Investigating the Impact of Pregnancy-Induced Hypertension on Fetal Outcomes: A Comprehensive Study in Maternity Hospitals
Background: Hypertension in pregnancy is a major obstetric complication that poses a significant risk to maternal and fetal health, leading to increased morbidity and mortality. According to the World Health Organization, hypertensive disorders of pregnancy (HDP) claim the life of at least one woman every seven minutes. HDPs are associated with an increased risk of adverse fetal and neonatal outcomes, including preterm birth, intrauterine growth restriction (IUGR), perinatal mortality, and maternal morbidity and mortality. Prompt recognition and management of PIH are essential to mitigate these complications and ensure optimal maternal and fetal outcomes. Hence the study was undertaken to assess the impact of Pregnancy Induced Hypertension on fetal outcome among Antenatal mother with PIH at maternity hospital of Anand and Kheda district. Objectives: To assess the clinical presentation among mother with PIH at maternity hospital; To assess the impact of Pregnancy Induced Hypertension on fetal outcome. Methodology: A Prospective study was conducted at Dr. N. D. Desai hospital, Nadiad. Sample size was 30. Sample was selected by Consecutive Sampling Technique. The data regarding Demographic variable, Obstetric History, Classification of PIH, Blood pressure, Drug Received & Fetal outcomes was collected using Structured Interview Scheduled. The result is computed by using descriptive and frequency and percentage using tables, graph etc. Data were analysed according to objectives of the study. Results: In present study, the incidence of gestational hypertension, pre-eclampsia, and eclampsia was 10%, 86.66%, and 3.33%, respectively. These conditions were more common in primipara. The symptoms of pregnancy-induced hypertension (PIH) included pedal edema (60%), vomiting (43.33%), blurry vision (6.66%), convulsions (3.33%), and dizziness (6.66%), as well as epigastric pain (16.66%) and lower abdominal pain (36.66%). Most mothers (83.33%) received antihypertensive medication. The study also found that fetal complications included preterm births (66.66%) and low birth weight (56.66%). Additionally, 63.33% of babies required NICU admission, and there were cases of post-term birth (3.33%), congenital abnormalities (3.33%), birth asphyxia (3.33%), and neonatal deaths (10%). Conclusion: Pregnancy-induced hypertension is a common and serious condition that can have devastating effects on both mothers and babies. To combat this, we need to raise awareness and take action at both community and hospital levels to reduce the risks and improve outcomes.
Abbreviations
PIH: Pregnancy-Induced Hypertension; DIC: Disseminated Intravascular Coagulation; SGA: Small for Gestational Age; IUGR: Intrauterine Growth Restriction; IUFD: Intrauterine Fetal Death; PTL: Preterm Labor; LBW: Low Birth Weight; NICU: Neonatal Intensive Care Unit; NMM: Neonatal Morbidity and Mortality.
Introduction
Pregnancy is a remarkable and life-changing experience for women, typically filled with excitement and hope for a healthy and uncomplicated journey. Expectant mothers usually anticipate a smooth pregnancy and delivery, but unfortunately, complications can arise. Among these potential complications, Pregnancy-Induced Hypertension (PIH) is a common and significant threat to the health and well-being of both mother and baby [1].
Pregnancy induced hypertension is defined as a systolic blood pressure above 140mmHg or a diastolic blood pressure above 90mmHg, or both. Both systolic and diastolic pressure increases are crucial in identifying pregnancy-induced hypertension. PIH is a type of hypertension that develops after the 20th week of gestation in women who previously had normal blood pressure. PIH is broadly categorized into three types: gestational hypertension, pre-eclampsia, and eclampsia, which are distinguished by their severity and symptoms [2].
Women with Pregnancy-Induced Hypertension (PIH) are at increased risk for obstetric and perinatal complications, including placental abruption, maternal organ dysfunction, and disseminated intravascular coagulation (DIC). Furthermore, those with a history of severe preeclampsia are more likely to experience persistent postpartum symptoms, such as headaches, left upper quadrant pain, visual disturbances, fatigue, and cognitive impairment. Long-term, PIH is associated with an elevated risk of cardiovascular disease, including atherosclerosis and hypertension, as well as an increased incidence of Type 2 diabetes mellitus and intracranial hemorrhage. Additionally, fetuses of mothers with PIH are at higher risk for intrauterine growth restriction (IUGR), preterm birth, small for gestational age (SGA), and intrauterine fetal demise (IUFD) [3].
Fetal complications such as Intrauterine Growth Restriction (IUGR), Intrauterine Fetal Death (IUFD), stillbirths, Preterm Labour (PTL) and Low Birth Weight (LBW) infants, increased need for Neonatal Intensive Care Unit (NICU) admission, and elevated Neonatal Morbidity and Mortality (NMM) rates are prevalent, highlighting the importance of antenatal surveillance and timely interventions to mitigate these adverse pregnancy outcomes [4].
Currently there are about 7 million cases of pre- eclampsia each year [5]. Between 2000 and 2023 the overall prevalence of PIH ranged between 6.9% and 62.2%, with the highest prevalence noted within African studies and lowest in South American studies [6].
The prevalence of hypertensive disorder of pregnancy in India varies by region. For example, a cross-sectional study conducted in Kashmir found prevalence of PIH 7.4% in 2023 [7] and an observational study in selected hospital of west Bengal found prevalence of PIH 9.01% in 2023 [8].
Objectives
To assess the clinical presentation among mother with PIH at maternity hospital. To assess the impact of Pregnancy Induced Hypertension on fetal outcome.
Assumptions
The impact of Pregnancy induced hypertension may be observed among pregnant women. The effect of hypertension during pregnancy may affect the fetal and maternal outcome.
Review of Literature
Preet A, et al. [9] Hypertensive disorder of pregnancy one of the most common medical Disorder seen during pregnancy. Early diagnosis of hypertensive disordered of pregnancy by regular antenatal checkup can help in proper management, thus decreasing the maternal fetal complication related to them. Objectives: To study Feto-maternal outcomes of hypertensive disordered of pregnancy and complication related to them. A study was conducted in department of obstetric and gynecology at JJ group of hospital, Mumbai, India for duration of 18 month from January 2020 to June 2021. This study had a sample size of 500 antenatal patients. Result: The incidence of hypertensive disorder of pregnancy was 10.2%, being most common in age group of 21-25 years (45.1%) and primigravida patients (47.1%). The most common type of hypertensive disorder in our study was non severe pre-eclampsia with incidence of 74.50%. The most common complication was ligohydrominos (11.76%), followed by pre-term delivery (9.80%) and IUGR (9.80%). The most common neonatal complication in PIH group was low birth weight followed by fetal distress (19.6%), prematurity (9.8%) and IUGR(9.80%).Conclusion: Hypertensive disorder of pregnancy are more prevalent in younger and nulliparous mothers. Early diagnosis and appropriate management of hypertensive disorder in pregnant women can prevent the maternal and fetal complication and improve the outcome of pregnancy. These women should be monitored carefully to prevent maternal morbidity and mortality [9].
Ain SN, et al. [10] Pregnancy induced hypertension is a significant cause of morbidity among pregnant females and also affects the foetal outcome. Objectives: To estimate the prevalence of PIH and the factors associated with PIH. A cross-sectional study was conducted over a 3 month period from July to September 2021 using convenient sampling. A total of 402 pregnant women were included. Result: majority (97.8%) were up to para 3 and 89% were literate. The prevalence of PIH was 6.5%. Hypertension was more frequent among the women with age more than 30 years (p=0.041) and women with higher pre-pregnancy BMI (p=0.010). Maternal education, occupation and parity were not associated with hypertension in pregnancy. Conclusion: In study older women with higher BMI were more at risk of having PIH in pregnancy. Therefor we would recommend earlier age at marriage and lifestyle modification for maintaining normal BMI [10].
Elghoudi A, et al. [11] Maternal and perinatal mortality and morbidity are mainly affected by hypertension during pregnancy. Haemorrhage and cerebral bleeding are the primary and significant complication of pre-eclampsia. Abruption of placenta and renal failure are among major complications caused by this disease. Objectives: To examine the incidence of PIH, pre-eclampsia, the management of PIH, including the early diagnosis, the pharmacological drug management used, and prevalence of maternal and perinatal complications. The cross-sectional study took place in alijalaa maternity hospital, which represented the west state of Libiya in period from 1st January 2012 to 31st December 2012, the sample size was 660 with patients who were diagnosed, managed, and terminated according to protocol management of the hospital. Result: The incidence of PIH is 8.4% and pre-eclampsia is 5.1%. The reported complication included: Eclampsia, HELLP syndrome, abruption placenta, and pulmonary oedema see in 18%, 6%, 9%, 4% and less than one percent, respectively. The fetal complication were pre term babies and IUGR in nineteen percent, LBW in twenty-five percent, IUFD in five percent, neonatal death in two percent, perinatal death in six percent. In the PIH patients, the presence of associated symptoms such as headache, blurred vision, irritability, and presence of such as severe hypertension, generalized oedema, exaggerated reflexes, increased risk of maternal and fetal complication. Conclusion: to decrease mother and newborn mortality and morbidity in PIH patients, a rigorous management protocol is required to implement evidenced based guidelines [11].
Materials and Methods
Research Approach
Quantitative research approach
Research Design
Prospective observational research design
Research Variable
Impact of pregnancy induced hypertension
Socio Demographic Variable
Age, Religion, Residential status, Food pattern, Education, Occupation
Population
Antenatal mother with Pregnancy induced hypertension
Research Setting
Selected Maternity hospital of Anand and Kheda district
Sample
Sampling Technique: Consecutive sampling technique Sample Size: 30 Sampling Criteria Inclusive Criteria
- Women with & after 20 weeks of gestation with PIH & delivered at maternal hospital of Anand and Kheda district.
- Women who are willing to participate
- Women who knows Gujrati, English, Hindi Exclusive Criteria
- Women who are not willing to participate in study.
- Women who are not having PIH after 20th week.
Tool for Data Collection
A structured Quetionnaire was prepared. The data was collected using Structured Interview Scheduled method. The tool was divided into 6 sections. Section I: It Consist of socio-demographic variable that includes Age, Religion, Residential status, Food pattern, Education, Occupation. Section II: Distribution of PIH mothers as per obstetric history. Section III: Mothers as per classification of PIH. Section IV: PIH mothers as per their blood pressure. Section V: PIH mothers as per drug received.
Section VI: Fetal outcomes of mothers with PIH.
Results
Table 1 Shows that the majority of mothers with Pregnancy-Induced Hypertension (PIH) fell into two age groups: 16(53.33%) were between 18-22 years old, and 9(30%) were between 23-27 years old. The dominant characteristics of PIH mothers were: 25(83.33%) were Hindu, 25(83.33%) had an educational level below SSC, and all were homemakers. Additionally, 18(60%) followed a vegetarian diet, while 8(26.66%) and 4(13.33%) followed non-vegetarian and ovo-vegetarian diets, respectively. Most PIH mothers 21(83.33%) resided in rural areas.
| Demographic | Frequency | Percentage (%) |
|---|---|---|
| Age (In years) | ||
| 18-22 | 16 | 53.33% |
| 23-27 | 9 | 30% |
| 28-32 | 3 | 10% |
| >32 | 2 | 6.66% |
| Religion | ||
| Hindu | 25 | 83.33% |
| Muslim | 4 | 13.33% |
| Christian | 0 | 0% |
| Other | 1 | 3.33% |
| Residential Status | ||
| Urban | 9 | 30% |
| Rural | 21 | 70% |
| Food Pattern | ||
| Veg | 18 | 60% |
| Nonveg | 8 | 26.66% |
| Ova-veg | 4 | 13.33% |
| Education | ||
| <SSC | 25 | 83.33% |
| SSC | 0 | 0% |
| HSC | 5 | 16.66% |
| Graduation | 0 | 0% |
| Occupation | ||
| Home maker | 30 | 100% |
| Working women | 0 | 0% |
Table 1: Socio-demographic profile of PIH mothers (n=30).
Table 2 shows the majority of participants 23(76.66%) had moderate anemia, while 5(16.66%) had severe anemia. In terms of weight, 12(40%) of participants fell into the 40- 49 kg range, followed by 12(40%) in the 50-59 kg range. Most participants were primigravida 17(56.66%) and primipara 17(56.66%), indicating it was their first pregnancy and delivery. A significant number of participants had a previous history of PIH 4(13.33%) and C Section 4(13.33%). During their current pregnancy, common symptoms included pedal edema 18(60%), vomiting 13(43.33%), and lower abdominal pain 11(36.66%) while blurry vision and Dizziness were 2(6.66%), headache, convulsion, epigastric pain were 8(26.66%), 1(3.33%), 5(16.66%) respectively. A small percentage of participants had a family history of PIH 5(16.66%). 6(20%) were undergone emergency LSCS while 10(33.33%) and 14(46.66%) had vaginal and C section respectively. 22(73.33%) delivered before 37 weeks of gestation, 8(26.66%) delivered between 37-39 weeks of gestation.
| Obstetric History | Frequency | Percentage (%) |
|---|---|---|
| HB Level (in g/dl) | ||
| <9 | 5 | 16.66% |
| 9-13 | 23 | 76.66% |
| 14-18 | 2 | 6.66% |
| Weight of Mother (in kg) | ||
| 40-49 | 12 | 40% |
| 50-59 | 12 | 40% |
| 60-69 | 4 | 13.33% |
| >69 | 2 | 6.66% |
| Gravida | ||
| 1 | 17 | 56.66% |
| 2 | 8 | 26.66% |
| 3 | 2 | 6.66% |
| Above 3 | 3 | 10% |
| Parity | ||
| Primipara | 17 | 56.66% |
| Multipara | 13 | 43.33% |
| Past Obstetric History with PIH | ||
| PIH | 4 | 13.33% |
| Pre-term | 0 | 0% |
| Previous CS | 4 | 13.33% |
| Abortion | 0 | 0% |
| Others | 8 | 26.66% |
| 17 | 56.66% | |
| Clinical Presentation during Present Pregnancy | ||
| Headache | 8 | 26.66% |
| Blurry vision | 2 | 6.66% |
| Pedel edema | 18 | 60% |
| Convulsion | 1 | 3.33% |
| Epigastric pain | 5 | 16.66% |
| Dizziness | 2 | 6.66% |
| Vomitting | 13 | 43.33% |
| Pain in lower abdomen | 11 | 36.66% |
| No complaints | 5 | 16.66% |
| Family History of PIH | ||
| Yes | 5 | 16.66% |
| No | 25 | 83.33% |
| Mode of Delivery | ||
| Vaginal | 10 | 33.33% |
| C section | 14 | 46.66% |
| Em LSCS | 6 | 20% |
| Instrumental | 0 | 0% |
| Gestational Age at Delivery | ||
| <37 week | 22 | 73.33% |
| 37-39 week | 8 | 26.66% |
| >39 week | 0 | 0% |
Table 2: Distribution of PIH mothers as per Obstetric history(n=30).
Table 3 and Figure 1 shows The PIH mothers were classified into three categories based on the severity of their condition. The majority, 86.66% (26 participants), were diagnosed with pre-eclampsia, a condition characterized by high blood pressure and proteinuria during pregnancy, which can lead to severe complications if left untreated. A small percentage, 10% (3 participants), had gestational hypertension, which is high blood pressure during pregnancy without proteinuria or other severe symptoms. The most severe category, eclampsia, accounted for 3.33% (1 participant), where mothers experienced seizures due to severe pre-eclampsia, a life-threatening condition.
| Classification of PIH mothers | Frequency | Percentage (%) |
|---|---|---|
| Gestational Hypertension | 3 | 10% |
| Pre-eclampsia | 26 | 86.66% |
| Eclampsia | 1 | 3.33% |
Table 3: Distribution of PIH mothers as per classification of PIH(n=30).
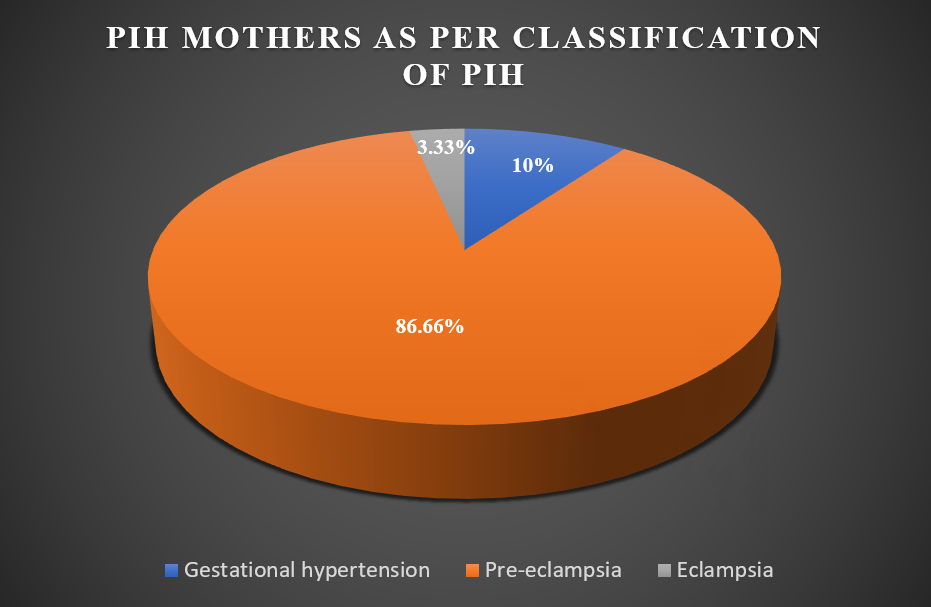
Table 4 shows the majority of PIH mothers, accounting for 22(73.33%), have systolic blood pressure readings between 140-160 mmHg and diastolic readings between
90-100 mmHg. In contrast, 8(26.66%) of PIH mothers have higher systolic readings, ranging from 161-180 mmHg, and higher diastolic readings, ranging from 101-120 mmHg. This
classification highlights the varying degrees of hypertension among PIH mothers, with most experiencing moderate elevations in blood pressure and a smaller proportion experiencing more severe increases.
| Classification of PIH mothers as per blood pressure | Frequency | Percentage (%) |
|---|---|---|
| Systolic B. P. (In mm hg) | ||
| 140-160 | 22 | 73.33% |
| 161-180 | 8 | 26.66% |
| Diastolic B. P. (In mm hg) | ||
| 90-100 | 22 | 73.33% |
| 101-120 | 8 | 26.66% |
Table 4: Distribution of PIH mothers as per their blood pressure (n=30).
Table 5 and Figure 2 shows the medication usage among the group shows that antihypertensive drugs like labetalol are the most commonly used, with 25 individuals (83.33%) receiving treatment to manage their high blood pressure. In contrast, no individuals (0%) are taking anticonvulsant medications, which are typically used to prevent seizures. Meanwhile, a smaller group of 5 individuals (16.66%) are taking other types of medications like iron, folic acid, calcium gluconate.
| Drug | Frequency | Percentage (%) |
|---|---|---|
| Antihypertensive | 25 | 83.33% |
| Anticonvulsant | 0 | 0% |
| Other | 5 | 16.66% |
Table 5: Distribution of PIH mothers as per drug received (n=30).
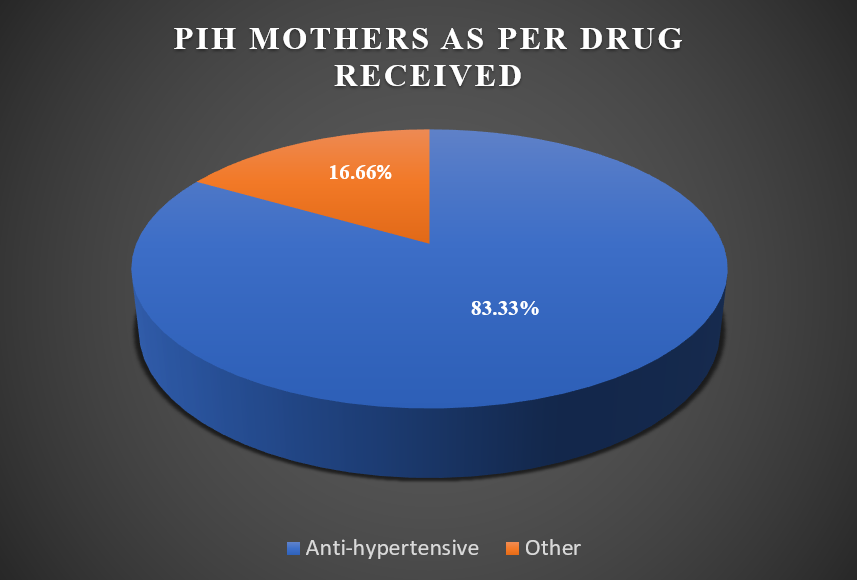
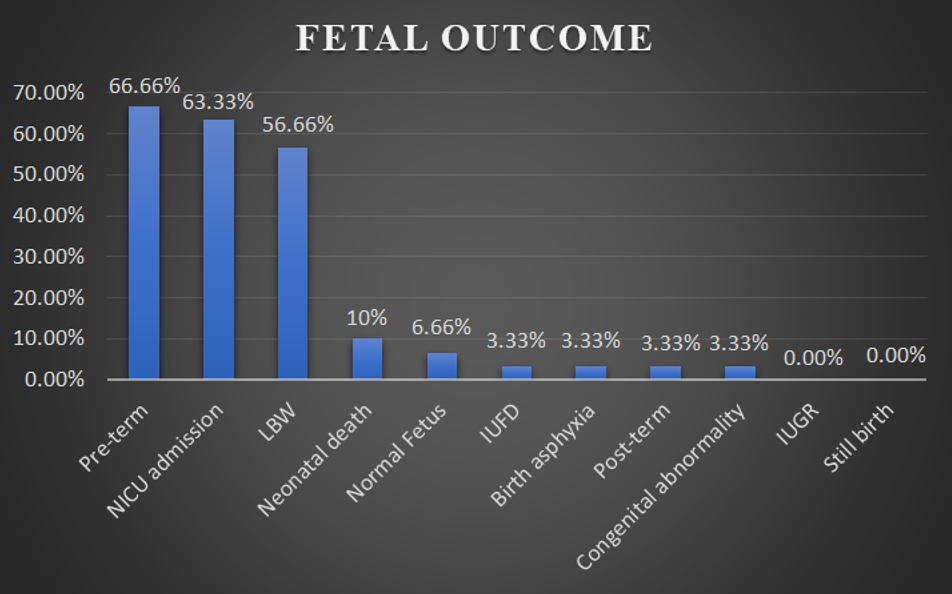
Table 6 and Figure 3 the outcomes among the group reveal a range of results. The majority of births were pre- term 20(66.66%), with only one post-term birth (3.33%). Low birth weight (LBW) was a significant concern, affecting 17 babies (56.66%). Fortunately, there were no cases of Intrauterine Growth Restriction (IUGR). However, 19 babies (63.33%) required admission to the Neonatal Intensive Care Unit (NICU). There was one case of Intrauterine Fetal Death (IUFD) and three cases of neonatal death (10%). Additionally, there was one case each of birth asphyxia, congenital abnormality, and stillbirth. Only two babies (6.66%) were reported as normal fetuses, highlighting the need for close monitoring and care in this group.
| Outcome | Frequency | Percentage |
|---|---|---|
| Pre-term | 20 | 66.66% |
| Post-term | 1 | 3.33% |
| LBW(<2.5kg) | 17 | 56.66% |
| IUGR | 0 | 0% |
| NICU admission | 19 | 63.33% |
| IUFD | 1 | 3.33% |
| Still birth | 0 | 0% |
| Neonatal death | 3 | 10% |
| Birth Asphyxia | 1 | 3.33% |
| Congenital abnormality | 1 | 3.33% |
| Normal fetus | 2 | 6.66% |
Table 6: Fetal outcome in mothers with PIH (n=30).
Discussion
A prospective observational study was carried out in selected maternity hospital of Anand and Kheda district. Consent was taken from mothers who were willing to participate in research study and data were collected through structured interview questionnaire. On analysis it was found that significant prevalence of hypertensive disorders in pregnancy, with 10% of cases classified as gestational hypertension, 86.66% as pre-eclampsia, and 3.33% as eclampsia [12, 13, 14, 15]. Notably, these conditions were more common among primipara mothers. The most frequent symptoms of PIH were pedal edema, vomiting, and abdominal pain, while antihypertensive medication was administered to the majority of mothers. Furthermore, the study highlighted a high incidence of fetal complications, including preterm births and low birth weight, with a substantial proportion of babies requiring NICU admission. Other notable complications included post-term birth, congenital abnormalities, birth asphyxia, and neonatal mortality [16, 17].
Recommendations
1. The similar study can be conducted with larger samples and different demographic variables. 2. A similar study can be do at different settings to strengthen findings.
3. A study can be conducted by retrospective research design. 4. The similar study can be conducted to investigate prevalence rate of Pre-eclampsia. 5. The study can be conducted with aim to provide guideline.
Consent and Ethical Approval
The study was approved by the institutional ethical committee (IEC) of Dinsha Patel College of Nursing, Nadiad. There is a total 15 members in the committee from various departments. The Ethical Approval Reference number is MAM Uni/IECHR/2024/45 And a formal written consent was gathered from the samples prior to data collection.
Acknowledgement
Special thanks to all participants Pregnant mothers of study, all faculties who validate the tool, Obstetrician of the hospital to permit us to conduct study in their hospitals, and Research guide for their constant support and instructions.
Competing of Interest
Authors have declared that no competing of interest exists.
References
-
Chaudhary G (2016) A Study to Assess the Effectiveness of Planned Teaching Programme (PTP) on the Knowledge Regarding Management of Pre-Eclampsia among Antenatal Mothers Attending Antenatal Clinic in Selected Hospitals of Faridkot, Punjab. Inter J Adv Res (IJAR) 4(9): 1899-905.
-
Pandya K, Prajapati A, Gajjar T, Rawat R (2021) A Study to Assess the Impact of Pregnancy Induced Hypertension on Fetal Outcomes among PIH Patients Delivered at Tertiary Care Hospital, Dadra & Nagar Haveli. Int J Health Sci Res 11(1): 268-272.
-
Cheng CC, Jen JL, Chuan CC, Yiing ML, Chi JW (2021) Effects of a Case Management Program for Women With Pregnancy-Induced Hypertension. J Nurs Res 29(5): e169.
-
Robillard PY, Dekker G, Scioscia M, Bonsante F, Boukerrou M, et al. (2023) Preeclampsia in 2023: Time for Preventing Early onset- and Term Preeclampsia: The Paramount Role of Gestational Weight Gain. J Reprod Immunol 158: 103968.
-
Mukosha M, Hatcher A, Mutale W, Lubeya MK, Conklin JL, et al. (2024) Prevalence of Persistent Hypertension Following Pregnancy Complicated by Hypertensive Disorders in Low- and Middle-Income Countries: A Systematic Review. Front Glob Womens Health 5: 1315763.
-
Qulsum R, Kaul RUR, Shah RJ, Allaqband UF (2021) Prevalence of Hypertension in Pregnancy in a Health Block Hajin of Kashmir Valley: A Cross-Sectional Study. Inter J Sci Res 10(2): 50-52.
-
Maity S, Chaudhuri S, Ghosh P (2023) Maternal Near Miss and Maternal Death among Women with Hypertensive Disorders in Pregnancy: an Observational Study in a Selected Hospital in West Bengal. International Journal of Reproduction, Contraception, Obstetrics and Gynecology 12(6): 1802-1807.
-
Preet A, Anand AR [2023] A Study on Fetomaternal Outcome of Hypertensive Disorders of Pregnancy. International Journal of Reproduction, Contraception, Obstetrics and Gynecology 12(9).
-
Ain SN, Gull S, Qulsum R, Khan ZA, Qureshi UA (2023) Prevalence of Pregnancy Induced Hypertension and Associated Factors in Kashmiri Women Attending a Tertiary Care Hospital at Srinagar: A Cross-Sectional Study. International Journal of Reproduction, Contraception, Obstetrics and Gynecology 12(2): 387- 390.
-
Elghoudi A, Alsharef A, Elghoudi A (2022) A Cross- Sectional Study on Current Practice of the Management of Pregnancy Induced Hypertension and Its Maternal and Foetal Complications and Outcome in the Western Part of the State of Libya. Open Journal of Obstetrics and Gynecology 12(3): 222-241.
-
Dutta DC (1998) Textbook of Obstetrics. In: 4th (Edn.), New Central Book Agency Publishers.
-
Patel R, Baria H, Patel HR, Nayak S (2017) A Study on Pregnancy Induced Hypertension and Foetal Outcome among Patient with PIH at Tertiary Care Hospital, Valsad. International Journal of Community Medicine and Public Health 4(11): 4277-4281.
-
Gandhi MR, Jani PS, Patel UM, Kakani CR, Thakor NC, et al. (2015) Perinatal Outcome in Pregnancy Induced Hypertension Cases at GMERS Medical College, Dharpur- Patan, North Gujarat region, India: A Prospective Study. International Journal of Advances in Medicine 2(2): 152- 155.
-
Raman RK, Kumari R, Kumar R (2022) An Observational Study On Pregnancy Induced Hypertension and it Outcome among Patients Attending a Tertiary Care Hospital of Bihar. International Journal of Health and Clinical Research 5(3): 489-492.
-
Devgan N, Devgan R (2021) Pregnancy Induced Hypertension and Foetal Outcome Among Patients with PIH in a Tertiary Care Teaching Hospital. International Journal of Health and Clinical Research 4(12): 389-393.
-
Kumari S (2020) Prevalence of Hypertensive Disorder of Pregnancy in North India. International Journal of Physiology 8(1): 86-90.
- Teaching Cognitive Behavioral Therapy to Graduate Psychiatric Mental Health Nurse Practitioner Students: Utilizing A Mixed Methods Course Evaluation
- The Role of Pharmacogenetic Testing in Clinical Practice: A Path toward more Effective, Personalized and Cost-effective Care
- Implementing Screening with the GAD-7 in an Outpatient Mental Health Setting: A Quality Improvement Project
- Social Media and Health Promotion
- Impact of Covid-19 Pandemic on the Academic Performance and Attitude of Nursing Students towards E-Learning
- A Study to Assess the Knowledge Regarding Ill Effects of Tobacco Consumption on Health among Adolescents in Selected Higher Secondary School in Nadiad City