Pico-Tesla Transcranial Magnetic Stimulation on Depression Patients with Double Blind Experimental Design
Aim: We used a whole-head 122 channel magneto encephalography system and a double-blind experimental design to patients with depression. Methods: The participants were 10 patients with depression (3 male, 7 female) ranging from 25-40 years of age. The pT-TMS was applied to the above patients with magnetic field amplitude (1-7.5pT) and frequency (8-13Hz). Each patient had two separate recording sessions consisting of 3 runs in which we gave real or sham pT-TMS. We then tried to predict the real and sham stimulation sessions based on the changes in the mean peak frequency difference in the 2-7Hz band observed in the patients' brain. Results: After unblinding a significant effect was observed with an increase of frequencies in the range of 2-7 Hz across the subjects followed by a substantial mood improvement and normalization of the MEG. A majority of the patients reported benefit from the pT-TMS treatment the results were statistically significant at 4 out of 10 patients (40 %). Conclusion: A generally accepted method that would present the highest efficacy, with the greatest acceptability for the depressed patients has not been established yet. This method of the pT-TMS has the potential to be a significant non invasive, secure and valuable means in the managing of patients with depression.
Objective
The majority of patients suffering with depressive disorder haven't experienced a reduce in symptoms by antidepressant treatments. The mainly widely used antidepressant treatments are serotonin-specific uptake inhibitors that selectively target the serotonin system.
This is because the hypothesis of depression has postulated that decrease in serotonin levels leads to increased predisposition to depression. The high prevalence of treatment resistant depression (TRD) causes an important concern for patients and also societal and economic costs. Due to this limited efficiency of existing therapies in this sub-population, other somatic treatments are investigated. Neuro stimulation treatments for TRD are vagus nerve stimulation (VNS) and deep brain stimulation (DBS). Conveying the high occurrence of TRD the expected effect of TRD is a significant societal and economic impact, with cost burden that is about twice that of non-resistant major depressive disorder (MDD) [1, 2, 3]. The electroconvulsive therapy (ECT) was used for the treatment of psychiatric disorders in 1930. It was the first therapy for depressed patients who have severe suicidal ideation or psychotic features. ECT was also indicated for treatment of MDD without psychotic features, typically when antidepressants have been tried at satisfactory doses and for an sufficient time [4]. In the last decade, alternative somatic treatments have emerged as feasible options for resistant depression, including VNS and DBS. In both cases, effectiveness and security of these interventions in the managing of neurological disorders has already been established as addition therapies for refractory seizure disorders and movement disorders [5]. Trancranial Magnetic Stimulation (TMS) was used as an extra alternative means for treatments for patients suffering from depression, reflecting the limited therapeutic advances with conventional antidepressants and the appearance of protected and efficient neuro stimulation therapies. The use of TMS is for the reason that it is a non-invasive technique to stimulate the human brain.TMS was introduced as a neurophysiological technique, when Barker, et al. [6] developed a machine that permitted non-invasive stimulation of the cerebral cortex. Since its introduction, TMS has been used to assess the motor system, to study the function of several cerebral regions, and for the pathophysiology of several neuropsychiatric illnesses. In addition, Anninos and Tsagas [7] suggested that pico Tesla TMS (pT-TMS) with an electronic device might have therapeutic potential by increased the abnormal (2-7 Hz) frequencies of the brain activity towards frequencies of less than or equal to those frequencies of the alpha frequency range (8-13Hz) of each patient [8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19]. One probable electrophysiological clarification for the efficacy of pT-TMS has been provided by the proposed “Neural Net Model” [13] which suggests that magnetic stimulation causes a temporally modulated neuronal inhibition in areas exhibiting abnormal activity in the frequency range of 2-7Hz. This proposal is in concordance with information presented by other investigators [20, 21, 22]. Another explanation for managing the symptoms of depression patients using pT-TMS is based on Morrell’s hypothesis that each stimulus entering the brain is maintained for a certain period of time representing the short-term memory of the particular stimulus occurrence [23]. If the stimulus experience persisted for an extending period of time then the short-term memory of the presented stimulus is converted to the permanent memory of the stimulus. Based on this principle from neurophysiology it may be possible to make the brains of depression patients to change their abnormal activities to normal using pT-TMS of proper frequencies and intensities. The aim of this study is to identify any change in the brain state in accordance with our predictions that the pT-TMS should increase the mean peak frequency difference (MPFD) within the 2-7Hz band towards frequencies ≤ 8-13Hz for each depression patient.
Methods
Biomagnetic measurements were performed using a whole-head 122-channel MEG gradiometer device (Neuromag-122, Neuromag Ltd. Helsinki, Finland) in an electromagnetically shielding room. The spontaneous MEG recordings were taking with sampling frequency rate at 256Hz and associated Nyquist frequency at 128Hz. The MEG signal was filtered with cut-off frequencies at 0.3 and 40Hz. The subjects were 3 male and 7 female volunteers in 25-40 years of age. Informed consent for the methodology and aim of the study was obtained from all participants prior to the procedure. The research was approved by the Research Committee of the Democritus University of Thrace (code number 80347). All patients were referred to our Laboratory of Medical Physics in Alexandroupoli, Greece, by practicing neurologists. They were off medication for 24 hours during their participation in the study. In our research we haven't include healthy subjects as controls because this study was previously done and published by Troebinger, et al. [19] in which we have used a double-blind experimental design with our pico- Tesla TMS electronic device [7] in order to look for an effect of pT-TMS in healthy subjects. All MEG data tracings were visually inspected carefully off-line for movement artifacts and periods contaminated with movement artifacts were cut off. The time taken for each recording was 2min in order to make sure alertness for each subject. Every patient was scanned in two separate sessions. During each MEG scan the subject had no task and was asked to sit comfortably in the MEG chair. The first session (session 1) consisted of a 2-minute resting state MEG scan. These data were consequently used to establish the subject’s alpha frequency in the range of (8-13 Hz), for calibration of the pT-TMS electronic device. In the second scanning session (session 2), the protocol was as follows: At all times the pT-TMS electronic device which is connected to the helmet was set to real or sham stimulation by a third party. Neither the researcher nor the participant were aware of the state of the device. First, 2 minutes of pre-stimulus baseline MEG data were recorded (run 1). Next, 2 minutes of real or sham pT-TMS stimulation were administered with the subject sitting comfortably just outside the scanner room. Following these 2 minutes of stimulation, a further 2 minutes of resting state MEG data were acquired (run 2). This was followed by another 2 minutes of stimulation- in this case the device was switched from sham to real or vice versa (by the third party)- and 2 more minutes of MEG scanning data were carried out (run 3).
The pT-TMS Electronic Device
The pT-TMS electronic device is a modified helmet containing up to 122 coils which are arranged in five array groups, so as to cover the main 7 brain regions (frontal, vertex, right and left temporal, right and left parietal, and occipital regions) of the subject. It is designed to create pT-TMS range modulations of magnetic flux in the alpha frequency range (8-13Hz) of each patient. The pT-TMS device was configured for each individual to generate a square wave (so as to resemble the firing activity of neurons in the brain). Anninos, et al. [12] modulated magnetic field at the individual’s mean peak alpha frequency - generated in the subject’s occipital lobe [7]. A schematic of the alpha wave generated by the electronic device can be seen in Anninos, et al. [17]. The electronic device has an extra hidden switch to disable current flow to the helmet coils. This switch, controlling real or sham stimulation, was operated by a member of the technical support team, so that neither the subject nor the experimenter were aware of whether sham or real stimulation was applied (double blind design).
Spectral Estimates
A software program was developed in our laboratory in order to detect the amplitude of the primary dominant frequency of the power spectra of the MEG recordings obtained from each depression patient and channel after the application of Fast Fourier Transform (FFT) (Figure 1). Then, it was interesting to look (alpha for calibration of the electronic device) and (2-7Hz, 8-13Hz and 14-24Hz for the analysis) and as it was stated above at the primary dominant frequency of the power spectra of the MEG recordings obtained from each patient and channel after the application of the FFT. In Figure 1 the actual signal length for analysis is 2 min and the FFT was applied only to 9secs, and in order to explain the primary dominant frequency it was necessary to use the Matlab program to magnify the spectrum. Thus, in the spectrum is not seen the whole frequency range which is 0-7 Hz ,but only see the range 0-5 Hz due to the magnification.
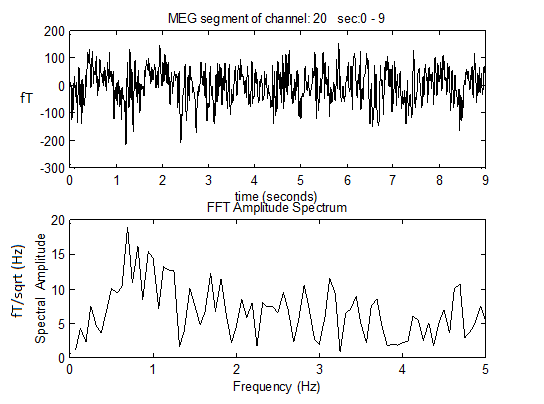
Figure 1: A) A MEG record of 9 sec obtained from a patient B) the application of FFT on the MEG record Analysis and Prediction of Sham and Stimulus Runs As it was indicated before in session 2 there are 3 data sets (run1, run2, run3) and the task is to identify where the sham stimulation was delivered (before recording run2 or before recording run3). Based on the frequency differences across all channel groups it was possible to make a prediction of the likely stage (run2 sham or run3 sham) of pT-TMS in each of the 10 recordings MEG depression patients.
The Prediction from Sham to Real Stimulation
In order to blindly identify real from sham stimulation it was necessary to predict the frequency increase due to pT-TMS from all recorded MEG channels. For this purpose it was needed to calculate the increase in primary dominant frequency from sham to real stimulation under two conditions. Having this in mind, then it can be estimated either the average frequency difference for each brain channel by calculating the differences between each average frequency of (run1+run3) / 2 from the run2 if run3 is the sham and run2 is the real stimulation or the average frequency differences of (run1+run2) / 2 from the run3 if the run2 is the sham and run3 is the real stimulation for the same patient in each brain channel as it is seen in the following equations 1 and 2.
We have attempted to determine the order of stimulation (run2 sham or run3 sham) based on the MPFD as shown in Table 1. On each of the 10 patients we based our predictions (run2 sham or run3 sham) on any order gave rise to the largest change in the MPFD from all MEG recorded channels. In Table 1, based on the knowledge of the true stimulation sequence, we can show the true effect of pT-TMS. Based on the binomial test, the probability for correctly selecting 9 or more events, each with a probability of 0.5, from 10 patients is highly statistical significant or at chance level (90%). This was correct in our case after unblinding as we can see in Table 1. Table 2 shows the brain regions and the corresponding channels in each brain region. Table 5 shows the symptoms in each of the 10 patients after the sham stimulation as were evaluated in interviews by clinicians the next day after the sham stimulation (2nd day in our lab), and the symptoms in each of the patients evaluated by clinicians one month after daily pT-TMS treatment at home.
Δf (2) = run 2 - (run1+run3)/2 (1)
Δf (3) = run3 - (run1+run2)/2 (2)
In these equations run1 is considered as the baseline MEG recordings, being the same for both calculations. In order to obtain all the above differences from all brain channels a software program was developed also in our laboratory (using equations 1 and 2) to estimate the MPFD of (Δf(2) or Δf(3)) for both calculations. If after all these calculations we have a MPFD from Δf(2) in (equation 1) to be greater for a particular patient then run2 is the real stimulation and run3 the sham stimulation or if the MPFD is greater from Δf(3) in (equation 2) then run3 is the real stimulation and the run2 will be the sham stimulation. We used two-tailed t- test for the statistical analysis of the results.
Results
| Patients Code | Run2 | Run3 | MPFD Hz | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Real stimulation | Sham stimulation | 0.003>-0.001 | ||||||||
| 2 | Real stimulation | Sham stimulation | 0.532>-0.325 | ||||||||
| 3 | Real stimulation | Sham stimulation | 0.754>-0.259 | ||||||||
| 4 | Real stimulation | Sham stimulation | No clear | ||||||||
| 5 | Sham stimulation | Real stimulation | 0.018<0.424 | ||||||||
| 6 | Sham stimulation | Real stimulation | -0.345<-0.09 | ||||||||
| 7 | Real stimulation | Sham stimulation | -0.410<-1.77 | ||||||||
| 8 | Real stimulation | Sham stimulation | 0.110>-0.421 | ||||||||
| 9 | Real stimulation | Sham stimulation | -0.011<-0.815 | ||||||||
| 10 | Sham stimulation | Real stimulation | 0.438<0.467 |
Table 1: This table shows the prediction to determine the order of stimulation (run2 sham or run3 sham) based on the MPFD in band 1 (2-7 Hz) as is described by equations 2 and 3. On each of the 10 depression patients the prediction was based (run2 sham or run3 sham) on whichever order gave rise to the largest change in MPFD from all MEG recorded channels. In patient 4 the MPFD was not clear and after unblinding the prediction was correct in 9/10(90%).
| Brain Regions | Channels | ||||
|---|---|---|---|---|---|
| Right Temporal | 1-14 ,111-120 | ||||
| Left Temporal | 43-50,55-62,67-74 | ||||
| Right Parietal | 5-6,11-16,97-100,109,110 ,115-122 | ||||
| Left Parietal | 47-52,59-64,71-74,79,80,87-90 | ||||
| Frontal | 17-42 | ||||
| Occipital | 75-86,91-96, 101-110 | ||||
| Vertex | 13-16,49-54,61-66,73,74,89,90,99,100, 117-122 |
The time frame of our clinical investigations was as follows: 1st day: MEG measurements in our lab (baseline run1).Application of sham stimulation and MEG recordings afterwards (run3). We found no significant differences in the patients' MEG spectrum.
2nd day: Interview by clinicians after the sham stimulation (Table 5). Application of real pT-TMS and MEG recordings afterwards (run2). The patients' MEG spectrum was almost like normal in the majority of them with absence most of the abnormal frequencies.
3rd day: Interview by clinicians after real stimulation. They confirmed our findings of our MEG recordings.
10th day: MEG recordings and evaluation by clinicians Table 5 shows the symptoms in each patient before pT- TMS and after sham stimulation, and the symptoms after the real pT-TMS stimulation after one month as were evaluated by interview by clinicians. In order to determine the maximum effect of stimulation for each of the 7 brain regions we based our results to the maximum on the MPFD for all patients. Thus, in Table 3 and Table 4 are shown the MPFD in Hz from Real(run2 in Δf(2)) to Sham(run3 in Δf(3)) and Real(run3 in Δf(3)) to Sham(run2 in Δf(2)) stimulation respectively for each of the 7 brain regions as it is stated in Table 2 for all patients. Tables 6, 7, represent the statistical analysis for the 10 patients. The results were statistically significant at the level of 0.05. We observed that the results of 4 out of 10 patients were statistically significant (40%).
| P | RT | RT | LT | LT | RP | RP | LP | LP | F | F | V | V | O | O | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Run2 real MPFD | Run3 sham MPFD | Run2 real MPFD | Run3 sham MPFD | Run2 real MPFD | Run3 sham MPFD | Run2 real MPFD | Run3 sham MPFD | Run2 real MPFD | Run3 sham MPFD | Run2 real MPFD | Run3 sham MPFD | Run2 real MPFD | Run3 sham MPFD | |||||||||||||||||||||||||||||
| 1 | 5.5 | 2.59 | 3.06 | 3.09 | 5.5 | 2.38 | 3.19 | 3.09 | 2.31 | 1.5 | 5.5 | 3.69 | 4.75 | 3.97 | ||||||||||||||||||||||||||||
| 2 | 5.16 | 2.34 | 2.31 | 4.53 | 5.16 | 2.06 | 4.69 | 4.94 | 4.75 | 1.78 | 5.16 | 4.94 | 5.66 | 4.66 | ||||||||||||||||||||||||||||
| 3 | 4.34 | 3.53 | 5.44 | 5.75 | 5.03 | 3.41 | 5.44 | 1.19 | 2.97 | 2.97 | 5.44 | 1.19 | 4.81 | 5.03 | ||||||||||||||||||||||||||||
| 4 | 4.38 | 1.5 | 4.03 | 4.72 | 4.38 | 4 | 4.03 | 3.75 | 4.84 | 3.69 | 4.03 | 4 | 5.19 | 4.59 | ||||||||||||||||||||||||||||
| 7 | 4.72 | 0.19 | 1.34 | 0.88 | 4.72 | 1.84 | 1.34 | 0.19 | 4.75 | 2.38 | 3.25 | 0.72 | 4.13 | 1.09 | ||||||||||||||||||||||||||||
| 8 | 4.19 | 5.31 | 4.38 | 3.75 | 3.75 | 5.31 | 4.38 | 3.75 | 3.13 | 1.44 | 1.44 | 5.31 | 4.81 | 0.44 | ||||||||||||||||||||||||||||
| 9 | 5.38 | 2.56 | 3.69 | 4.38 | 5.38 | 1.94 | 2.5 | 4.75 | 5.06 | 3.94 | 5.38 | 3.44 | 4.19 | 4.75 |
Table 3: This Table is shown the maximum effect of the MPFD in real and sham stimulations for each of the 1,2,3,4,7,8 and 9 patie
Table 3: This Table is shown the maximum effect of the MPFD in real and sham stimulations for each of the 1,2,3,4,7,8 and 9 patients, according to the order of stimulation (run2 sham or run3 sham) in Table 1 . (P: patient number, RT: right temporal, LT: left temporal, RP: right parietal, LP : left parietal, F : frontal, V : vertex , O: occipital ).
| P | RT | RT | LT | LT | RP | RP | LP | LP | F | F | V | V | O | O | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Run3 Real MPFD | Run2 sham MPFD | Run3 Real MPFD | Run2 sham MPFD | Run3 Real MPFD | Run sham MPFD | Run3 Real MPFD | Run2 sham MPFD | Run3 Real MPFD | Run2 Sham MPFD | Run3 Real MPFD | Run2 sham MPFD | Run3 Real MPFD | Run2 Sham MPFD | |||||||||||||||||||||||||||||
| 5 | 4.88 | 3.69 | 4.38 | 1.69 | 4.69 | 3.44 | 4.75 | 1.81 | 3.88 | 4.31 | 3.56 | 4.5 | 5.56 | 4.13 | ||||||||||||||||||||||||||||
| 6 | 2.63 | 3.22 | 4.75 | 4.03 | 3 | 3.22 | 4.72 | 4.22 | 3.97 | 3.94 | 4.72 | 4.22 | 4.41 | 2.56 | ||||||||||||||||||||||||||||
| 10 | 4.44 | 4.31 | 3 | 2.5 | 4.44 | 4.31 | 3 | 4.81 | 4.94 | 3.25 | 4.44 | 4.31 | 4 | 5.5 |
Table 4: This table shows the maximum effect of the MPFD from Real (run3 in Δ (f (3)) to Sham(run2 in Δf (2)) stimulations for ea
1. (P: patient number, RT: right temporal, LT: left temporal, RP: right parietal, LP: left parietal, F: frontal, V: vertex, O: occipital).
| Patient | Sex | Symptoms before pT-TMS | Symptoms after sham pT-TMS | Symptoms after pT-TMS | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F | 1.Depressed mood, Score 3 | 1.Depressed mood, Score 2 | 1. Absent, Score 0 | ||||||||||
| 2.Feelings of Guilt, Score 3 | 2.Feelings of Guilt, Score 2 | 2. Absent, Score 0 | ||||||||||||
| 3.Suicide, Score 1 | 3.Suicide, Score 1 | 3. Absent, Score 0 | ||||||||||||
| 4.Insomnia early, Score 1 | 4.Insomnia early, Score 1 | 4. Insomnia early, Score 0 | ||||||||||||
| 5.Insomnia imiddle, Score 1 | 5.Insomnia middle, Score 1 | 5.Insomnia middle, Score 0 | ||||||||||||
| 6.Insomnia Late, Score 2 | 6.Insomnia Late, Score 2 | 6.Insomnia Late, Score 0 | ||||||||||||
| 7.Work and Activities, Score 2 | 7.Work and Activities, Score 2 | 7.Work and Activities, Score 0 | ||||||||||||
| 8. Retardation, Score 1 | 8. Retardation, Score 1 | 8. Retardation, Score 0 | ||||||||||||
| 9. Agitation, Score 2 | 9. Agitation, Score 2 | 9. Agitation, Score 1 | ||||||||||||
| 10. Anxiety(psychological),Score 2 | 10. Anxiety(psychological), Score 1 | 10.Anxiety(psychological), Score 0 | ||||||||||||
| 11. Anxiety(somatic), Score 1 | 11. Anxiety(somatic), Score 1 | 11. Anxiety(somatic), Score 1 | ||||||||||||
| 12. Somatic symptoms(gastrointestinal), Score 1 | 12. Somatic symptoms(gastrointestinal), Score 1 | 12. Somatic symptoms(gastrointestinal), Score 0 | ||||||||||||
| 13.Somatic symptoms general, Score 1 | 13.Somatic symptoms general, Score 1 | 13.Somatic symptoms general, Score 0 | ||||||||||||
| 14. Genital symptoms, Score 1 | 14. Genital symptoms, Score 1 | 14. Genital symptoms, Score 1 | ||||||||||||
| 15.Hypochondriasis, Score 3 | 15.Hypochondriasis, Score 3 | 15.Hypochondriasis, Score 0 | ||||||||||||
| 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 0 | ||||||||||||
| 17. Insight, Score 1 | 17. Insight, Score 1 | 17. Insight, Score 0 | ||||||||||||
| 2 | F | 1.Depressed mood, Score 1 | 1.Depressed mood, Score 1 | 1. Absent, Score 0 | ||||||||||
| 2.Feelings of Guilt, Score 1 | 2.Feelings of Guilt, Score 1 | 2. Absent, Score 0 | ||||||||||||
| 3.Suicide, Score 0 | 3.Suicide, Score 1 | 3. Absent, Score 0 | ||||||||||||
| 4.Insomnia early, Score 1 | 4.Insomnia early, Score 1 | 4. Insomnia early, Score 0 | ||||||||||||
| 5.Insomnia middle, Score 1 | 5.Insomnia middle, Score 1 | 5.Insomnia middle, Score 0 | ||||||||||||
| 6.Insomnia Late, Score 1 | 6.Insomnia Late, Score 1 | 6.Insomnia Late, Score 0 | ||||||||||||
| 7.Work and Activities, Score 1 | 7.Work and Activities, Score 1 | 7.Work and Activities, Score 0 | ||||||||||||
| 8. Retardation, Score 1 | 8. Retardation, Score 1 | 8. Retardation, Score 1 | ||||||||||||
| 9. Agitation, Score 3 | 9. Agitation, Score 2 | 9. Agitation, Score 1 | ||||||||||||
| 10. Anxiety(psychological), Score 1 | 10. Anxiety(psychological),Score 1 | 10.Anxiety(psychological),Score 0 | ||||||||||||
| 11. Anxiety(somatic), Score 1 | 11. Anxiety(somatic),Score 1 | 11. Anxiety(somatic),Score 1 | ||||||||||||
| 12. Somatic symptoms(gastrointestinal), Score 1 | 12. Somatic symptoms(gastrointestinal),Score 1 | 12. Somatic symptoms(gastrointestinal),Score 0 | ||||||||||||
| 13.Somatic symptoms general, Score 1 | 13.Somatic symptoms general, Score 1 | 13.Somatic symptoms general, Score 0 | ||||||||||||
| 14. Genital symptoms, Score 1 | 14. Genital symptoms, Score 1 | 14. Genital symptoms, Score 1 | ||||||||||||
| 15.Hypochondriasis, Score 2 | 15.Hypochondriasis,Score 3 | 15.Hypochondriasis,Score 0 | ||||||||||||
| 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 1 | ||||||||||||
| 17. Insight, Score 0 | 17. Insight, Score 1 | 17. Insight, Score 0 | ||||||||||||
| 3 | M | 1.Depressed mood, Score 3 | 1.Depressed mood, Score 2 | 1. Absent, Score 0 | ||||||||||
| 2.Feelings of Guilt, Score 1 | 2.Feelings of Guilt, Score 1 | 2 .Absent, Score 0 | ||||||||||||
| 3.Suicide,Score 1 | 3.Suicide,Score 1 | 3. Absent, Score 0 | ||||||||||||
| 4.Insomnia early, Score 2 | 4.Insomnia early, Score 2 | 4. Insomnia early, Score 0 | ||||||||||||
| 5.Insomnia middle, Score 1 | 5.Insomnia middle, Score 1 | 5.Insomnia middle, Score 0 | ||||||||||||
| 6.Insomnia Late, Score 2 | 6.Insomnia Late, Score 2 | 6.Insomnia Late, Score 0 | ||||||||||||
| 7.Work and Activities, Score 1 | 7.Work and Activities, Score 1 | 7.Work and Activities, Score 0 | ||||||||||||
| 8. Retardation, Score 1 | 8. Retardation, Score 1 | 8. Retardation, Score 0 | ||||||||||||
| 9. Agitation, Score 3 | 9. Agitation, Score 2 | 9. Agitation, Score 0 | ||||||||||||
| 10. Anxiety(psychological),Score 1 | 10. Anxiety(psychological),Score 1 | 10.Anxiety(psychological),Score 1 |
| 11. Anxiety(somatic),Score 2 | 11. Anxiety(somatic),Score 2 | 11. Anxiety(somatic),Score 1 | ||
|---|---|---|---|---|
| 12. Somatic symptoms(gastrointestinal),Score 1 | 12. Somatic symptoms(gastrointestinal),Score 1 | 12. Somatic symptoms(gastrointestinal),Score 0 | ||
| 13.Somatic symptoms general, Score 1 | 13.Somatic symptoms general, Score 1 | 13.Somatic symptoms general, Score 0 | ||
| 14. Genital symptoms, Score 1 | 14. Genital symptoms, Score 1 | 14. Genital symptoms, Score 0 | ||
| 15.Hypochondriasis,Score 1 | 15.Hypochondriasis,Score 1 | 15.Hypochondriasis,Score 0 | ||
| 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 0 | ||
| 17. Insight, Score 1 | 17. Insight, Score 1 | 17. Insight, Score 0 | ||
| 4 | M | 1.Depressed mood, Score 3 | 1.Depressed mood, Score 3 | 1. Absent, Score 0 |
| 2.Feelings of Guilt, Score 1 | 2.Feelings of Guilt, Score 1 | 2. Absent, Score 0 | ||
| 3.Suicide,Score 0 | 3.Suicide,Score 1 | 3. Absent, Score 0 | ||
| 4.Insomnia early, Score 1 | 4.Insomnia early, Score 1 | 4. Insomnia early, Score 0 | ||
| 5.Insomnia middle, Score 1 | 5.Insomnia middle, Score 1 | 5.Insomnia middle, Score 0 | ||
| 6.Insomnia Late, Score 1 | 6.Insomnia Late, Score 1 | 6.Insomnia Late, Score 0 | ||
| 7.Work and Activities, Score 1 | 7.Work and Activities, Score 1 | 7.Work and Activities, Score 1 | ||
| 8. Retardation, Score 1 | 8. Retardation, Score 1 | 8. Retardation, Score 0 | ||
| 9. Agitation, Score 2 | 9. Agitation, Score 2 | 9. Agitation, Score 0 | ||
| 10. Anxiety(psychological),Score 1 | 10. Anxiety(psychological),Score 1 | 10.Anxiety(psychological),Score 1 | ||
| 11. Anxiety(somatic),Score 1 | 11. Anxiety(somatic),Score 1 | 11. Anxiety(somatic), Score 1 | ||
| 12. Somatic symptoms(gastrointestinal),Score 0 | 12. Somatic symptoms(gastrointestinal),Score 0 | 12. Somatic symptoms(gastrointestinal), Score 0 | ||
| 13.Somatic symptoms general, Score 1 | 13.Somatic symptoms general ,Score 1 | 13.Somatic symptoms general, Score 0 | ||
| 14. Genital symptoms, Score 1 | 14. Genital symptoms, Score 1 | 14. Genital symptoms, Score 0 | ||
| 15.Hypochondriasis,Score 1 | 15.Hypochondriasis,Score 1 | 15.Hypochondriasis, Score 0 | ||
| 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 0 | ||
| 17. Insight, Score 1 | 17. Insight, Score 1 | 17. Insight, Score 0 | ||
| 5 | F | 1.Depressed mood, Score 1 | 1.Depressed mood, Score 1 | 1. Absent, Score 0 |
| 2.Feelings of Guilt, Score 1 | 2.Feelings of Guilt, Score 1 | 2. Absent, Score 0 | ||
| 3.Suicide,Score 0 | 3.Suicide,Score 0 | 3. Absent, Score 0 | ||
| 4.Insomnia early, Score 1 | 4.Insomnia early, Score 1 | 4. Insomnia early, Score 0 | ||
| 5.Insomnia middle, Score 1 | 5.Insomnia middle, Score 1 | 5.Insomnia middle, Score 0 | ||
| 6.Insomnia Late, Score 1 | 6.Insomnia Late, Score 1 | 6.Insomnia Late, Score 0 | ||
| 7.Work and Activities, Score 1 | 7.Work and Activities, Score 1 | 7.Work and Activities, Score 0 | ||
| 8. Retardation, Score 1 | 8. Retardation, Score 1 | 8. Retardation, Score 1 | ||
| 9. Agitation, Score 2 | 9. Agitation, Score 2 | 9. Agitation, Score 0 | ||
| 10. Anxiety(psychological), Score 1 | 10. Anxiety(psychological), Score 1 | 10.Anxiety(psychological), Score 1 | ||
| 11. Anxiety(somatic), Score 1 | 11. Anxiety(somatic),Score 1 | 11. Anxiety(somatic), Score 1 | ||
| 12. Somatic symptoms(gastrointestinal), Score 1 | 12. Somatic symptoms(gastrointestinal), Score 1 | 12. Somatic symptoms(gastrointestinal), Score 0 | ||
| 13.Somatic symptoms general, Score 1 | 13.Somatic symptoms general, Score 1 | 13.Somatic symptoms general, Score 0 | ||
| 14. Genital symptoms, Score 1 | 14. Genital symptoms, Score 1 | 14. Genital symptoms, Score 0 | ||
| 15.Hypochondriasis,Score 2 | 15.Hypochondriasis,Score 2 | 15.Hypochondriasis, Score 0 | ||
| 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 0 | ||
| 17. Insight, Score 1 | 17. Insight, Score 1 | 17. Insight, Score 0 | ||
| 6 | F | 1.Depressed mood, Score 2 | 1.Depressed mood, Score 2 | 1. Absent, Score 1 |
| 2.Feelings of Guilt, Score 1 | 2.Feelings of Guilt, Score 1 | 2. Absent, Score 0 | ||
| 3.Suicide, Score 0 | 3.Suicide, Score 0 | 3. Absent, Score 0 | ||
| 4.Insomnia early, Score 1 | 4.Insomnia early, Score 1 | 4. Insomnia early, Score 1 | ||
| 5.Insomnia middle, Score 1 | 5.Insomnia middle, Score 1 | 5.Insomnia middle, Score 1 | ||
| 6.Insomnia Late, Score 2 | 6.Insomnia Late, Score 1 | 6.Insomnia Late, Score 1 | ||
| 7.Work and Activities, Score 1 | 7.Work and Activities, Score 1 | 7.Work and Activities, Score 0 | ||
| 8. Retardation, Score 1 | 8. Retardation, Score 1 | 8. Retardation, Score 0 | ||
| 9. Agitation, Score 2 | 9 .Agitation, Score 1 | 9. Agitation, Score 0 | ||
| 10. Anxiety(psychological), Score 1 | 10. Anxiety(psychological),Score 1 | 10.Anxiety(psychological), Score 0 | ||
| 11. Anxiety(somatic), Score 1 | 11. Anxiety(somatic), Score 1 | 11. Anxiety(somatic), Score 0 | ||
| 12. Somatic symptoms(gastrointestinal), Score 1 | 12. Somatic symptoms(gastrointestinal), Score 1 | 12. Somatic symptoms(gastrointestinal), Score 0 | ||
| 13.Somatic symptoms general, Score 1 | 13.Somatic symptoms general, Score 1 | 13.Somatic symptoms general, Score 0 | ||
| 14. Genital symptoms, Score 1 | 14. Genital symptoms, Score 1 | 14. Genital symptoms, Score 0 | ||
| 15.Hypochondriasis,Score 2 | 15.Hypochondriasis,Score 2 | 15.Hypochondriasis, Score 0 | ||
| 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 0 | ||
| 17. Insight, Score 1 | 17. Insight, Score 1 | 17. Insight, Score 0 | ||
| 7 | F | 1.Depressed mood, Score 1 | 1.Depressed mood, Score 1 | 1. Absent, Score 0 |
| 2.Feelings of Guilt, Score 1 | 2.Feelings of Guilt, Score 1 | 2. Absent, Score 0 | ||
| 3.Suicide,Score 0 | 3.Suicide,Score 0 | 3. Absent, Score 0 | ||
| 4.Insomnia early, Score 1 | 4.Insomnia early, Score 1 | 4. Insomnia early, Score 1 | ||
| 5.Insomnia middle, Score 1 | 5.Insomnia middle, Score 1 | 5.Insomnia middle, Score 1 | ||
| 6.Insomnia Late, Score 2 | 6.Insomnia Late, Score 1 | 6.Insomnia Late, Score 1 | ||
| 7.Work and Activities, Score 1 | 7.Work and Activities, Score 1 | 7.Work and Activities, Score 0 | ||
| 8. Retardation, Score 1 | 8. Retardation, Score 1 | 8. Retardation, Score 0 | ||
| 9. Agitation, Score 3 | 9. Agitation, Score 2 | 9. Agitation, Score 0 | ||
| 10. Anxiety(psychological),Score 2 | 10. Anxiety(psychological),Score 1 | 10.Anxiety(psychological),Score 0 | ||
| 11. Anxiety(somatic),Score 1 | 11. Anxiety(somatic),Score 1 | 11. Anxiety(somatic), Score 0 | ||
| 12. Somatic symptoms(gastrointestinal),Score 1 | 12. Somatic symptoms(gastrointestinal),Score 1 | 12. Somatic symptoms(gastrointestinal), Score 0 | ||
| 13.Somatic symptoms general, Score 1 | 13.Somatic symptoms general, Score 1 | 13.Somatic symptoms general, Score 0 | ||
| 14. Genital symptoms, Score 1 | 14. Genital symptoms, Score 1 | 14. Genital symptoms, Score 0 | ||
| 15.Hypochondriasis,Score 2 | 15.Hypochondriasis,Score 2 | 15.Hypochondriasis, Score 0 | ||
| 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 0 | ||
| 17. Insight, Score 1 | 17. Insight, Score 1 | 17. Insight, Score 0 | ||
| 8 | F | 1.Depressed mood, Score 1 | 1.Depressed mood, Score 1 | 1. Absent, Score 1 |
| 2.Feelings of Guilt, Score 1 | 2.Feelings of Guilt, Score 1 | 2. Absent,, Score 0 | ||
| 3.Suicide,Score 0 | 3.Suicide,Score 0 | 3. Absent, Score 0 | ||
| 4.Insomnia early, Score 1 | 4.Insomnia early, Score 1 | 4. Insomnia early, Score 1 | ||
| 5.Insomnia middle, Score 1 | 5.Insomnia middle, Score 1 | 5.Insomnia middle, Score 1 | ||
| 6.Insomnia Late, Score 2 | 6.Insomnia Late, Score 1 | 6.Insomnia Late, Score 1 | ||
| 7.Work and Activities, Score 1 | 7.Work and Activities, Score 1 | 7.Work and Activities, Score 0 | ||
| 8. Retardation, Score 1 | 8. Retardation, Score 1 | 8. Retardation, Score 0 | ||
| 9. Agitation, Score 3 | 9. Agitation, Score 2 | 9. Agitation, Score 0 | ||
| 10. Anxiety(psychological), Score 2 | 10. Anxiety(psychological), Score 1 | 10.Anxiety(psychological), Score 0 | ||
| 11. Anxiety(somatic),Score 1 | 11. Anxiety(somatic),Score 1 | 11. Anxiety(somatic),Score 0 | ||
| 12. Somatic symptoms(gastrointestinal),Score 1 | 12. Somatic symptoms(gastrointestinal),Score 1 | 12. Somatic symptoms(gastrointestinal),Score 0 | ||
| 13.Somatic symptoms general, Score 1 | 13.Somatic symptoms general, Score 1 | 13.Somatic symptoms general, Score 0 | ||
| 14. Genital symptoms ,Score 1 | 14. Genital symptoms, Score 1 | 14. Genital symptoms, Score 0 | ||
| 15.Hypochondriasis,Score 2 | 15.Hypochondriasis,Score 1 | 15.Hypochondriasis,Score 0 | ||
| 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 0 | ||
| 17. Insight, Score 1 | 17. Insight, Score 1 | 17. Insight ,Score 0 | ||
| 9 | F | 1.Depressed mood, Score 1 | 1.Depressed mood, Score 1 | 1.Depressed mood, Score 0 |
| 2.Feelings of Guilt, Score 1 | 2.Feelings of Guilt, Score 1 | 2.Feelings of Guilt, Score 0 | ||
| 3.Suicide,Score 0 | 3.Suicide,Score 0 | 3.Suicide,Score 0 | ||
| 4.Insomnia early, Score 1 | 4.Insomnia early, Score 1 | 4.Insomnia early, Score 0 | ||
| 5.Insomnia middle, Score 1 | 5.Insomnia middle, Score 1 | 5.Insomnia middle, Score 0 | ||
| 6.Insomnia Late, Score 2 | 6.Insomnia Late, Score 1 | 6.Insomnia Late, Score 0 | ||
| 7.Work and Activities, Score 1 | 7.Work and Activities, Score 1 | 7.Work and Activities, Score 1 | ||
| 8. Retardation, Score 1 | 8. Retardation, Score 1 | 8. Retardation, Score 0 | ||
| 9. Agitation, Score 3 | 9. Agitation, Score 2 | 9. Agitation, Score 1 | ||
| 10. Anxiety(psychological), Score 2 | 10. Anxiety(psychological), Score 1 | 10. Anxiety(psychological), Score 0 | ||
| 11. Anxiety(somatic), Score 1 | 11. Anxiety(somatic), Score 1 | 11. Anxiety(somatic), Score 0 | ||
| 12. Somatic symptoms(gastrointestinal), Score 1 | 12. Somatic symptoms(gastrointestinal), Score 1 | 12. Somatic symptoms(gastrointestinal), Score 0 | ||
| 13.Somatic symptoms general, Score 1 | 13.Somatic symptoms general, Score 1 | 13.Somatic symptoms general, Score 0 | ||
| 14. Genital symptoms, Score 1 | 14. Genital symptoms, Score 1 | 14. Genital symptoms, Score 1 | ||
| 15.Hypochondriasis,Score 2 | 15.Hypochondriasis,Score 1 | 15.Hypochondriasis,Score 0 | ||
| 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 0 | ||
| 17. Insight, Score 1 | 17. Insight, Score 1 | 17. Insight, Score 0 | ||
| 10 | M | 1.Depressed mood, Score 1 | 1.Depressed mood, Score 1 | 1.Depressed mood, Score 0 |
| 2.Feelings of Guilt, Score 1 | 2.Feelings of Guilt, Score 1 | 2.Feelings of Guilt, Score 0 | ||
| 3.Suicide,Score 1 | 3.Suicide,Score 1 | 3.Suicide,Score 0 | ||
| 4.Insomnia early, Score 1 | 4.Insomnia early, Score 1 | 4.Insomnia early, Score 0 | ||
| 5.Insomnia middle, Score 1 | 5.Insomnia middle, Score 1 | 5.Insomnia middle, Score 0 | ||
| 6.Insomnia Late, Score 2 | 6.Insomnia Late, Score 1 | 6.Insomnia Late, Score 0 | ||
| 7.Work and Activities, Score 1 | 7.Work and Activities, Score 1 | 7.Work and Activities, Score 0 | ||
| 8. Retardation, Score 1 | 8. Retardation, Score 1 | 8. Retardation, Score 0 | ||
| 9. Agitation, Score 3 | 9. Agitation, Score 2 | 9. Agitation, Score 0 | ||
| 10. Anxiety(psychological), Score 2 | 10. Anxiety(psychological), Score 1 | 10. Anxiety(psychological), Score 0 | ||
| 11. Anxiety(somatic), Score 1 | 11. Anxiety(somatic), Score 1 | 11. Anxiety(somatic), Score 1 | ||
| 12. Somatic symptoms(gastrointestinal),Score 1 | 12. Somatic symptoms(gastrointestinal),Score 1 | 12. Somatic symptoms(gastrointestinal),Score 0 | ||
| 13.Somatic symptoms general, Score 1 | 13.Somatic symptoms general, Score 1 | 13.Somatic symptoms general, Score 0 | ||
| 14. Genital symptoms, Score 1 | 14. Genital symptoms, Score 1 | 14. Genital symptoms, Score 1 | ||
| 15.Hypochondriasis,Score 2 | 15.Hypochondriasis,Score 1 | 15.Hypochondriasis,Score 0 | ||
| 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 1 | 16.Loss of Weight, Score 0 | ||
| 17. Insight, Score 1 | 17. Insight, Score 1 | 17. Insight, Score 0 |
- Table 5: This table shows the symptoms for the Hamilton Rating Scale for the 10 depression patients before and after sham pT-TMS as were evaluated by interview by clinicians the next day (2nd day in our lab) and after pT-TMS as were evaluated by interview by clinicians one month after daily pT-TMS treatment at home (F:female; M:male).
- Patients
- RUN2(REAL) t-test
- P values
- 1
- 4,25±1,36
- 2,90±0,83
- 0,04
- 2
- 4,69±1,10
- 3,60±1,46
- 0,14
- 3
- 4,84±0,90
- 3,24±1,76
- 0,05
- 4
- 4,41±0,45
- 3,75±1,06
- 0,15
- 7
- 3,46±1,54
- 0,98±0,89
- 0.003
- 8
- 3,72±1,14
- 3,61±1,97
- 0.9
- 9
- 4,51±1,10
- 3,68±1,09
- 0.18
- Mean ± SD
- The results are statistical significant at the level of 0.05 (marked bold).
- Patients
- RUN3(REAL) t-test
- P values
- 5
- 4,52±0,66
- 3,36±1,16
- 0,04
- 6
- 4,02±0,87
- 3,63±0,63
- 0,35
- 10
- 4,03±0,75
- 4,14±0,98
- 0,82
- Mean ± SD
Table 7: Statistical analysis for the 7 patients of Table 3.
The results are statistical significant at the level of 0.05 (marked bold).
Discussion
About 30% of patients suffering from a main depressive disorder do not respond adequately to the established pharmacological, psychotherapeutic, or somatic treatments. Advances in technology and promising knowledge about the dysfunctional brain circuits underlying depression have led to the development of different neuromodulation techniques [24] .In the early 1990s, studies revealed that it is potential to evoke long term mood changes in healthy volunteers by rapid rate repetitive TMS (rTMS) over the frontal cortex. Subsequent studies involving depressed patients found frontal cortical rTMS administered daily to be clinically efficient. A broadly accepted technique that would present the highest efficacy, with the best acceptability has not been established so far. In order to come close to this purpose, the most significant factors to be addressed by more studies are: localization, frequency, intensity, concurrent medication, maintenance treatments, number of pulses, trains, unilateral, or bilateral mode of application [25]. During the last two decades TMS was applied in therapy of mood disorders and psychoses more on the principle of consuetude, than confirmations of the obvious effectiveness. However lately a group of experts presented a study, in which they regarded TMS as the effective method in therapy of depression and schizophrenia [26]. Sabesan, et al. [27] investigated TMS on geriatric depression. They identified several factors other than age that moderate the observed variations in the efficacy of rTMS in the elderly. Andrews, et al. [28] concluded that the effect of the TMS-induced cortico spinal excitation on post activation depression may be explained by a combination of pre- and postsynaptic mechanisms. Opie, et al. [29] investigated task-related changes in intra cortical inhibition assessed with paired- and triple-pulse TMS.
We have attempted to influence the depression patients with the pT-TMS electronic device [7]. The coils of the device were constructed to emit back to the brain magnetic fields of appropriate intensities and frequencies to those emitted prior to the application of pT-TMS. This resulted in a decrease of the maximal magnetic power emitted from these areas and an attenuation of the depression disorder activity. It is known that magnetic fields modify the activity of the pineal gland, which has been shown to control dopaminergic, and endogenous opioid functions [30]. On a cellular level, the consequences of magnetic fields on depression activity may be related to alterations in properties and stability of biological membranes and their transport characteristics including their intra- and extra cellular distributions and flux of calcium ions [22]. Chervyakov, et al. [31] in a review article analyzed the potential mechanisms underlying the therapeutic effects of TMS. They concluded that the total therapeutic effects of repetitive TMS may be determined by their total impact on a number of processes in the brain, including long-term potentiation, long-term depression, changes in cerebral blood flow, the activity of certain enzymes, interactions between cortical and sub cortical structures, and gene expression. Troebinger, et al. [19] have used a double-blind experimental design to look for an effect of our pT-TMS electronic device [7] on healthy subjects. They measured resting state MEG brain activity. After unblinding, they found no significant effect of an increase in the frequency range (2-7 Hz) across the subject group. This was due to the fact that from the 14 healthy subjects that was involved in the study only 8 were characterized with frequencies (2-7 Hz) and exhibited the effect of pT-TMS. In this study was set out to reproduce the effects of the increased abnormal dominant frequencies of 2-7 Hz band due to the effect of the pT -TMS in patients with depression. Our experimental design was double-blind and our predictions were based of the true order of stimulation and on the MPFD in the data. After unblinding it was found that correctly predicted the order of stimulation in 9 out of 10 patients. This prediction was in line with what one would expect by chance. The following day's examination (2nd, 3rd day) with the MEG showed that their spectrum was almost like normal with absent most of the high abnormal frequencies in the 2-7Hz frequency band. All depression patients were evaluated clinically and with the MEG a week after the first application of the pT-TMS in our lab (10th day). Most of the patients reported a progressive worsening to their pretreatment status. To conclude if the responses elicited in our lab were reproducible, it was advised the patients to apply the pT-TMS treatment every night (23.00 pm) at home. After one month nightly application of pT-TMS at home, all depression patients were assessed again and the majority of them reported to have benefit from this treatment (Table 5).
Conclusion
This method of the pT-TMS has potential effects to be a significant non invasive secure and effectual modality in the managing of depression patients. Nevertheless, further research with more patients are required in order to evaluate its potential important contribution for managing the symptoms of depression patients.
Acknowledgement
Funding for this work was provided by a collaboration of GGET (General Secretariat of Research and Technology, GR) and ERGO AEBE, INC, GR under the research program titled "Foundation of a Laboratories Network and purchase of a Multichannel Biomagnetometer SQUID (Superconducting Quantum Interference Device), in order to develop an expert system for automatic acquisition, analysis, evaluation and exploitation of MEG signals that are emitted from different organs of the human body" (Grant Number: 80623).
Conflict of Interest
The authors declare that they have no conflict of interest.
References
-
Gibson TB, Jing Y, Smith Carls G, Kim E, Bagalman JE, et al. (2010) Cost burden of treatment resistance in patients with depression. Am J Manag Care 16(5): 370-377.
-
Ivanova JI, Birnbaum HG, Kidolezi Y, Subramanian G, Khan SA, et al. (2010) Direct and indirect costs of employees with treatment-resistant and non- treatment resistant major depressive disorder. Curr Med Res Opin 26(10): 2475-2484.
-
Trivedi MH, Rush AJ, Wisniewski SR, Nierenberg AA, Warden D, et al. (2006) Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice. Am J Psychiatry 163(1): 28-40.
-
Kennedy SH, Giacobbe P (2007) Treatment resistant depression-Advances in somatic therapies. Ann Clin Psychiatry 19(4): 279-287.
-
Kennedy SH, Milev R, Giacobbe P, Ramasubbu R, Lam RW, et al. (2009) Canadian Network for Mood and Anxiety Treatments CANMAT Clinical guidelines for the management of major depressive disorder in adults. IV. Neurostimulation therapies. J Affect Disord 117(Suppl 1): S44-S53.
-
Barker AT, Jalinous R, Freeston IL (1985) Non - invasive magnetic stimulation of human motor cortex. Lancet 1(8437): 1106-1107.
-
Anninos PA, Tsagas N (1995) Electronic apparatus for treating epileptic individuals. Sept 26
-
Anninos P, Adamopoulos A, Kotini A, Tsagas N, Tamiolakis D, et al. (2007) MEG evaluation of Parkinson's diseased patients after external magnetic stimulation. Acta Neurol Belg 107(1): 5-10.
-
Anninos P, Kotini A, Anninou N, Adamopoulos A, Papastergiou A, et al. (2008) MEG recordings of patients with CNS disorders before and after external magnetic stimulation. J Integr Neurosci 7(1): 17-27.
-
Anninos P, Kotini A, Tamiolakis D, Tsagas N (2006) Transcranial magnetic stimulation A case report and review of the literature. Acta Neurol Belg 106(1): 26- 30.
-
Anninos PA, Adamopoulos AV, Kotini A, Tsagas N (2000) Nonlinear analysis of brain activity in magnetic influenced Parkinson patients. Brain Topogr 13(2): 135-144.
-
Anninos PA, Beek B, Csermely TJ, Harth EM, Pertile G (1970) Dynamics of neural structures. J Theor Biol 26(1): 121-148.
-
Anninos PA, Tsagas N, Adamopoulos A (1989) A brain model theory for epilepsy and the mechanism for treatment with experimental verification using SQUID measurements. In: Cotterill RM(Ed) Models of brain function. New York, Cambridge University Press, pp: 405-421.
-
Anninos P, Adamopoulos A, Kotini A (2015) MEG as a Medical Diagnostic Tool in the Greek Population. Acta Medica (Hradec Kralove) 58(3): 71-78.
-
Anninos P, Kotini A, Adamopoulos A, Tsagas N (2003) Magnetic stimulation can modulate seizures in epileptic patients. Brain Topogr 16(1): 57-64.
-
Anninos PA, Tsagas N, Jacobson JI, Kotini A (1999) The biological effects of magnetic stimulation in epileptic patients. Panminerva Med 41(3): 207-215.
-
Anninos PA, Tsaga N, Sandyk R, Derpapas K (1991) Magnetic stimulation in the treatment of partial seizures. Int J Neurosci 60(3-4): 141-171.
-
Kotini A, Anninos P (2016) Alpha delta and theta rhythms in a neural net model Comparison with MEG data. J Theor Biol 388: 11-14.
-
Troebinger L, Anninos P, Barnes G (2015) Neuromagnetic effects of pico-Tesla stimulation. Physiol Meas 36(9): 1901-1912.
-
John ER (1967) Mechanisms of memory in representational systems. New York: Academic Press
-
Kaczmarek LK, Adey WR (1974) Weak electric gradients change ionic and transmitter fluxes in cortex. Brain Res 66(3): 537-540.
-
Ossenkopp KP, Cain DP (1988) Inhibitory effects of acute exposure to low intensity 60Hz magnetic fields on electrically kindled seizures in rats. Brain Res 442: 255-260.
-
Morrell LK (1966) Some characteristics of stimulus- provoked alpha activity. Electroencephalogr Clin Neurophysiol 21(6): 552-561.
-
Bewernick B, Schlaepfer TE (2015) Update on Neuromodulation for Treatment-Resistant Depression. F1000Res 4: F1000 Faculty Rev-1389.
-
Morvai S, Nagy A, Kovács A, Móre CE, Berecz R, et al. (2016) Unanswered questions in the transcranial magnetic stimulation treatment of patients with depression. Ideggyogy Sz 69(1-2): 4-11.
-
Zyss T, Rachel W, Datka W, Dudek D, Zięba A, et al. (2015) Transcranial magnetic stimulation in psychiatric therapy. Przegl Lek 72(7): 371-375.
-
Sabesan P, Lankappa S, Khalifa N, Krishnan V, Gandhi R , et al. (2015) Transcranial magnetic stimulation for geriatric depression: Promises and pitfalls. World J Psychiatry 5(2):170-181.
-
Andrews JC, Stein RB, Roy FD (2015) Reduced postactivation depression of soleus H reflex and root evoked potential after transcranial magnetic stimulation. J Neurophysiol 114(1): 485-492.
-
Opie GM, Ridding MC, Semmler JG (2015) Task- related changes in intracortical inhibition assessed with paired- and triple-pulse transcranial magnetic stimulation. J Neurophysiol 113(5): 1470-1479.
-
Lissoni P, Esposti D, Esposti G, Mauri R, Resentini M, et al. (1986) A clinical study on the relationship between the pineal gland and the opioid system. J Neural Trans 65(1): 63-73.
-
Chervyakov AV, Chernyavsky AY, Sinitsyn DO, Piradov MA (2015) Possible Mechanisms Underlying the Therapeutic Effects of Transcranial Magnetic Stimulation. Front Hum Neurosci 9: 303.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury