis is always associated with findings on the face, the effect of overexposure to the sun. A bruise does not show any dermal atrophy, skin tears or the distribution of purpura.


Water soluable vitamins: The B vitamins Vitamin B3 – Pellagra. A sign of vitamin B3 deficiency observed at the bed side is fine checking or cracking of thin skin. They are subtle at first and look something like the water between floating islands of thin ice as a pond thaws in the spring. Exposure to UV light causes these spaces to turn cherry red. The classic symptoms are dermatitis, dementia, diarrhea, and death. (The four Ds). The dermatitis can be quite dramatic including alligator skin hyperkeratosis as is frequently illustrated in text books showing the sun exposed neck line with skin changes seen in farmers with a B3 deficiency. Poor wound healing is listed as one of the features of Pellagra.
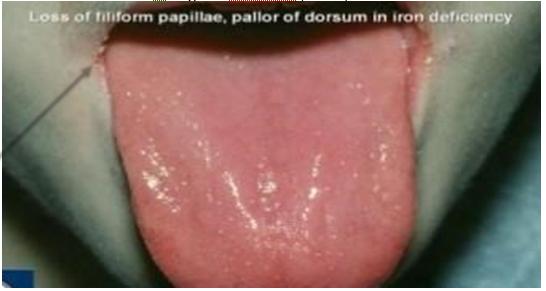
It should not be confused with the flaking of an essential fatty acid deficiency which often co presents with the hyperkeratosis of Pellagra. When both are present there is a more dramatic scaling skin appearance than each alone [8]. • Recommendation: Niacinamide 250 mg BID. Except for B12 and B6, B vitamins are water soluble and are excreted in the urine with no appreciable storage [9]. This means that, along with vitamin C they must be ingested every day. They generally function as coenzymes and cofactors in the cytochrome oxidase pathway producing ATP [10]. ATP is the energy currency used to physically accomplish everything from muscle contraction to protein synthesis. A deficiency will first negatively affect rapidly metabolizing tissues with high cellular turnover rates such as the blood (especially the white cells), and gastrointestinal tract, the kidney and brain [11]. If a patient has an under lying condition involving these organs, the danger is under, not over supplementation. Overdose is difficult to achieve as urine excretion of Niacinamide is prompt. Diagnosis on physical exam: Glossitis. Slightly differing presentations of glossitis are the hallmark of all the B vitamin deficiencies. Findings can overlap given that in malnourished patients all micronutrients have been under fed.
The tongue is normally covered with villi giving it a velvety appearance. Lingular villi are long enough to hold a small saliva froth causing a slight whitish look. The healthy tongue also has a hint of a cyanotic or venous blood hue. B deficiencies cause atrophy of the villi and flattening of the velvety surface. It is replaced by a smooth surface and a reddish color depending on the predominant B Vitamin causing the deficit. For example, B2, Riboflavin, produces a magenta colored flank steak appearing surface and occasionally angular stomatitis or cracks at the corners of the lips also known as chelitis [12].
- Recommendation: B Vitamin Complex as supplied by one multivitamin tablet BID plus a high potency B complex tablet. Fat Soluble Vitamins- Diagnosis based on physical diagnosis. Except for para follicular hyperkeratosis, a finding of a Vitamin A deficiency, physical diagnosis of fat soluble deficiencies cannot be made on bedside physical exam [13]. Nevertheless, vitamins A, D, E and K all play a role in skin and bone metabolism [14, 15, 16, 17]. Although stored, it is likely that the depleted reserves in a malnourished patient will serve as a buffer against toxicity.
- Recommendation: One multivitamin PO Bid. Vitamin D: Vitamin D has captured the interest of nutritionists over the past decade. It is no longer relegated to calcium absorption and bone health as it has been shown to do much more from enhancing physical strength to being associated with a significant decrease in the incidence of various cancers [18].
Vitamin D could be considered a hormone as well as a vitamin in that it is also synthesized in skin exposed to sun light. For pressure ulcer patients, their primary infirmity often precludes exposure to sun light. Further, the final step of conversion of vitamin D2 to vitamin D3, calcitriol, is carried out in the kidney. Therefore, in addition to diet and sun exposure, renal health is essential [19].
The skin has an innate antimicrobial function that plays a role in wound healing which involves vitamin D. In addition to activating numerous genes involved in wound healing, vitamin D activates over 2,000 genes, which is about 10% of the genome [20]. To heal the wound, genome control of cell proliferation and differentiation is critical. Calcitriol is a phospholipid that crosses the cell membrane and enters the nucleus. There it binds to vitamin D receptors and initiates gene expression directly involved in local immune function as well as cell differentiation [21]. For example after wounding, vitamin D increases the expression of genes in the keratinocyte which code for antimicrobial receptors and the antimicrobial peptide cathelicidin. Vitamin D3 assists in the eradication of infectious microbes [22].
Following injury, keratinocytes accumulate around the wound. Keratinocytes convert vitamin D2 to the active form vitamin D3, calcitriol. The increased D3 available at the wound then activates vitamin D receptors. This then triggers detection of microbes via activation of genes CD14 and TRL2 [23].
In addition to the antimicrobial effect, wound healing is enhanced by cathelicidins role in angiogenesis and epithelization. There is rapidly emerging science for the role of vitamin D in health and disease prevention. Overdosing is not an issue. Note: Spending 20 minutes at the beach in a swim suit will produce 10,000 IU of vitamin D [24]. • Recommendation: Vitamin D3, 2000 IU, BID, 1,25-di- OH Calcitriol (32.0 - 100 ng/dl) Essential Fatty Acid Deficiency (Efad): Both omega 6 and omega 3 fatty acids are essential as a supplement because they cannot be synthesized. These fatty acids are concentrated in the cell membrane of every tissue in the bodyand there is emerging literature supporting their role in wound healing [25].
All cells have an inner and outer cell membrane, a double wall made of protein. The ratio of omega 3 to omega 6 in the cell wall is directly related to their dietary intake [26].
For example, eating red meat will provide a higher ratio of omega 6 where eating fish will provide omega 3. But, as with humans, neither cows nor fish can make EFAs. EFAs are produced by photosynthesis and are part of the food chain. When energy of the sun strikes water, via photosynthesis, carbon, hydrogen and oxygen are taken up and synthesized into omega 3 by algae. On land, photosynthesis in vegetables such as corn produce a high percent of omega 6. Forty percent of corn oil is omega 6 [27].
Following stress, omega 3 and omega 6 are converted into prostaglandins, leukotrienes and thromboxane. These second messengers govern the degree of the response to the stress with omega 3 causing PGE1, LT5 series and TxA3 which are anti-inflammatory. On the other hand, omega 6 forms PGE2, LT4 series and TxA2 which are pro inflammatory.
- Diagnosis on physical exam: Gross flaking of skin is present, usually starting with the lower extremity, best seen along the anterior shin. Simply rubbing the epidermis will release dry material that resembles snowflakes as it settles on the sheets.
- Recommendation: Concentrated fish oil, 1 gm gel capsule BID. Be sure that the fish oil is guaranteed free of mercury and pesticide contamination. The agribusiness uses pesticides and the factory manufacturing business uses mercury which find their way into rivers and then into the ocean. The cleanest fish oil is from the North Sea where neither industry flourishes. Fish caught 25 km off shore are safe. The oil should not have a fishy taste or smell. If it does, it is rancid and should be returned to the vendor for a fresh supply. Omega 3 is an antioxidant, but consuming rancid fish oil does more harm than good.
Special Role of Vitamin C, Zinc, Glucosamine/Chondroiten and D3-
Vitamin C: Chronic vitamin C undernutrition is associated with a depletion of total body collagen. Collagen is one third of all the formed protein in the body [28]. Atrophy of the dermis and the media of arterioles is a result easily seen on physical exam [29]. All proteins in the body are constantly being made and degraded. This is a normal process called protein turnover. For example, the result of not re synthesizing collagen following its natural degradation in the dermis is a loss of mechanical "push back" or resistance to external force. When chronic scurvy is present, clotting of dermal capillary vessels occurs at pressures below those necessary to create a Stage I lesion in normally nourished individual [30, 31].
Vitamin C is a water-soluble vitamin with no storage. Except for humans and the guinea pig, all other mammals can synthesize Vitamin C from glucose [32]. In experiments using rats, stress will induce increased production of Vitamin C. If the rat weighed 70 kg the increase in endogenous vitamin C production would be 10 gm per day. Not using a human or guinea pig model is therefore problematic in wound healing studies.
For the patient with the chronic wound, necessity to supplement Vitamin C rests on the fact that Vitamin C is required for collagen synthesis. There are numerous other essential roles for the vitamin in preventing oral, ophthalmic, musculoskeletal, cardiac, gastrointestinal pathologies which on occasion cause death [33]. The discussion of Vitamin C’s role in health and metabolism is however beyond the scope of this paper.
In order to heal a wound, fibroblasts must produce collagen. This is a relatively complicated process which requires an abundant supply of the amino acids proline and lysine. The microscopic structure of collagen literally looks like twine with cords wrapped around each other and connected by cross links. Cross linking of strands forms a triple helix twisting first to the left then right and back again. This architecture gives a strand of collagen strength greater than a steel wire of the same diameter. However, it is not proline and lysine that cross links and twists the strands. Rather, it is hydroxyproline and hydroxylysine. Vitamin C is the hydroxylase adding - OH to proline and lysine facilitating cross linking and twisting [34].
Because there are no stores of Vitamin C, a diet deficient in the daily requirement will fail to support the normal replacement of collagen turnover. A small daily deficiency will inevitably result in a clinically significant total body collagen deficit over time. Day by day and year by year chronic scurvy evolves. The acute form is described as the 4 Hs i.e.: hemorrhage, hyperkeratosis, hypochondriasis and hematologic abnormalities. These were described in sailors on long voyages. However, the chronic form common to the elderly presents as skin dermis and capillary wall thinning. This can be observed at the bed side and is the major reason for skin failure leading to pressure wounds. The wound care nurse can readily observe the signs of Vitamin C and Zinc deficiencies on admission or at the time of wound consult.
When there is a Stage III or IV pressure ulcer, granulation tissue must be synthesized to fill the defect. These defects can require tens of grams of tissue. This in turn will require a Vitamin C supplement well above the 60 mg per day recommended dose.
Despite the fact that it will take months to heal large Stage III and IV wounds, the positive effect of Vitamin C supplementation can be seen in 24 to 48 hours. This can be observed in skin tears where the defect will scab over and not require topical treatment beyond 5 to 7 days. The skin tear is a sign of a Vitamin C deficiency, not the disease. • Physical exam for signs of chronic scurvy: The wound care nurse should inspect the skin on the dorsum of the hand for dermal atrophy and/or observe the hands and arms for purpura indicating chronic collagen wasting causing capillary fragility. Chronic Vitamin C deficiency can become so severe that the extensor tendons and the interosseous venous plexus can be seen beneath a transparent epidermis. This sign is described as "clear plastic wrap" skin. It is 4+ dermal wasting.
In example 2 routine testing for micronutrient levels was assayed at the time of consult and repeated monthly (Figure 1). It should be cautioned that a single lab value amounts to a snap shot of what was eaten within the past few hours and has nothing to do with overall collagen status of the patient. Recommendation 500 mg Vitamin C BID Normal range of Vitamin C (0.4 - 2.0 mg/dl).
Zinc: Martix metalloprotinases (MMPs) tissue inhibitor metalloproteinases (TIMPs), are under gene control. In wounds, they turn on and off enzymes to digest necrotic collagen and other proteinaceous debris. They are the ever-present enzymes of healing, able to digest every protein found in the extra cellular matrix. They have structural similarities and were originally classed by substrate specificity such as collagenases, gelatinases, stromolysins and basement membrane type metalloproteinases. They are no longer classified according to substrate activity since 15 of the 20 MMPs found in a pressure wound have collagenase activity. They are involved in everything from embryo development to cancer metastasis.
As an example, a specific MMP is required to digest the anchors of the keratinocyte allowing the epithelial cell to bind the leading edge on the granulation tissue border to leap frog into the lead position. The MMP is blocked by its TIMP allowing it to form an anchor [35]. Their role is tightly regulated in every aspect of wound healing. Under gene control they respond to signaling molecules such as growth factors produced by platelets and macrophages populating a clean granulating wound. MMPs and TIMPs simultaneously move a healing wound in many directions with interlocking parts. The only constant is that both require zinc. Clearly, there is no need to apply external collagenase when 15 natural MMPs simply require an oral zinc supplement.
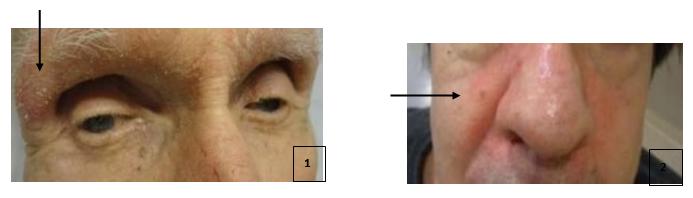
Because autolysis of necrotic protein is an ongoing function of MMPs, debridement should be limited to the surgical removal of nonviable tissue but not include excision of surrounding healthy tissue. It is unnecessary and risks serious bleeding. If zinc is supplemented, the rim and thin base of necrotic tissue left in the wound following scissor debridement will undergo natural autolysis. Follow-up superficial mechanical removal using A zinc rash is observed on the face. It is a reddish scaly patch of the lateral eye brows and nasolabial folds. Acrodermatitis enteropathica is a congenital zinc malabsorption condition where the zinc rash is commonly seen (Figure 15). Adequate oral zinc supplementation clears the rash.
saline, non-gauze wipe such as a paper towel, and a tongue blade split longitudinally, or a disposable curette removes the remaining debris and above all biofilm. Within a short period of time, there is healthy granulation, no drainage, odor or pain. To repeat for emphasis: a scalpel is not recommended as a debriding tool. A scalpel is for incision. Biofilm and autolyzed debris are best removed using the curettage technique. Using a scalpel is dangerous.
Zinc is the most abundant trace mineral in the human body. It plays a pivotal role in approximately 300 enzyme reactions and its requirement for wound healing has been established [36, 37, 38, 39, 40, 41]. Zinc is also a powerful antioxidant and plays a role in skin integrity. Zinc is present in all organs, tissues and fluids of the body. Twenty percent of total body zinc is in the skin and its appendages. A review of all the roles zinc plays in health and healing is beyond the scope of this paper. As a testament to Zinc’s importance, scientists in the European Union have formed a group called the Zincage Study [42]. Their findings make testing for a zinc deficiency and recommending supplementation a wise clinical decision for all patients but especially in the pressure ulcer population [39].
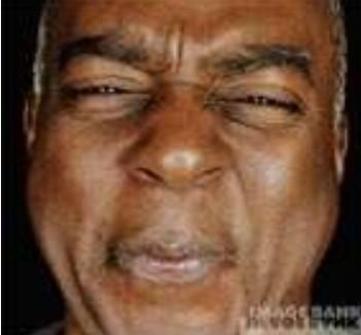
Until 1974 zinc was considered non-essential. Zinc toxicity is difficult to achieve because to an individual who does not have a zinc deficiency zinc has a vial taste and causes gastrointestinal distress. The patient will refuse to take it. If a zinc deficiency is present, zinc is tasteless. • Diagnosis
A Zinc Taste Test (ZTT) is a diagnostic functional test. Two ml of a 0.1% solution of zinc sulfate is poured from a bottle and given to a patient who is asked to hold the solution in their mouth for one minute. Within seconds, individuals who are not zinc deficient taste its rather unpleasant flavor and make a wry expression. Or, within 30 seconds an unpleasant metallic taste is reported.
Hypogusia is a term that describes the inability to taste Zinc. As part of the wound consult in addition to plasma vitamin C and D, serum Zinc levels were routinely measured for confirmation of deficiency diagnosed by the Zinc Taste Test (ZTT). Two hundred and twenty mg of zinc sulfate provides 51 mg of zinc.
A Simple and Accurate Functional Test for Zinc Deficiency
The Zinc Tally Test is cumbersome. Instead of using a bottle of solution a simple and accurate test for zinc deficiency is to spray the oral mucosa with two puffs of a zinc solution using an over the counter cold remedy. As with the Talley Test, a zinc deficiency is diagnosed if the subject does not develop a wry facial expression within seconds of oral Zicam® Spray. The two methods are equivalent. A zinc taste test has become part of a wound care consult. It was noted thatall patients with glossitis were zinc deficient. However, patients on a daily multivitamin or tube feeding usually do not have glossitis but can have a positive ZTT.
In addition, no patient receiving Zinc supplements recovered from hypogusia despite having normal serum values. Zinc is absorbed and excreted by the gut [43]. The simplicity of the oral spray ZTT make it an important part of a patient’s work up. Recommendation Zinc sulfate 220 mg PO BID (= 50mg of Zinc) Normal range (70 - 150 ug/dl) 1.1.1. Glucosamine/Chondroitin: Glucosamine and chondroitin sulfate are key nutrients in the formation and maintenance of glycosaminoglycans (GAG proteins) in the extra cellular matrix. This is the space, including the basement membrane of opposing cells, which connect one budding vascular component of granulation tissue to another [44]. This space is filled with a network of suspended mesh like elements which anchor cells, regulate intercellular communication, and produce a wide range of growth factors essential to healing. In addition to being a local depot for cell growth signal molecules, it segregates one tissue from another which is essential for wound healing [45, 46].
The formation of GAGs requires Vitamin C and glucosamine. Glucosamine is a sulfur containing amino acid and is the major constituent in chondroitin. In addition, to other linear molecules, heparin sulfate and keratin sulfate comprise the interlocking mesh. Their negative surface charges attract sodium which holds water. Along with albumin, which similarly holds water they form the gel of the gel sol matrix [47]. GAGs glue together the fibrous elements found in the ECM in all tissues of the body. These include elastin, fibronectin and laminin as well as collagen. Sixty percent of total body albumin is in this space.
- Diagnosis: Presume GAG deficiency if there are signs of a Vitamin C deficiency.
- Recommendation: Give approximately 1000 mg glucosamine, chondroitin 600 mg, MSM 250 mg BID.
Pillar II Conclusion
The details presented in Pillar II equip a wound care nurse with science when giving adequate doses of micronutrients to heal a wound. Micronutrient deficiencies are a common cause for stalling the healing process.
A nutrition assessment as practiced by clinical dietitians traditionally focuses on determining the visceral and somatic protein status. But it neglects identification of even obvious signs of micro nutrient deficiencies. It is predominently micronutrient deficiencies that cause skin failure that precedes the wound. To date, even the required 48hour admission skin assessment by a nurse overlooks easily recognized signs of Scurvy (Vitamin C), Pellagra (Vitamin B3) essential fatty acid deficiencies (omega 3 and 6) and zinc deficiency as presented here. It will be necessary for the wound care nurse to teach Physical Diagnosis related to the oral and cutaneous sings of micro nutrient deficiencies as was recommended in AHCP but universally neglected [11]. Upon diagnosis of a micronutrient deficiency the full panel of supplements needs to be started. The standard over the counter supplement is the minimum to prevent a deficiency in healthy individuals (Figure 16). In unpublished observations by the author, all patients with pressure wounds have Scurvy at the time of consult. And, if supplements are started when signs of Scurvy are noted on admission skin assessment, pressure wounds do not develop.

“Mega doses", as they are called by some, are in line with good clinical judgment given their lack of toxicity, and the size of the deficit. It is important to realize that the under nutrition which caused the deficit has in some cases depleted total body structural components as well as stores. They represent an accumulating deterioration of structure/organ/function. Proper and aggressive supplementation up regulates protein synthesis aimed at repair.
In Pillars I and II errors in management are obvious. A pressure wound cannot heal if there is continued pressure and it cannot heal if there is an inability to synthesize collagen.
Healing Pressure Wounds – Dressing Protocol
Pillar III: Wound Care, Provide A Salubrious Dressing
Introduction
Healing is classically divided into three overlapping phases: 1) inflammatory 2) proliferative and 3) remodeling [48, 49, 50, 51, 52]. These three phases integrate via gene coordination. Involved in this process is chemotaxis, phagocytosis, neocollagenesis, extracellular matrix (ECM) degradation of collagen, elastin, fibronectin, laminin the basement membrane and every other protein found in the ECM. Finally, remodeling guides angiogenesis and epithelization. New contributions to basic science regarding events at the genetic and molecular level are providing a better understanding of the phases which create the salubrious dressing.
The pressure ulcer and other chronic wounds, at some point, been considered “suspended in the inflammatory phase”. Note: pro inflammatory cytokines are abundant in the slime or pancake batter like biofilm. They thwart the healing activity of macrophages and fibroblasts. In fact, the wound care nurse has probably observed a reversal of healing tissue associated with an episode of severe sepsis.
Biofilm, a Key Impediment to Wound Healing
The colony of bacteria inherent in biofilms release chemical signals that attract polymorphonucleocytes. The associated inflammation produces pain and drainage that has a foul odor. Inflammation is secondary to the release of proinflammatory cytokines, TNF alpha, IL 1, IL 6, IL 8 and IFN gamma which instruct macrophages and platelets to keep their distance until the job of ridding the wound of bacteria and necrotic debris is accomplished. This holds off the required influx of macrophages and platelets which are essential for healing. Macrophages clean remaining debris created by MMPs. They digest all devitalized proteins in the ECM allowing platelets to make collagen and release Transforming Growth Factor Beta, Platelet Derived Growth Factor etc. which initiate cellular healing behavior [53].
Wound Care Protocol Controlling Biofilm
The practice of surgical debridement traces its origin to the wounds of war. It required the surgeon to cut away all tissue that was potentially contaminated by field debris that was forcefully distributed throughout the wound by a penetrating injury. Infection was the most common cause of death from war wounds before the era of antibiotics. This meant cutting and removing layer after layer of injured tissue until the surgeon could see unmolested living tissue, including the bone. As an Army surgeon with active front line field hospital experience answered after being asked what did he do all day he replied: "I made big wounds out of little wounds".
During the American Civil War, the Military Surgeon was nicknamed "saw bones". This is because of the wide use of horses in battle and farming. Horse manure was everywhere. Horse manure commonly contains tetanus spores which are long lived and almost indestructible. The only option to save a wounded soldier's life was to amputate at one point above the site of the wound. A bullet wound to the knee was otherwise 80% fatal.
Unfortunately, even in the era of antibiotics, this philosophy of care has carried over from the field wound to nursing home patient. The policy was to surgically debride devitalized tissue with a scalpel until only viable bleeding material remained. Debriding itself became part of the wounding process. Civil War wound debridement protocols have no place in the management of pressure wounds today.
Two kinds of biofilm can be described: slime or pancake batter like. Biofilm is tenacious requiring mechanical removal. It is a complex aggregation of microorganisms growing on the surface of the wound an surrounding moistened skin. It is an effective defense by bacteria against antibiotics. In contrast to "fixed" biofilm bacteria, planktonic bacteria are free floating [54]. Biofilm is a multi-species cooperative of structural heterogenicity, genetic diversity, and interaction producing an extracellular matrix of polymeric substances including DNA, proteins and polysaccharides [55]. Neither systemic nor topical antibiotics can eradicate these colonies [56]. Biofilms and associated planktonic bacteria are the perfect environment for the development of antibiotic resistance. Despite the practice of culturing planktonic bacteria from the surface of a wound, it is useless and mentioned only to be condemned. It may lead to the ill- advised and inappropriate prescription of antibiotics; a practice known to promote antibiotic resistance.
If a zone of cellulitis develops in tissues around the wound, sharply debride of a small sample for culture. A pressure wound dose not hurt. Hover, cellulitis is accompanied by the three classic signs: tumor, dolor and rubor i.e., swelling, pain and redness [57]. Antibiotic treatment is in order for cellulitis, and not to be ordered for management of the ever-present presence of planktonic bacteria.
A fabric of cotton or silk should be eliminated from dressings. A contaminated silk suture is an illustration. Biofilm forms a suture granuloma, with its tenderness, drainage, redness and odor. In order to heal, this suture must be removed. A contaminated fabric suture potentiates contamination, specially cotton.
All wounds, even in a “sterile surgical field" can be contaminated. A single silk suture placed in a standard surgical "sterile field" will decrease the number of bacteria required to form an abscess by 100,000 organisms [58].
There are a number of ways to remove biofilm. Historically, the first and perhaps the best is Maggot Debridement Therapy (MDT) which was popular until the late 1930s [59]. Maggots eat decaying tissue and bacteria. They activate cell signal molecules to promote granulation tissue synthesis. This begins when a female fly lays its eggs on the dressing. The larvae find their way through the fabric onto the wound. MDT is FDA approved.
Other costlier and time-consuming techniques are mechanical rather than biological. Wet to dry dressings are again mentioned only to be condemned. A wound must never be allowed to dry, and narcotics are often necessary to mitigate severe pain caused by removal of the dry dressing [60].
Vacuum assisted devices work well because biofilm is taken up in the interstisis of the sponge. They are expensive, frequently lose vacuum and may require narcotics for pain during dressing change if the absorbent material dries on to the sponge [61].
There are other devices that use mechanical energy in the form of sound waves or pressurized solutions used to soften and wash away the biofilm. Time and cost can again become an issue.
The least expensive and effective technique is to moisten the wound with an irrigant, split a wooden tongue depressor length wise, scrape the two halves together to remove slivers. This creates an instrument which, along its original sanded edge is "dull" and along its fresh fractured edge is relatively "sharp". At the end is a shape similar to a parrot's beak which is useful for removing collections of biofilm from crevices (Figure 17).

Figure 17 Before: Slough is a biofilm like material consisting of colonies of bacteria and other microorganisms causing inflammation stalling macrophages and fibroblasts.
The serrated blades of disposable picnic knives are also effective. These instruments are used for in a sweeping, windshield wiper motion. This is not debridement. Rather, curettage of biofilm is a valuable step promoting healing and needs to be done regularly.

After: Split tongue blade used to curette pancake batter biofilm and slough.
Dendritic cells are in all tissue facing the external environment (skin and gut lumen). By number, they are most common in the gut where organisms are sampled, and surface antigens transmitted to the lymphatic tissue where T and B cells are programmed. Similarly, dendritic cells in the skin sample the skin’s surface organisms. The pro inflammatory antigens are similarly processed, and stall wound healing. It is prudent to keep the skin around the wound as clean and dry as possible.
Eschar Removal
A hard-leathery dark eschar that has no soft areas, emits no odor or when pressed shows no purulent secretions is a natural dressing. The wound is healing beneath the eschar. Except for occasionally trimming the elevated edges of the cap, simple protection and serial evaluation for signs of infection is in order. If the cap can be maintained until it falls off, there is very little scaring. If removed prior to healing, a larger wound is created which will result in a scar. On a regular basis the evaluation begins by the wound care nurse wiping a finger across the entire surface feeling for softening soft and moisture indicating infection. If present, the eschar is then prepared with a topical antiseptic for excision of the softened cap.
Before practicing conservative serial bedside debridement, other physician should be familiar with techniques to regain homeostasis. These include prolonged direct pressure, hand held battery heat cautery, silver nitrate and the surgical placement of figure of eight suture ligatures.
If debridement privileges are granted to a trained wound care nurse, it is helpful to visualize the example of a room with a ceiling and floor as there is a space between the eschar cap and the tissue beneath. Between this ceiling and floor, one can imagine a room in which there is endogenous enzymatic activity caused by MMPs digests of collagen, elastin and other elements of the ECM. It is a zone of autolysis. It is soupy, painless and bloodless. It is the natural space for safe blunt dissection.
To enter this space, using iris scissors. Choose an upturned point along the undersurface of the eschar at the necrotic/viable border of the skin. Spread and snip the sharp points of the iris scissor until the instrument drops into the liquefied material in the "room". Once in this space, grasp the edge of the eschar with a clamp and apply traction. Now, angle the tips of the curved iris scissor so as to see the tips lifted against the cap from beneath. Keep the dissecting scissors angled up as they are advanced, opened and then pulled back to detach remaining elements of the digest from the undersurface of the cap. When a blunt dissection of the undersurface extends form border to border is complete, the scissors are removed, and the clamp repositioned to grasp the eschar to apply firmer traction. Mayo or other heavy surgical scissors are then used to excise the necrotic tissue, leaving a thin border of black eschar bordering viable skin. The dissection deliberately leaves a millimeter or less of necrotic cap behind to avoid cutting into the dermis. It will bleed (Figures 18 & 19). If bleeding is observed, it is usually controlled with direct pressure and/or cautery.
A dry eschar is a natural dressing, however, if it becomes soft with peripheral secretions that have an odor it must be removed to allow drainage of a contaminated space.

B) Clamp traction preparing for iris scissor dissection beneath the eschar base.
B) Result of 10 months of superficial curettage, maltodextrin and non-adhesive dressing plus supplements described above. The patient had a diverting colostomy 10 years ago, the crater at the 4’Oclock position is his anus.
Super Dilute Surface Antiseptic Solutions
The common irrigating solutions are povidone iodine, chlorhexidine, and bleach (Dakin’s solution). At full strength they prevent healing. However, they can be diluted to 0.9% and retain efficacy without stalling healing. To deal with microbes and facilitate wound healing, the wound and the surrounding area is curettage with super dilute antiseptic solutions.
Chlorhexidine is widely used as a surface cleaner and disinfectant for the skin and wounds. The solution is repeatedly rubbed onto the surrounding skin. The aim is to loosen and remove debris and surface bacteria, which would otherwise be sampled via dendritic cells and initiate an inflammatory response Povidone iodine has been shown most effective in suppressing recurring biofilm. It is also used as a 0.9% solution. After curettage of the biofilm the wound is rinsed with a mist of 0.9% chlorhexidine.
Odor is controlled with a 0.9% bleach solution. This solution is sprayed as needed during the curettage step. A standard Dakin’s is a 25% solution of bleach. Caution, Dakin’s solution will stop both odor and healing.
The Dressing
The dressing, following debridement of necrotic debris and ongoing superficial curettage of biofilm, is a treatment and should do three things simultaneously: 1) Discourage bacterial growth, 2) Stimulate endogenous matrix metalloproteinases, 3) Stimulate the secretion of wound healing signaling molecules. All these appear to be active when materials like maltodextrin powder, collagen or honey derivatives and similar topical treatment dressings are used.
Following surface preparation, there are a growing number of products that promote MMP activity, suppression of biofilm formation and enhanced granulation tissue growth.
These include carbohydrate-based products like honey and dextrans and/or alginates. Whatever is used to create a salubrious environment it is placed on a non-adhesive dressing cut to the size and shape of the wound. Maceration of surrounding skin will occur if the dressing is too large and overlaps on the healthy peri-wound skin surface.
The dressing must stay in place until the next change. To better accomplish this, it might be helpful to clean the surrounding skin with alcohol then apply an adhesive prep. Finally, an adhesive overlay of choice to secure the treatment dressing in place is firmly pressed onto the skin. Soon absorbent pads are no longer necessary. Recall, it is the author's experience that eliminating necrotic debris/biofilm, by curettage and not placing cotton fiber in the wound results in the elimination of secretions and odor. Wound care kits that promote these practices are available.
Conclusion
The lead questions were: Can an effective bedside protocol be devised, which will eliminate trips to the hospital or clinic for OR debridement, grafts, flaps etc.? Can expensive topical agents, such as enzymes, be eliminated? Can the use of expensive non-cotton dressings be replaced in favor of a combination of inexpensive honey, maltodextrin, povidone and collagen? Can the need for wound vacuum devices and hyperbaric oxygen treatments be reduced or bypassed in favor of bedside debridement and biofilm curettage? It is not a floatation device or vitamins by themselves that achieve the desired results. It is not a new dressing or wound manipulation.
An effective wound care protocol requires maximum attention to each of the THREE PILLARS OF HEALING. Given the current "standard of care" practices, if a wound becomes chronic, there may be an omission related to one of these three discrete considerations.
Three Common Types of Errors in Wound Healing
- Failed offloading pressure from the wound.
- Micronutrient deficiency.
- Improper dressing which stimulate an inflammatory response.
A Type I error is the most common. Examples of errors include: the air mattress is left on maximum inflation after a diaper is changed. Or, the patient is not placed on their custom V-cut cushion to float their sacral wound during time in a chair, including meals, therapy and dialysis. And, pillows meant to float the wounded heel are placed under the heel instead of the under the calf and Achilles tendon.
A Type II error is frequently associated with a micro rather than macro nutrient deficiency, despite the fact the patients’ nutritional status is managed by a dietitian. The failure to teach physical diagnosis of the oral and cutaneous signs of micronutrient deficiencies during nursing and dietitian training is tragic. Perhaps the American Dietetic Association should reevaluate its condemnation of vitamin supplements when it comes to seniors or anyone who has a chronic illness with cutaneous signs of deficiencies. A paper has been published which presents the oral and cutaneous signs of micronutrient deficiencies [6]. When assessing the need to supplement Vitamin C and all the other micronutrients for patients with pressure wounds, it should be recognized that deficits have accumulated for months, even years. As a result, the patient now suffers from an accrued structural deficit. Put another way, it is not the vitamin C in today’s meal that counts, rather it is the lack of vitamin C over an extended period of time prior to developing a pressure wound. The deficit is very large. Recall collagen is 30% of all formed protein in the body and 70% of skin. Collagen deficiency caused by a vitamin C deficiency leads to skin failure which precedes a pressure wound.
Likewise, for ZINC, one cannot heal a wound without adequate endogenous availability of ZINC to replenish the consequences of total body depletion i.e., MMPs, immune function and more than 300 enzymes etc.
A Type III error is the use of a dressing that is of little value or in fact is detrimental to healing. Toxic agents such as hydrogen peroxide, undiluted iodophor, Dakin’s
Solution, ant-acids mixed with sugar and other inspirations are to be abandoned.
Avoid placing cotton (gauze) in a wound. How can a wound close if it is packed open? Gauze, necrotic debris or other foreign material will quickly form a biofilm. The combination of inflammation and pressure aided by a cotton packing itself results in pain, odor, and drainage. Mechanical control of biofilm works but a scalpel is dangerous. Rather, a blunt device like a tongue blade can be used to curette off the biofilm. This is curettage, not debridement and can be done by the wound care RN. Similarly, the dressing change protocol should effectively remove remaining auto digested tissue and provide a salubrious environment which is judged effective if it quickly results in no odor, drainage, or pain and a lush granulating bed.
When a patient is placed on Hospice the above protocol is to be continued given that "prevention of any injury or suffering" is a mandate common to Hospice organizations. If the cutaneous support supplements are discontinued skin failure will progress, existing wounds will deteriorate, and new wounds will form. Any argument that continuing the Three Pillar wound care protocol will prolong life is mute in view of the fact to not do so will potentially cause suffering. Wound care for the Hospice patient is comfort care.
The field of wound care is a rewarding practice for the RN. By organizing procedures and practice into three inter related functions the rate of pressure wound healing is increased, costs decreased, and professional satisfaction achieved.
Early intervention with micronutrient supplements upon observation of cutaneous signs of scurvy has significant prevention potential. With Acknowledge to Our Staff at Onsite Healthcare Inc. Roger L. Teran, MD, Martha J. Cuevas and Vanessa Rojas.
The material contained in this paper has three distinct pillars of information. This lends itself to presentation as three separate articles.
References
-
Patient Protection and Affordable Care Act. Wikipedia.
-
Amadeo K. How the Affordable Health Care Act Affects You. The Balance.
-
National Pressure Ulcer Advisory Panel (NPUAP) The National Pressure Ulcer Advisory Panel - NPUAP.
-
European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel. Treatment of pressure ulcers: Quick Reference Guide. Washington DC: National Pressure Ulcer Advisory Panel; 2009.
-
Bergstom N (1994) Chapter 1. Clinical Practice Guideline – Treatment of Pressure Ulcers. U.S. Department of Health and Human Services, Agency for Health Care Policy and Research, 95-0653.
-
Kaminski MV, Drinane, JJ (2014) Learning the Oral and Cutaneous Signs of Micronutrient Deficiencies. J Wound Ostomy Continence Nurs 41(2): 127-135.
-
Graham B (2009) Essential Fatty Acid Deficiency – Signs & Symptoms, Treating vs. Testing. ProHealth.com.
-
Badawy AA (2014) Pellagra and Alcoholism: A Biochemical Perspective. Alcohol and Alcoholism 49(3): 238-250.
-
Morin K (2005) Water-Soluble Vitamins. American Journal of Maternal Child Nursing 30(4): 271.
-
(2016) Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline, Home.
-
Kaminski MV, Pinchcofsky G, Williams SD (1989) Nutritional Management of Decubitus Ulcers the Elderly. Advances in Skin & Wound Care 2(4): 20-30.
-
(2018) Angular Cheilitis – Symptoms, Causes, Treatment, Contagious, Pictures. Angular Cheilitis - Pictures, Symptoms, Contagious, Treatment.
-
(2016) Vitamin and Mineral Supplement Fact Sheets. Vitamin and Mineral Supplement Fact Sheets.
-
Kagoma P (1985) The Effect of Vitamin E on Experimentally Induced Peritoneal Adhesions in Mice. Arch Surg 120(8): 949-951.
-
Raju SS, Kulkarni DR (1986) Vitamin A reverses the Wound-Healing Suppressant Effect of Cyclophosphamide. Indian Journal of Pharmacology 18(3): 154-157.
-
Taren D, Chvapil M, Weber C (1987) Increasing the Breaking Strength of Wounds Exposed to Preoperative Irradiation Using Vitamin E Supplementation. Int J Vitam Nutr Res 57(2): 133- 137.
-
Greenwald DP, Sharzer LA, Padawer J, Levenson SM, Seifter E (1990) Zone II flexor tendon repair: Effects of vitamins A, E, beta-carotene. J Surg Res 49(1): 98- 102.
-
Lappe J, Travers D, Davies M, Recker R, Heaney R (2007) Vitamin D and Calcium Supplementation Reduces Cancer Risk: Results of a Randomized Trial. Am J Clin Nutr 85(6): 1586-1591.
-
Holick MF (2007) Vitamin D Deficiency. N Engl J Med 357(3): 266-281.
-
Ramagopalan SV, Heger A, Berlanga AJ, Maugeri NJ, Lincoln MR, et al. (2010) A ChIP-seq defined genome- wide map of vitamin D receptor binding: Associations with disease and evolution. Genome Res 20(10): 1352-1360.
-
Tian XQ, Chen TC, Holick MF (1995) 1, 25- Dihydroxyvitamin D3: A novel agent for enhancing wound healing. J Cell Biochem 59(1): 53-56.
-
Segaert S (2008) Vitamin D Regulation of Cathelicidin in the Skin: Toward a Renaissance of Vitamin D in Dermatology? J Invest Dermatol 128(4): 773-775.
-
Shin DM, Yuk JM, Lee HM, Lee SH, Son JW, et al. (2010) Mycobacterial lipoprotein activates autophagy via TLR2/1/CD14 and a functional vitamin D receptor signalling. Cell Microbiol 12(11): 1648-1665.
-
Sunlight and Vitamin D Synthesis. Sunlight & Vitamin D Production in the Human Body.
-
Hulsey TK, O Neill JA, Neblett WR, Meng HC (1980) Experimental wound healing in essential fatty acid deficiency. Journal of Pediatric Surgery 15(4): 505- 508.
-
Simopoulos A (2006) Evolutionary Aspects of Diet, the Omega-6/Omega-3 Ratio, and Gene Expression. Phytochemicals Nutrient-Gene Interactions 137-159.
-
Doughman SD, Krupanidhi S, Sanjeevi CB (2007) Omega-3 Fatty Acids for Nutrition and Medicine: Considering Microalgae Oil as a Vegetarian Source of EPA and DHA. Curr Diabetes Rev 3(3): 198-203.
-
Zuber M, Zia F, Zia KM, Tabasum S, Salman M, et al. (2015) Collagen based polyurethanes—A review of recent advances and perspective. Int J Biol Macromol 80: 366-374.
-
MacKay D, Miller AL (2003) Nutritional Support for Wound Healing. Altern Med Rev 8(4): 359-377.
-
Akikusa JD, Garrick D, Nash MC (2003) Scurvy: forgotten but not gone. J Paediatr Child Health 39(1): 75-77.
-
Blee TH, Cogbill TH, Lambert PJ (2002) Hemorrhage associated with vitamin C deficiency in surgical patients. Surgery 131(4): 408-412.
-
Michels AJ, Hagen TM, Frei B (2013) Human Genetic Variation Influences Vitamin C Homeostasis by Altering Vitamin C Transport and Antioxidant Enzyme Function. Annu Rev Nutr 33(1): 45-70.
-
Figueroa Méndez R, Rivas Arancibia S (2015) Vitamin C in Health and Disease: Its Role in the Metabolism of Cells and Redox State in the Brain. Frontiers in Physiology 6.
-
Mayne R, Burgeson R (1987) Water Soluble Vitamins. In Structure and Function of Collagen Types. Orlando: Academic Press: 312.
-
Woessner JF Jr (1991) Matrix metalloproteinases and their inhibitors in connective tissue remodeling. FASEB J 5(8): 2145-2154.
-
Prasad A (1995) Zinc: an Overview. Nutrition 11(1): 93-99.
-
Shatzman AR, Henkin RI (1981) Gustin concentration changes relative to salivary zinc and taste in humans. Proc Natl Acad Sci U S A 78(6): 3867-3871.
-
Beletate V, El Dib RP, Atallah AN (2007) Zinc supplementation for the prevention of type 2 diabetes mellitus. Cochrane Database of Systematic Reviews Reviews (1): CD005525.
-
Lansdown ABG, Mirastschijski U, Stubbs N, Scanlon E, Ågren MS (2007) Zinc in wound healing: Theoretical, experimental, and clinical aspects. Wound Repair Regen 15(1): 2-16.
-
Kanoni S, Dedoussis GV, Herbein G, Fulop T, Varin A, et al. (2010) Assessment of gene-nutrient interactions on inflammatory status of the elderly with the use of a zinc diet score--ZINCAGE study. Journal of Nutritional Biochemistry 21(6): 526-531.
-
Greaves MW, Skillen AW (1970) Effects of Long- Continued Ingestion of Zinc Sulphate in Patients with Venous Leg Ulceration. The Lancet 296(7679): 889- 891.
-
Kanoni S, Dedoussis GV, Herbein G, Fulop T, Varin A, et al. (2010) Assessment of gene–nutrient interactions on inflammatory status of the elderly with the use of a zinc diet score — ZINCAGE study. 21(6): 526-531.
-
Jackson MJ, Jones DA, Edwards RHT, Swainbank IG, Coleman ML (1984) Zinc homeostasis in man: studies using a new stable isotope-dilution technique. Br J Nutr 51(02): 199-208.
-
Antonowicz I, Kodicek E (1969) The effect of scurvy on glycosaminoglycans of granulation tissue and costal cartilage. Biochem J Biochemical Journal 111(5).
-
Mccarty MF (1996) Glucosamine for wound healing. Med Hypotheses 47(4): 273-275.
-
Fialkova MA, Smirnova TIu, Ivanova GI, Aboiants RK, Golubeva VF (1989) Effect of chondroitin sulfate preparations on wound healing and the strength of the surgical scar. Biull Eksp Biol Med 108(3): 1327- 1329.
-
Kaminski MV Jr, Haase TJ (1992) Albumin and colloid osmotic pressure: implications for fluid resuscitation. Crit Care Clin 8(2): 311-321.
-
Enoch P, Price S Cellular (2004) Molecular and biochemical differences in the pathophysiology of healing between acute wounds, chronic wounds and wounds in the aged. World Wide Wounds.
-
Crawford WH (2009) Tissue Repair and Wound Healing. PTHL 312a: Basic Disease Processes 53-68.
-
Lorenz PH, Longaker MT (2008) Wounds: Biology, Pathology, and Management. In: Norton JA, et al. (eds), Surgery. Springer, New York, NY, pp: 191-208.
-
Stadelmann WK, Digenis AG, Tobin GR (1998) Physiology and healing dynamics of chronic cutaneous wounds. Am J Surg 176(2): 26S-38S.
-
Ehrlichman RJ, Seckel BR, Bryan DJ, Moschella CJ (1991) Common Complications of Wound Healing. Prevention and Management. The Surgical Clinics of North America 71(6): 1323-1351.
-
Clark RAF (1988) The Molecular and Cellular Biology of Wound Repair. Wound Repair: 3-50.
-
Bjarnsholt T (2013) The role of bacterial biofilms in chronic infections. APMIS 136: 1-51.
-
Stoodley P, Sauer K, Davies DG, Costerton JW (2002) Biofilms as Complex Differentiated Communities. Annu Rev Microbiol 56:187-209.
-
Olson ME, Ceri H, Morck DW, Buret AG, Read RR (2002) Biofilm bacteria: formation and comparative susceptibility to antibiotics. Can J Vet Res 66(2): 86- 92.
-
Chiappelli, F, Bach, Q, Kasar, V (2015) Implications and applications of systematic reviews for evidence- based dentistry and comparative effectiveness research: A sample study on antibiotics for oro-facial cellulitis treatment. Dental Hypotheses Dent Hypotheses 6(4): 134-140.
-
Cruz F, Leite F, Cruz G, Cruz S, Reis J et al. (2013) Sutures coated with antiseptic pomade to prevent bacterial colonization: a randomized clinical trial. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology 116(2): e103-109.
-
Zarchi, K, Jemec, GB (2012) The efficacy of maggot debridement therapy - a review of comparative clinical trials. Int Wound J 9(5): 469-477.
-
Armstrong MH, Price P (2004) Wet-to-Dry Gauze Dressings: Fact and Fiction. Wounds 16(2): 56-62.
-
Kirkby KA, Wheeler JL, Farese JP, Ellison GW, Bacon NJ, et al. (2010) Surgical views: Vacuum-assisted wound closure: clinical applications. Compend Contin Educ Vet 32(3): E1-6.
- Teaching Cognitive Behavioral Therapy to Graduate Psychiatric Mental Health Nurse Practitioner Students: Utilizing A Mixed Methods Course Evaluation
- The Role of Pharmacogenetic Testing in Clinical Practice: A Path toward more Effective, Personalized and Cost-effective Care
- Implementing Screening with the GAD-7 in an Outpatient Mental Health Setting: A Quality Improvement Project
- Social Media and Health Promotion
- Impact of Covid-19 Pandemic on the Academic Performance and Attitude of Nursing Students towards E-Learning
- A Study to Assess the Knowledge Regarding Ill Effects of Tobacco Consumption on Health among Adolescents in Selected Higher Secondary School in Nadiad City