Diastematomyelia in Children in 12 Cases and Literature Review
Introduction: Diastematomyelia is a rare form of firm spina with an incidence of 2-4 per 1,000 births that requires early diagnosis and management to avoid any neurological or orthopedic worsening that may become permanent in a growing child. Patients and Method: it is a retrospective study of 12 patients treated between January 2017 and February 2020. Results: the average age was 4.5 years with extremes ranging from 06 months to 14 years. The lumbar location being the most frequent in 8 cases (66.66%). The MRI made it possible to make the diagnosis and to classify it in type 1 in 9 cases (75%) and in type 2 in 3 cases (25%) and to highlight associated lesions in 10 cases (83.33%). All of our patients were operated on, there is 1 case of motor worsening (8.3%) which was only transient, 7 patients stabilized (58.3%) and 4 patients improved (33.33%). Conclusion: the cutaneous stigmata associated with progressive congenital scoliosis in a child should prompt us to further explorations of the entire nervous axis in search of this pathology which is associated with other nerve damage which must be treated simultaneously than Diastematomyelia.
Introduction
Diastematomyelia is a rare condition of firm spina with an incidence of 2-4 per 1000 births according to Jindal [1]. It results from a disturbance of the gastrulation process, which causes the notochord to split on either side of the obstacle. This split notochord induces a double neural plate, therefore a double neural tube (diplomyelia); while the mesenchyme which organizes itself around the split notochord and neural tube tends to produce a splitting of the medullary canal (diastematomyelia). There are 2 types, type 1 or the two hemi-marrows each are in a clean bag; whereas in type 2 these are contained in a single bag. This predominates in the female sex with a sex ratio of 3F/1H. The clinical pictures are different depending on the age; thus the cutaneous stigmata predominate in newborns and infants, are grafted by orthopedic and neurological manifestations in older children. The MRI performed in all of our patients confirmed the diagnosis and should explore the entire nervous axis in order to highlight other associated lesions such as attached lower marrow, syringomyelia, thick filum. However, in the case of type 1 diastematomyelia we supplemented with the practice of a spinal scanner which allowed us to better appreciate the bone component of the spur as well as its direction, the lumbar seat of which seems to be the most frequent in our series. And according to the literature review. All our patients were operated with 90% good results, see stabilization and this was a function of the severity of the neurological signs and their duration of installation.
Patients and Methods
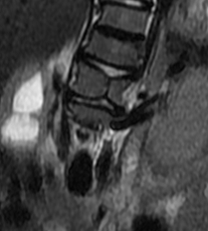
We identified 12 patients carrying this pathology during a period extending from January 2014 to September 2017 who are divided by sex into 9 female patients and 3 male patients, i.e. a ratio of 3F/1H. The age of our patients varies between 0-15 years with a peak recruitment of 5 patients between 4-6 years (41.66%) (Table 1 & Figures 1,2).
| Age | Number of cases | Sex | |
|---|---|---|---|
| Girls | Boys | ||
| 0-2 years | 1 | 1 | - |
| 2-4 years | - | - | - |
| 4-6 years | 3 | 2 | 1 |
| 6-8 years | 1 | - | 1 |
| 8-10 years | 1 | 1 | - |
Table 1: Distribution by age
Type 1 of Diastematomyelia is the most frequent, representing more than 9 cases, ie 75% of our series whose seat in the lumbar region is found in more than 8 cases (66.66%). According to PANG [2] type 1 is of the order of 60%.

- Orthopedic manifestations are the second reason in 85% of cases where kyphoscoliosis remains the main symptom
- The neurological deficits found in 50% of cases are varied, it may be atrophy involving one or both lower limbs with paraparesis.
• Trophic disorders such as plantar perforating ailments are found in 03 cases (25%).
• Sphincteric disorders are rare and are only found in 2
When recruiting our patients, the clinical manifestations that allowed the diagnosis are distributed as follows: • Skin stigmata are present in 100% of cases constituting one of the reasons for consultation.
cases (16.66%).
• Radiological investigations in type 1 Diastematomyelia have shown vertebral malformations such as:
• Cyphoscoliosis 8 cases (66.66%).
- 3 cases butterfly wing vertebrae
- A widening of the inter-pedicle distance at the level of the floor concerned by the spur 01 case
- Vertebral blocks 02 cases.

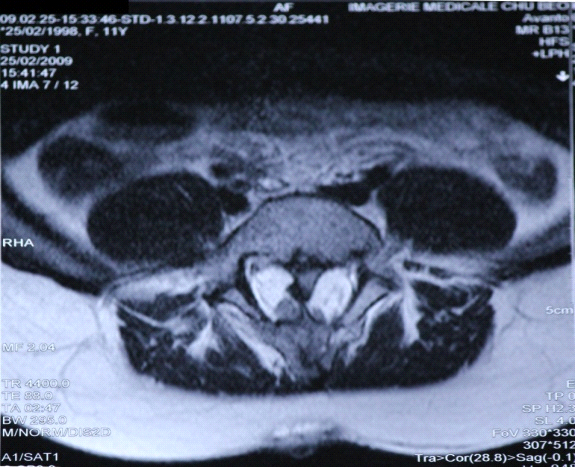
The MRI is the examination that was performed in all our patients 100%, it confirmed the diagnosis and specified the type of Diastematomyelia and to highlight associated lesions See Table 2 (Figure 3).
| Ersahin | Our Serie | |
|---|---|---|
| Thick filum | 113 cases 86.25% | 03 cases 50% |
| Myelomeningocele | 26 cas 19,84% | - |
| Meningocele missing | 23 cases | 03 cases 50%- |
| Méningocele | 19 cases | 01 case 16.66% |
| Intra dural lipoma | 12 cas | 01 case 16.66% |
| Dermal sinus | 8 cases | 01 case 16.66% |
| Epidermoid cyst | 6 cases | 01case 16.66% |
| Dermoid cyst | 5 cases | 01 case 16.66% |
| Lipomyelomeningocele | 5 cases | - |
| Tératoma | 01 case | - |
| Syringomyelia | - | 02cases 50% |
| Mac de type 1 | - | 02 cases 33.33% |
| 5th Ventricule | - | 01 case 16.66% |
Table 2: associated lesions
The treatment consists of:
- In patients who presented with type I SCM, the laminectomy or laminotomy is performed around the fixation of the rigid median septum.
- The spur is dissected extradurally between the two hemimoellae and removed either with “rodent” forceps; or by microdrill milling of the spur into the dural slot.
- After removal of the septum, the dura is opened on both sides of the dural cleft.
- The hemimoellae, containing fibrous bands or paramedian dorsal roots adhering to the dural sleeve, are sectioned, and the latter is then resected.
- Dural closure is achieved by reconstituting a single dural sheath.
- In patients with SCM type II, laminotomy is preferably performed at the caudal end of the segment concerned.
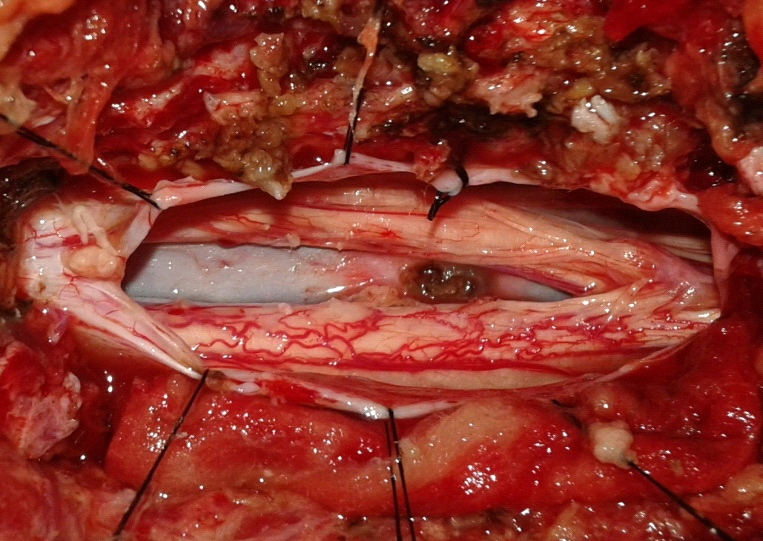
The fibrous septum is severed and any associated lesions that contribute to the attachment of the spinal cord, such as a thick filum terminale, or a dermal sinus tract, or a lipoma, are treated in one step (Figure 4).
Results
Diastematomyelia is a rare form of closed spina with an incidence of 2-4 per 1000 births [1]. Clinically apart from cutaneous stigmata; ten patients were symptomatic (83.3%) and break down as follows:
- 8 patients presented with a motor deficit associated with orthopedic manifestations
- 2 patients had a motor deficit alone
- 2 patients were asymptomatic with type 2 Diastematomyelia.
MRI revealed a bone spur in 09 cases (75%) including 07 cases in the lumbar region (77.77%) 2 in the dorsal region. Associated nerve damage is present in 10 cases (83.33%), the most frequent of which are a thick filum in 07 cases (58.33%), and a syringomyelic cavity in 05 patients (41.66%); a missed meningocele in 05 cases; dermoid and squamous cell tumors in 3 and 2 cases respectively and a myelomeningocele in 01 cases Table 2.
• Post-operative complications were observed in 3 patients (25%), they consisted of: CSF fistulas in 02 cases that did not require revision surgery. A transient paraparesis 01 case because the removal of the bone spur was laborious given its mplantation base which was wide and its close adhesion to one of the hemimoellae. Urinary retention, in 01case which required repeated probing and prolonged the length of hospitalization. These complications improved after 3 weeks in collaboration with rehabilitation treatment Table 3.
| Series | Ersahin | Our Serie |
|---|---|---|
| CSF leak | 10 cases/131 | 01 case |
| Meningitis | - | - |
| Pseudomeningocele | 5 cases | 01 case |
| Surgical wound infection | 2 cases | |
| Urinary retention or incontinence | 03 cases | 01 case |
| Motor worsening | 04 cases | 01 case |
| Neuropathic pain | 04 cases | - |
| Monoparesis | 01 case | - |
Table 3: Postoperative Complications.
