Brain Tuberculoma Presenting as Cerebral Cystic Tumor
Etiological diagnosis of cystic tumor in adult patients can be laborious. Differential diagnosis includes a variety of primary brain tumors such as pilocytic astrocytomas and gongliogliomas, metastases or brain abscesses. We report herein an exceptional cause of cystic brain tumor in a 22-year-old Tunisian man. The patient presented with acute intracranial hypertension syndrome with a right temporal parenchymatous cystic mass on brain MRI. This mass has a nodule of 25 mm in contact of its posterior wall, taking intense and homogenous contrast after Gadolinium injection, and associated with perilesionel edema. Operative findings denoted that cystic component of the tumor was in fact the temporalhorn of the lateral ventricle that has been excluded by the nodular lesion. Pathological study of the nodule confirmed the diagnosis of brain tuberculoma. In endemic area; tuberculosis must be ruled out first in patients with braintumors since it may simulate any type of lesion.
Introduction
On brain imaging, cystic tumors in adult patients can lead to a challenging differential diagnosis. Primary brain tumors such as pilocytic astrocytomas, gongliogliomas or oligodendroglyomas, cerebral metastases and brain abscesses are the most frequent. We report here in an exceptional cause of “cystic” brain tumor.
A 22-year old Tunisian man, with no medical history has presented with headache and vomiting evolving insidiously for one month. The patient was afebrile and did not complain of any other symptom. Neurological examination did not reveal any localizing signs except funduscopic exam showing a mild bilateral papilledema.
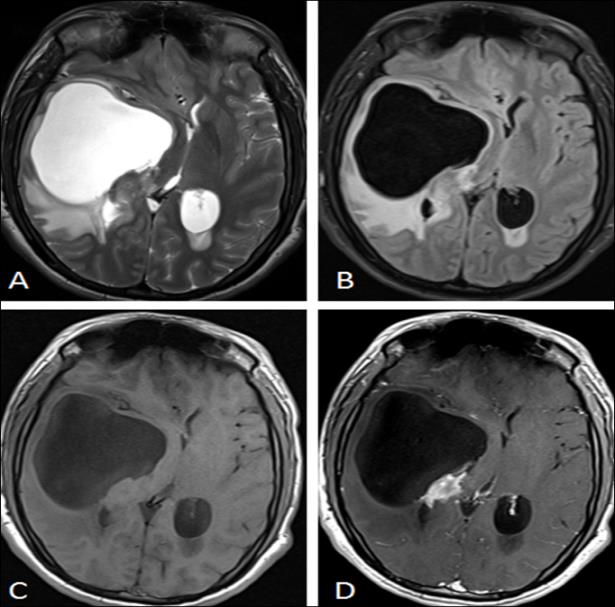
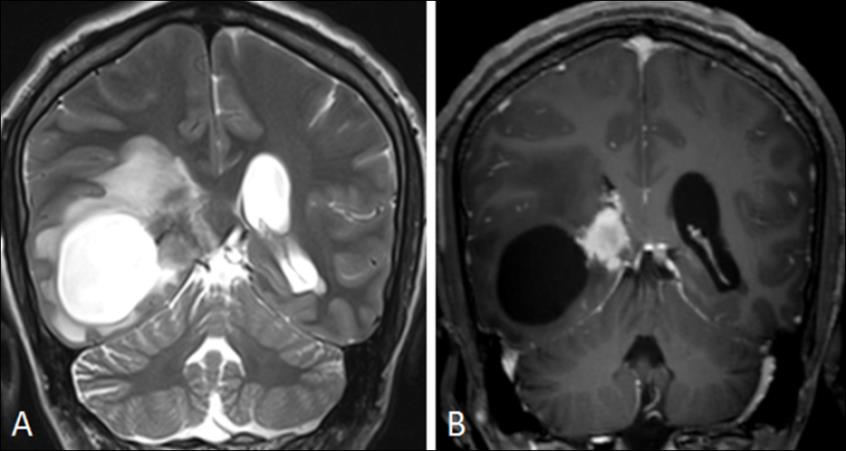
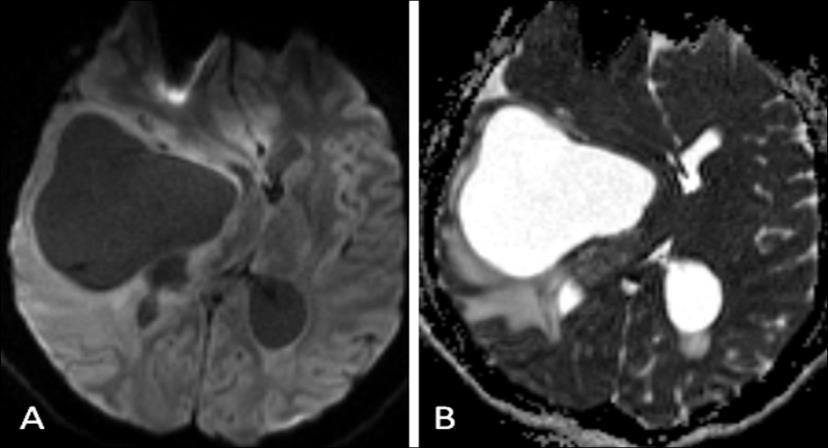
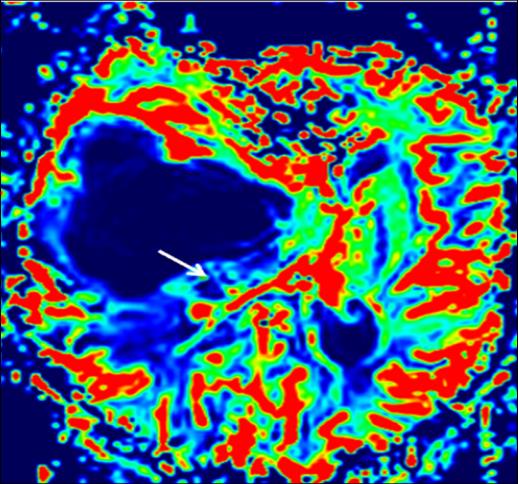
Brain MRI Figures 1-4 revealed a right temporal cystic mass, with thin walls and content identical to the signal of cerebrospinal fluid (CSF). This mass has a nodule of 25 mm in contact of its posterior wall, taking intense and homogenous contrast after Gadolinium injection, and it is associated with perilesional edema. In diffusion-weighted images, nodule has low diffusion signal with elevated Apparent Diffusion Coefficient (ADC). The cystic part of the tumor was identical to CSF on DWI. Perfusion sequence showed a decreased relative cerebral brain volume (rCBV) in both cystic and tissular parts of the tumor.
The patient was operated on for tumor removal considering he has elevated intracranial pressure and optic nerve involvement. Operative findings denoted that the cystic component of the tumor was in fact the temporal horn of the lateral ventricle which has been excluded by the nodular lesion. Pathological study of this nodular lesion revealed giant cells granuloma with focal caseous necrosis. The diagnosis of brain tuberculoma mimicking a cystic tumor was made and anti-tuberculosis chemotherapy was started. Tuberculosis is one of the most prevalent infectious diseases worldwide; near 10% of population is affected around the world [1]. Whereas, central nervous system involvement in tuberculosis remains rare (1% of all tuberculosis forms), and it is more exceptional in immunocompetent like our patient [1, 2]. The diagnosis of brain tuberculomas is still challenging despite the improvement of imaging techniques. In fact, radiological finding in brain tuberculomas are non- specific [1, 3]. Typical MRI features include target sign with peripheral ring enhancement. Nodular lesion with homogenous gadolinium enhancement is more uncommon and can be misdiagnosed with brain metastases [4]. In all cases, histopathological analysis or Koch bacillus isolating in CSF provide diagnostic confirmation [2]. Early administration of anti-tuberculosis drugs, associated in some cases to corticosteroids, can lead to complete regression and a good prognosis [2, 5]. Neurosurgical resorts can be indicated in patients with intracranial hypertension, brainstem or spinal cord compression or other serious neurological symptoms.
In conclusion, physician must remember that tuberculosis still the greatest clinical and radiological imitator. Therefore, tuberculomas should be ruled out in patients with brain tumors, especially in endemic area like Tunisia.
References
-
DeLance AR, Safaee M, Oh MC, Clark AJ, Kaur G, et al. (2013) Tuberculoma of the central nervous system. J Clin Neurosci 20(10): 1333-1341.
-
Battikh R, Yedeas M, Labidi J, Ben Abdelhafidh N, Zaouali J, et al. (2009) Tuberculomes cérébraux : à propos de six cas. Revue Neurologique 165(11): 943- 948.
-
Monteiro R, Carneiro JC, Costa C, Duarte R (2013) Cerebral tuberculomas-A clinical challenge. Respiratory Medicine Case Reports 9: 34-37.
-
Madhavan K, Widi G, Shah A, Petito C, Gallo BV, et al. (2012) Tuberculoma of the brain with unknown primary infection in an immunocompetent host. J Clinic Neurosci 19(9): 1320-1322.
-
Li H, Liu W, You C (2012) Central nervous system tuberculoma. J Clinic Neurosci 19(5): 691-695.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury