Fetus in Fetu
Fetus in fetu (FIF) is an extremely rare condition where a malformed or partially developed fetus is found within the body of its living twin. This anomaly arises from incomplete separation of monozygotic twins during early development, resulting in the parasitic twin being absorbed by the host twin. FIF is often identified via prenatal imaging such as ultrasound or MRI, or during postnatal surgery. Diagnosis is confirmed through histopathological examination of the mass, which reveals diverse fetal tissues. Treatment typically involves surgical removal of the parasitic twin, with a generally positive prognosis for the host. FIF offers unique insights into twin development and teratoma formation.
Abbreviations
FIF: Fetus in Fetu; MRI: Magnetic Resonance Imaging; CT: Computed Tomography.
Introduction
Fetus in fetu (FIF) is a rare and intriguing medical condition characterized by the presence of a malformed or partially developed fetus within the body of a living fetus. This condition falls under the broader category of teratomas, which are tumors containing tissues from different germ layers. FIF is an extraordinary phenomenon, shedding light on the complexities of fetal development and twin pregnancies. This article provides an in-depth examination of FIF, including its definition, causes, clinical features, diagnosis, treatment, and medical significance [1].
Definition and Background
Fetus in fetu (FIF) occurs when a twin embryo or fetus becomes incorporated within the body of its co-twin. This phenomenon typically arises during early fetal development due to the incomplete separation of monozygotic (identical) twins. One twin, known as the parasitic twin, becomes absorbed into the body of the host twin [2]. The condition is exceedingly rare, with only a few hundred cases documented in medical literature. FIF is often discovered through prenatal imaging or during surgery after birth (Figure 1).
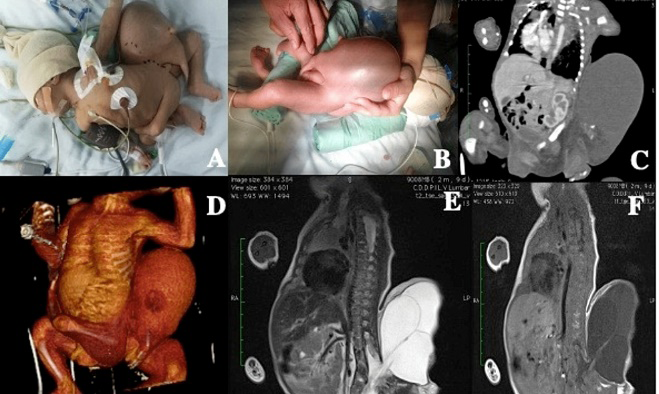
A and B: A one-week-old newborn with T12-L1 paraplegia had a parasitic twin attached to the dorso-lumbosacral region, featuring rudimentary hand traces and extremities. C and D: Tomography and 3D reconstruction showed the twin with a liquid cavity, sharing organs and bones with the newborn. D and E: MRI revealed a shared spinal column, spina bifida from L1 to L2, nerve root involvement, and myelomeningocele with extensive sacral agenesis.
Causes and Mechanisms
The primary cause of FIF is incomplete separation of monozygotic twins during the early stages of embryonic development. Monozygotic twins originate from a single fertilized egg that splits into two embryos. If the separation process is not complete, one embryo can become enveloped by the other. Several factors contribute to this process: Incomplete Embryo Separation: During the early stages of pregnancy, the division of the embryo into two separate entities may not be entirely successful. One embryo may be absorbed into the body of the other, leading to the development of FIF [3]. Genetic Mutations: While specific genetic causes are not fully understood, mutations and genetic anomalies might play a role in the development of FIF. Some research suggests that certain genetic factors could predispose embryos to this rare condition [4].
Clinical Features
Fetus in fetu can present with a range of clinical features, depending on the stage of pregnancy and the extent of development of the parasitic twin. Key features include: Prenatal Diagnosis: FIF may be detected during pregnancy through ultrasound imaging, which can reveal an abnormal mass with structures resembling a fetus. Advanced imaging techniques like MRI can provide further insights into the nature of the mass [2]. Postnatal Diagnosis: In some cases, FIF is identified after birth when a mass resembling a fetus is found within the abdomen of the host baby. Symptoms might include abdominal swelling or the presence of a palpable mass [3].
Diagnosis
The diagnosis of FIF involves a combination of imaging studies and surgical evaluation. Key diagnostic steps include: Ultrasound: Prenatal ultrasound is the primary tool for detecting FIF. It can show an abnormal mass with fetal-like structures, including limbs, vertebrae, and sometimes even internal organs [5]. MRI: Magnetic Resonance Imaging (MRI) provides detailed images of the mass and can help differentiate FIF from other types of tumors or masses [3].
Histopathological Examination: After surgical removal, histopathological analysis confirms the diagnosis of FIF by revealing the presence of various fetal tissues within the mass [2].
Treatment and Management
The primary treatment for FIF is surgical intervention. Key aspects of treatment include: Surgical Removal: The parasitic twin is typically removed through surgery. The timing of the surgery can vary; it may be performed prenatally if the condition is detected early, or postnatally if discovered after birth [6]. Prognosis: The prognosis for the host twin is generally favourable if the condition is managed effectively. Complications can arise, but early intervention usually results in a positive outcome [7].
Medical and Research Significance
Fetus in fetu offers valuable insights into fetal development and the mechanisms of twin formation. The rarity of FIF makes it a subject of considerable interest in medical research. Some key points of significance include: Developmental Insights: FIF provides a unique opportunity to study the processes of twin formation and the consequences of incomplete embryo separation. It enhances our understanding of early developmental stages and anomalies [8]. Teratoma Studies: FIF contributes to the broader field of teratoma research, helping researchers understand the development of tumors containing diverse tissues from different germ layers [9].
Recent Advances
Advancements in medical imaging and genetic research have improved the diagnosis and understanding of FIF: Advanced Imaging: High-resolution ultrasound and MRI techniques have enhanced the ability to detect and diagnose FIF more accurately, leading to better management and outcomes [10]. Genetic Research: On-going studies explore the genetic and developmental factors associated with FIF, aiming to uncover potential preventive measures and improve our understanding of this rare condition [11].
Case Report
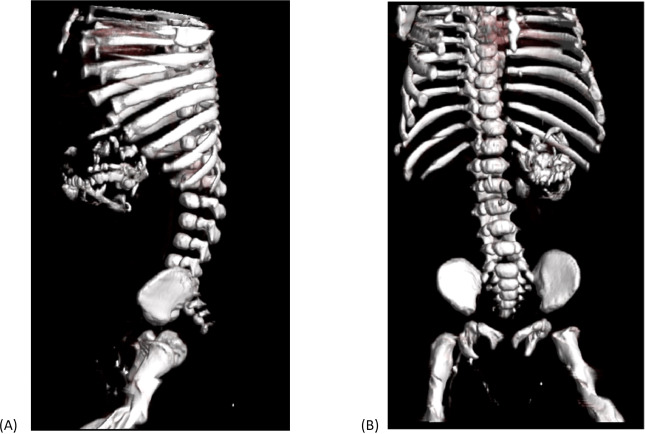
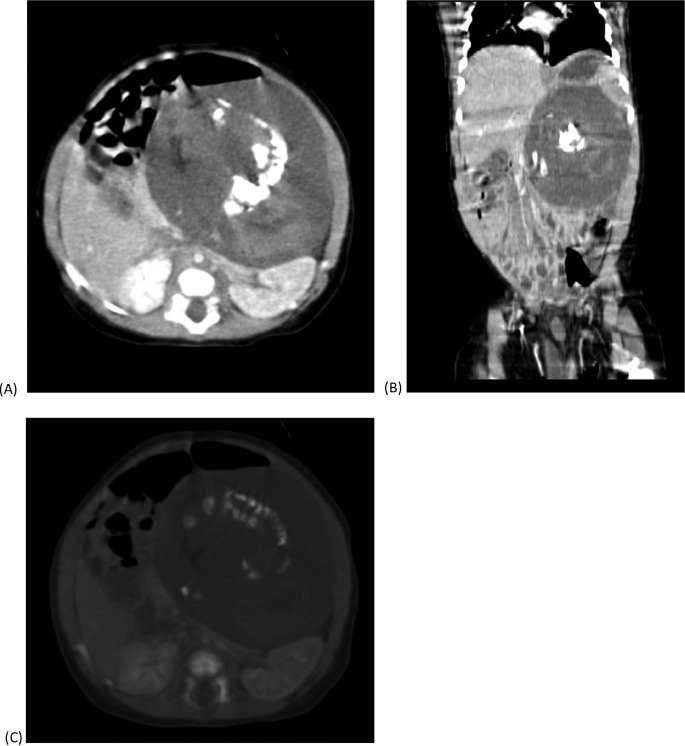
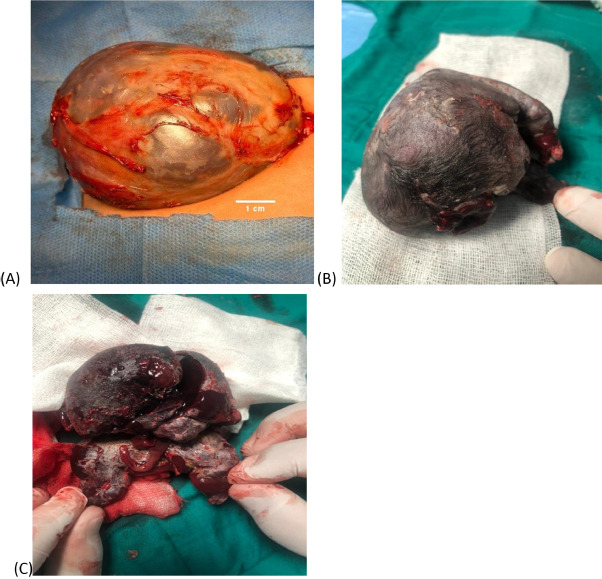
A 2-month-old male infant presented with an 8 × 12 cm solid, semi-mobile abdominal mass in the left upper quadrant. Imaging revealed a heterogeneous lesion on CT scan, with components including soft tissue, fat, fluid, and bone, causing displacement of bowel loops and major abdominal vessels [12]. The mass, extending into the left lumbar and epigastric regions, contained identifiable structures such as spine, ribs, facial bones, limbs, and scapula (Figures 2-4).
Conclusion
Fetus in fetu remains a rare but fascinating condition that highlights the complexities of fetal development and twin pregnancies. Its study provides valuable insights into the mechanisms of twin formation, the nature of teratomas, and the intricacies of early human development. Continued research and advances in imaging technology promise to enhance our understanding and management of this intriguing phenomenon.
References
-
Gupta N, Sharma D, Sharma P, Sharma R (2006) Fetus in fetu: A Review of the Literature with a Case Report. Pediatric Surgery International 22(9): 756-759.
-
Gassner HG, Ferraro N, Williams L (2005) Fetus in Fetu: A Review of Clinical and Histopathological Features. Human Pathology 36(9): 934-939.
-
Kumar R, Gupta AK, Sinha R, Choudhury P (2012) Fetus in Fetu: Prenatal Diagnosis and Postnatal Management. Journal of Pediatric Surgery 47(4): 727-731.
-
Suri V, Abdullah A, Verma S (2013) Genetic and Epigenetic Mechanisms in the Development of Teratomas and Fetus in Fetu. Pediatric and Developmental Pathology 16(4): 251-257.
-
Chuang SM, Lee CH (2012) Prenatal Diagnosis of Fetus in Fetu using Ultrasound: A Review. Journal of Clinical Ultrasound 40(5): 304-310.
-
Kaur A, Singh H (2014) Surgical Management of Fetus in Fetu: A Review. Journal of Pediatric Surgery 49(7): 1023- 1028.
-
Khatib S, Hisham A (2016) Prognosis and Management of Fetus in Fetu: A Review of the Literature. Journal of Pediatric Surgery 51(3): 471-477.
-
Smith JB, Lee CH (2014) Fetus in Fetu and its Developmental Implications: A Review of Twin Formation and Embryonic Anomalies. Developmental Biology 392(1): 3-12.
-
Patel AR, Kumar R (2017) Fetus in Fetu: Contributions to the Understanding of Teratomas and Germ Cell Tumors. Journal of Pathology and Translational Medicine 51(2): 155-163.
-
Xu J, Liu Y (2020) Advances in Imaging Techniques for the Diagnosis of Fetus in Fetu. Journal of Ultrasound in Medicine 39(8): 1587-1597.
-
Murphy C, Walker J (2021) Exploring the Genetic Basis of Fetus in Fetu and Implications for Future Research. Journal of Genetic Counseling 30(2): 381-390.
-
Agarwal A, Agrawal M, Ahuja S (2024) Fetus in Fetu in a 1-year-old Female: A Case Report. Journal of Pediatric Surgery Case Reports.
- Teaching Cognitive Behavioral Therapy to Graduate Psychiatric Mental Health Nurse Practitioner Students: Utilizing A Mixed Methods Course Evaluation
- The Role of Pharmacogenetic Testing in Clinical Practice: A Path toward more Effective, Personalized and Cost-effective Care
- Implementing Screening with the GAD-7 in an Outpatient Mental Health Setting: A Quality Improvement Project
- Social Media and Health Promotion
- Impact of Covid-19 Pandemic on the Academic Performance and Attitude of Nursing Students towards E-Learning
- A Study to Assess the Knowledge Regarding Ill Effects of Tobacco Consumption on Health among Adolescents in Selected Higher Secondary School in Nadiad City