Discussion
Pang, et al. [2] proposed a unified theory of embryogenesis which argues that all diastematomyelia results from a fundamental error in the formation of an accessory neurenteric channel between the yolk sac and the amnion. The sex ratio according to Pang [2, 3] is 3F/1H which seems to closely correlate with our series where the female predominance is clear. Clinically, cutaneous stigmata are present in our series in 100% of cases through hypertrichosis, at the apex of kyphosis, which appears to be pathognomonic of Diastematomyelia; while the literature review only records their presence between 40 and 60% [16].
These constitute an essential means of diagnosis in order to initiate the necessary additional investigations. The orthopedic manifestations that constitute scoliosis or kyphoscoliosis are present in 70% according to the review of the literature [10, 11, 12] and the limb shortening which constitutes the syndrome of James and lassman [9] is found in 30% cases.
The risk of neurological complications occurring with the correction of congenital scoliosis is ten times greater than with idiopathic scoliosis; This has to say that any patient who presents with congenital scoliosis must have an MRI because the detection and the early treatment of this diastematomyelia makes it possible to prevent any subsequent worsening of the scoliosis. These are very common in type 1 Diastematomyelia and absent in type 2.
Isolated sphincter disorders have been reported but rare; special attention must be given to children who have seen a regression of their sphincter cleanliness associated with a long history of constipation, hence the importance of urodynamic tests which may or may not show a neurogenic bladder [4, 5, 6].
Computed tomography and magnetic resonance are two examinations that complement each other. The first is useful for the study of bone alterations, while the second allows to appreciate and evaluate the associated lesions of which the lower marrow attached by a thick filum is the lesion most frequently encountered according to the literature review of the order of 70 to 83% [13] while syringomyelia is the second estimated between 29 to 55% [14, 15].
Conclusion
The cutaneous stigmata associated with progressive congenital scoliosis in a child should prompt us to further explorations of the entire nervous axis in search of this pathology which is associated with other nerve damage which must be treated simultaneously than Diastematomyelia.
According to MILLER [7] and Ersahin, et al. [8], the later the diagnosis, the more the risk of neurological worsening and therefore of sequelae which can be permanent and thus compromise the functional prognosis in a growing child is increased.
References
-
Jindal A, Mahapatra AK, Kamal R (1999) Spinal dysraphism. Indian J Pedia 66(5): 697-705.
-
Pang D, Dias MS, Barmada AM (1992) Split cord malformations. Part I: A unified theory of embryogenesis for double spinal cord malformations. Neurosurgery 31(3): 451-480.
-
Pang D (1992) Split cord malformations. Part II: Clinical syndrome. Neurosurgery 31(3):481-500.
-
Humphreys RP, Hendrick EB, Hoffman HJ (1982) Diastematomyelia. Clin Neurosurg 23: 436-456.
-
Goldberg C, Fenelon G, Blake NS (1984) Diastematomy- elia: a critical review of natural history and treatment. Spine 9(4): 367-372.
-
Jindal A, Mahapatra AK (2000) Split cord malforma- tion. A study of 48 cases. Indian J Pediatr 37(6): 603-607.
-
Miller A, Guille JT, Bowen JR (1984) Evaluation and treat- ment of diastematomyelia. J Bone Jt Surg Am 66:588– 601.
-
Ersahin Y, Mutluer S, Kocaman S, Demir- ats E (1998) Split spinal cord malformation in chil- dren. J Neurosurg 88(1): 57-65.
-
James CCM, Lassman LP (1958) Diastematomyelia. Arch Dis Child 33(172): 536-539.
-
Borkar SA, Mahapatra AK (2012) Split cord malformations: a two years experience at AIIMS. Asian J Neurosurg 7(2): 56-60.
-
Akay KM, Izci Y, Baysefer A, Timurkaynak E (2005) Com- posite type of split cord malformation: two different types at three different levels: case report. J Neurosurg 102(4 Sup): 436-438.
-
Birch BD, McCormick PC (1996) High cervi- cal split cord malformation and neurenteric cyst asso- ciated with congenital mirror movements: case report. Neurosurgery 38(4): 813-815.
-
Gan YC, Sgouros S, Walsh AR, Hockley AD (2007) Di- astematomyelia in children: treatment outcome and natural history of associated syringomyelia. Childs Nerv Syst 23(5): 515-519.
-
Cameron AH (1957) Arnold–Chiari and other neuroana- tomical malformations associated with spina bifida. J Pathol 73: 195-211.
-
Gupta RK, Sharma A, Jena A, Tya- gi G, Prakash B, et al. (1990) Magnetic resonance evalu- ation of spinal dysraphism in children. Childs Nerv Syst 6:161-165.
-
Yusuf E (2013) Split cord malforma- tion types I and II: a personal series of 131 pa- tients. Childs Nerv Syst 29(9): 1515-1526.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury