Effect of Intracerebroventricular Injection (ICV) of Simvastatin on Cerebellum and CA1 Region of the Hippocampus
Introduction: Simvastatin is a lipophilic statin. Lipophilic statins can cross the blood-brain barrier. The present study investigates the effect of simvastatin on cerebellum and region CA1 neurons of hippocampal in adult male rats without brain injury by the ICV method. Method: In this experimental study, 26 male Wistar rats weighing 250-300 g were randomly divided into six groups (n=6) including: control ICV (without injection), Shm (3μl ICV distilled water), simvastatin 28.5 nmol ICV, simvastatin 28.5 nmol ICV + vitamin D 5 µg/kg. Simvastatin treatment was performed for seven days. After the treatment period, Histological and biochemical studies were performed. Findings: Based on the results, the groups receiving simvastatin with a concentration 28.5 nmol did not have a significant difference in the percentage of degenerative cerebellar neurons compared to the control group (P> 0.05), but a significant percentage of degenerated cells in the neurons of the hippocampal region CA1 compared to the control group (P <0.05). Was observed with the control group. No significant effect was observed on the level of MDA and FRAP in any of the groups compared to the control group (P> 0.05). Conclusion: The present study results showed a negative effect of simvastatin on hippocampal pyramidal neurons, but this negative effect was not observed on Russian Purkinje cerebellar neurons.
Introduction
The first Statins were discovered in 1972 by Dr. Akira Ando’s research team [1]. Inhibitors of hydroxymethylglutaryl coenzyme A (HMG-CoA) reductase, statins are approved by the US Food and Drug Administration (FDA) as cholesterol- lowering drugs. These drugs target the liver and inhibit cholesterol biosynthesis, which results in decreased intracellular cholesterol levels in the liver and subsequently regulates the number of LDL-C receptors on the cell surface [2]. Statins are generally known for protecting and treating cardiovascular disease [3], reducing LDL-C and TG levels, and increasing HDL-C [4, 5]. Simvastatin is a member of the lipophilic family of Statins [6]. Research shows that simvastatin is a lipophilic statin capable of crossing the blood-brain barrier [7, 8], so it affects the brain.
Oxidative stress stems from the imbalance relation of oxidants (free radicals) and antioxidants, which results in the accumulation of free radicals in the cells, which subsequently interact with the biological molecules. It mainly arises from an increase in free radicals, an imbalance between the production and elimination of active species in the body, and a decrease in the potency of the antioxidant defense system [9, 10]. Several cellular processes, including cell metabolism, cell signaling pathways, gene expression, cell proliferation, and programmed cell death, are affected by oxidative stress [11]. The antioxidant defense system is divided into two categories: the non-enzymatic antioxidant defense consisting of small molecules such as vitamin E, ascorbate, and glutathione. The other is the enzymatic antioxidant defense of the cell includes superoxide dismutase catalase, glutathione peroxidase and glutathione peroxidase. Decomposition of volatile peroxidases derived from unsaturated fatty acids leads to the formation of malondialdehyde [12].
In addition to their effects on plasma lipids, statins can have important anti-inflammatory effects. Since inflammation is directly related to the production of reactive oxygen species, the molecular basis of the observed anti- inflammatory effects of statins may be related to the ability to They will be in the cessation of production or activity of ROS. The antioxidant effects of statins are likely to contribute to their clinical effectiveness in treating cardiovascular disease and other chronic diseases associated with increased oxidative stress in humans [13]. In addition to their fat- reducing properties, statins have separate pleiotropic effects, including inhibition of oxidative stress [14]. Statins have rapid anti-inflammatory and antioxidant effects [15].
The present study evaluated the direct effect of simvastatin on neurons in region CA1 of the hippocampus and cerebellar neurons.
Materials and Methods
Twenty-six male Westar rats weighing 250-300g were purchased from the animal house of Urmia University. All procedures were followed according to the National Institute of Health guide for the care and use of Laboratory Animals (NIH Publications No. 8023, revised 1978) and local guidelines for compassionate use of animals in research; Rats were kept in cages with open access to standard tap water and compact chow. The animals were held in the same laboratory conditions (18°C to 23°C room temperature and controlled humidity) with alternating 12-h light and dark cycles. The Ethics Committee has approved the proposal of this study of Urmia University (Ethics Code: IR-UU-AEC-3/1033 / DA).
Animal Grouping
- Healthy control group who received normal water were not injected (C).
- Sham group received 3 ul of distilled water as ICV (shm)
- Simvastatin group with a dose of 28.5 nmol received a simvastatin by ICV [16] (sim).
- Simvastatin group dose of 28.5 nmol with vitamin D supplement 5 µg/kg (200 IU) [17] (sim + vD).
The drugs were administered once daily for seven days. The drug simvastatin used in the present study was produced by Timova Pharmaceutical Company (Denmark).
Stereotaxic Surgery and Cannulation for Intraventricular Brain Group
A cannula was implanted in the third cerebral ventricle of the rats a week before the onset of behavioral tests. Before surgery, animals were anesthetized by intraperitoneal injection of ketamine and xylazine at doses of 10 mg/kg and 10 mg/kg, respectively [18] After shaving head and disinfecting hair with 10% betadine and 70% alcohol, they were placed in stereotaxic apparatus, then using third ventricular coordinate axes (AP = -4.2 mm, L = 0mm, DV = -4.2), a 5mm long cannula (needle head 23) was placed as a guiding cannula in the third ventricle of their brain. The coordinate axes used in stereotaxis to access the brain’s third ventricle were selected from the brain atlas [19] to fix the cannula on the animal skull using two eyeglass screws as a base dental cement (a mixture of self-curing acrylic and monomer). A piece of thin copper wire was inserted into the cannula to prevent CSF or blood flow through the guiding cannula.
After the end of the course of drug use, biochemical and microscopic studies were performed.
Histological Studies
The brains of mice were transferred to 10% formalin for fixation and then subjected to dehydration, clarification, paraffin, and molding; then, six micron-thick sections were prepared by microtome. After staining with hematoxylin and eosin, they were examined with a light microscope. The pyramidal neurons of region CA1 of the hippocampus and Purkinje neurons of the cerebellum were explicitly studied. Degeneration of neurons (degeneration: abnormal changes in cell appearance, including cell shrinkage, membrane uniformity, and cytoplasm density) were examined by light microscopy [20].
Sampling
After completing the course of medication (Seven days), the rats were euthanized with ketamine (75.00 mg kg-1; Alfasan, Woerden, The Netherlands) and xylazine (10.00 mg kg-1; Alfasan, Woerden, The Netherlands), both intraperitoneally (IP). Then blood samples were taken from the heart of the animals. After one hour, all blood samples were centrifuged at 1500 rpm for 10 minutes to isolate their serum. The obtained serum was carefully separated by a sampler and stored in Ependrov microtubes in a freezer at -80°C for serological assessments. The brain tissue was carefully removed and transferred to a −80°C freezer for evaluation of oxidative stress markers.
Biochemical Assay
To lipid peroxidation measurement, the malondialdehyde (MDA) concentrations of brain tissue were assessed using the reaction of thiobarbituric acid as previously described [21]. The amount of total antioxidant capacity (TAOC) of brain tissue was evaluated using the ferric reducing antioxidant power (FRAP) test [22].
Statistical Analysis
Data were analyzed by one-way ANOVA using SPSS 19 software and Tukey tests, and the results were presented as mean ± standard deviation error. P <0.05 was considered as the level of significance.
Serological Outcome
Results of Examination of Neurons in the Ca1 Region of the Hippocampus
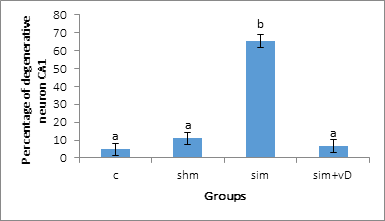
Statistical results of neurons in the cA1 region of the hippocampus (pyramidal neurons) showed that the group receiving simvastatin at a dose of 28.5 nmol (sim) had a significant increase (P <0.05) in the percentage of degenerative cells in this region compared to the control group, but other groups did not show a significant difference compared to the control group (P> 0.05) (Figure 1).
Results of Examination of Cerebellar Neurons (Purkinje Neurons)
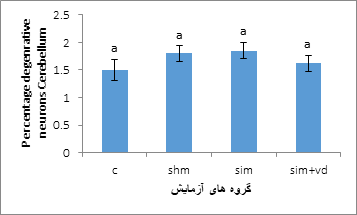
Statistical results of cerebellar neurons (Purkinje
neurons) showed that none of the groups had a significant difference in the percentage of degenerative cells in this area compared to the control group (P> 0.05) (Figure 2).
MDA Biochemical Test Results
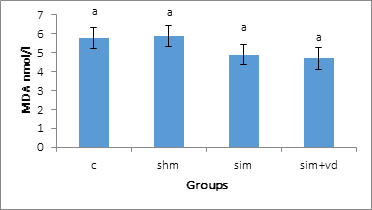
The statistical results of MDA biochemistry test in stereotaxic surgery group showed that none of the groups had a significant difference in MDA compared to the control group (P> 0.05), (Figure 3).
Results of FRAP Biochemical Test
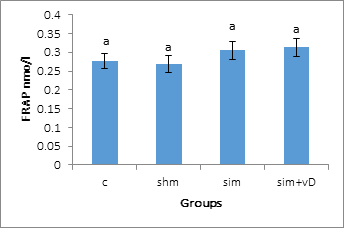
The statistical results of the FRAP biochemistry test showed that none of the tested groups were significantly different from the control group (P> 0.05) (Figure 4).
Discussion and Conclusion
Cholesterol is an essential sterol synthesized by most human cells, majorly in the liver. It is a necessary constituent of cell membranes; it acts as a precursor for synthesizing steroid hormones, vitamin D, and bile acids. Cholesterol is transported in plasma primarily in low- density lipoproteins (LDL) [23]. Statins have an impact on serum cholesterol concentration. Treatments with statins reduce LDL-C levels [24]. Cholesterol does not cross the blood-brain barrier [25]. Brain cholesterol is produced by its production in this organ. Any interference with cholesterol concentration in the brain can also affect the cell wall, resulting in lipophilic statins such as simvastatin. It can cross the blood-brain barrier and affect cholesterol concentration in the brain. In one study, when lovastatin or simvastatin was temporarily injected into mice, simvastatin was found in higher concentrations in the CNS, causing changes in the expression of more genes and significantly lowering brain cholesterol levels than lovastatin [26]. The study results of Wonders of Pamelia and Manik Panilia et al., Showed that cholesterol levels in the cerebral cortex are slightly reduced [27].
Some studies of the adverse effects of statins include: cessation of DNA synthesis and proliferation [28], cell death in primary neuronal cell culture [29, 30] death of neuroblasts [31], loss of synapses [32], and adverse effects on cognitive function has been reported in clinical studies [33]. The results showed that the death of neurons and oligodendrocytes was at a concentration of 0.1 μmol of simvastatin, which was in the same range for the inhibition of cholesterol by simvastatin in liver tissue [34, 35].
The results of some studies suggest that simvastatin is effective in inhibiting hippocampal cell apoptosis and inflammation in mice with Alzheimer’s disease. That simvastatin has protective effects on the nervous system [36, 37], and that treatment with simvastatin has potential inhibitory effects on apoptosis of hippocampal nerves, thus helping to improve memory [38, 39]. Some studies have shown that treatment with simvastatin significantly reduces nerve damage. And reduction of apoptosis in the hippocampus [40].
Measures that directly study cerebral structure, cerebral blood flow, cholesterol circulation, and neuronal activity can be used to understand how statins affect the CNS. Still, there are few studies in this area. And their results are different. Decreased hippocampal volume and memory impairment have been studied in some age-related studies; however, there are few studies on the effect of statins on the hippocampus. There are many differences in their results [41, 42]. Also, other research results indicate the death of cerebellar granular neurons in cell culture medium treated with simvastatin 0.1 μmol [29]. In this regard, the results of Zongmin and Steven’s research aimed at investigating the effect of simvastatin on the progression of myelination in a mouse cerebellum cell culture model, indicating inhibition of cholesterol synthesis by simvastatin during the progression of primary cells to neurons and oligodendrocytic and showed harmful effects of simvastatin on myelination [43].
The results of the present study, despite the difference in the type of use of simvastatin (in this study as intraventricular injection) and the difference in the dose used (in this study, 28.5 nmol dose of simvastatin) confirm the above research on the negative effect of simvastatin. The results of the study of hippocampal tissue in the present study indicate a significant increase in the percentage of degenerative pyramidal neurons in the cA1 region compared to the control group (Figure 1). The important point in this study is that in the group receiving vitamin D supplementation (Sim + vD), there was a significant decrease in the percentage of degenerated neurons compared to the group receiving simvastatin (sim), which can be the important point. It is important to take vitamin D supplements with simvastatin, which could lead to more research on the importance of taking statins more efficiently. If there is a lot of research on vitamin D supplementation with statins, it is associated with a decrease in vitamin D and the development of statin- induced muscle myopathy.
The study results of cerebellar tissue (Purkinje neurons) in the present study did not show any significant adverse effect of simvastatin in the groups receiving this drug compared to the control group (Figure 2). The present study is one of the few studies on the effect of statins on the cerebellum and the clinical manifestations of statin drugs on central nervous system cells, including the cerebellum. The present study was performed without complication in the cerebellum on healthy mice. The direct effect of simvastatin on the cerebellum was performed as part of the central nervous system results of the present study show that simvastatin is used in the form of i.c.v injection in the third ventricle of the brain, there is no negative effect on the appearance of cerebellar cells. It should be noted that the presence of vitamin D supplementation did not show any significant effect on the histomorphometry of cerebellar cells compared to the control group. Perhaps the main reason for the discrepancy between the results and some of the above studies is the difference in the type of statin used and the difference in the dose used and also the difference during the treatment period [16], Because of the importance of these drugs, more studies are needed in the future.
The question may arise as to why the drug simvastatin in the present study caused significant degeneration of pyramidal neurons in region CA1 of the hippocampus. Still, this tiger effect was not observed in Purkinje’s neurons? The answer to this question is in Segatto M. et al.’s research results. They reported that statins had the most significant effect on the hippocampus and cortex and had a minor impact on the cerebellum and brainstem. The results of Segatto M, et al. showed that differences in HMGR and LDLr regulation are present in brain areas. They also reported that these variations seem to be related to cholesterol turnover, regional myelin content, and synaptic plastic modulation. These data emphasize marked functional differences in HMGR and LDLr regulation in brain regions [44].
Simvastatin-induced toxicity has been reported on different cell types [45]. Statins have a significant effect on the hippocampus [44], and simvastatin has been reported to impair myelin repair in myelinated mice [46]. Simvastatin treatment may interfere with myelin repair by inhibiting lipid-associated signaling and the cholesterol- dependent process [47]. Other studies have also shown that simvastatin blocks the differentiation of progenitor cells into mature molecular cells in the CNC (Central nervous system) [48, 49]. Kaminsky et al.’s research showed that treatment of astrocytes with simvastatin induced apoptosis in a dose- and time-dependent manner [45]. Statins lower cholesterol [50], That cholesterol is an integral part of animal cell membranes; therefore, any drug that affects cholesterol concentration can affect animal cell membrane cholesterol since statins are cholesterol-lowering drugs. They can affect the cell membrane, cholesterol does not cross the blood-brain barrier, and brain cholesterol is produced by its production in this organ [25]. Any interference with cholesterol concentration in the brain can affect the wall. The effect of statins on cholesterol increase the permeability of cell membranes due to disturbing the cholesterol balance of the cell wall can enter the cell during tissue passage and affect the results of studies.
Increased antioxidant enzyme activity has been reported during treatment with atorvastatin and simvastatin [51]. MDA is a by-product of lipid peroxidation and is widely used as a marker of oxidative stress [52] oxygen radicals produce membrane peroxidation and malondialdehyde formation, which is detrimental to cellular function. Oxidation can increase membrane permeability while MDA can inactivate membrane channels by establishing interdisciplinary and intermolecular relationships [14]. Study results show a significant reduction in MDA with atorvastatin 20 mg Shows [53, 54]. Statins have been shown to reduce MDA in patients with type 2 diabetes and fatty liver [53, 55, 56]. Significant reductions in serum MDA as a marker of lipid peroxidation have been reported in patients treated with high-dose simvastatin [57].
FRAP concentration considers the cumulative action of all antioxidants present in plasma and body fluids and provides an integrated parameter instead of the simple sum of measurable antioxidants [58]. Simvastatin treatment does not affect the FRAP [59, 60], but the results of another study indicate that serum FRAP levels increase in patients treated with long-term atorvastatin [61]. Simvastatin has been reported to increase catalase levels and inhibit lipid peroxidation [62]. The results of a study by Joon John Moon et al. The antioxidant effects of statins indicated that short-term use of high-dose statins had significant antioxidant effects [63]. It also affects cholesterol levels, and its antioxidant effect is independent of cholesterol lowering effects [64]. Statins increase nitric oxide production, leading to increased catalase, 4BH, and inhibition of LDL oxidation. and restore vitamins C, E, and endogenous antioxidants such as ubiquinone and glutamine [65].
In general, citing previous research on the antioxidant effects of statins, it has been argued that statins decrease malondialdehyde levels and increase the FRAP test. The results of the present study showed that simvastatin in the dose used and the duration of use showed a slight effect on reducing MDA (Figure 3) and a small effect on increasing FRAP (Figure 4), and there was a no significant difference in either of the two biochemical factors. It should be noted that the presence of vitamin D did not show any significant effect in biochemical tests compared to the control group. The question arises: Why, despite the negative effect of simvastatin on pyramidal neurons in the CA1 region, has no negative effect occurred on biochemical tests? It should be noted that the effects of statins on serum profiles and other tissue effects are different from the antioxidant effects of statins [14, 64].
Also, in the present study, an adverse effect was observed in the CA1 region, but no significant adverse effect was observed in the cerebellum (Purkinje neurons). It should be noted that the tissue section studied for biochemical tests involves large parts of the brain and is not specific to the CA1 region. On the other hand, brain cholesterol is caused by its production in this organ [25]. Any interference in cholesterol concentration in the brain can also affect the cell wall. Thus the effect of statins on cholesterol and increased permeability Cell membranes can enter the cell due to disturbance of cell wall cholesterol balance during tissue passage and affect the results of studies (in the present study, this effect was observed in the CA1 region the hippocampus). As a result of the effect of statins on cholesterol and increasing the permeability of cell membranes as a result of disturbing the cholesterol balance of the cell wall, dye can enter the cell during tissue passage and affect the results of studies (in the present study, this effect on CA1 region of the hippocampus was observed). Although this drug was observed to harm CA1 cells, this does not mean that it damaged other parts of the brain (no significant adverse effect was observed on cerebellar neurons in the present study) or a negative antioxidant effect. It should be noted that the type of statin use and the dose used in the present study are different from the above research on the antioxidant effects of statins and that in the present study the direct effect of simvastatin on the brains of healthy mice was investigated [16], It should be noted that the present study was performed on laboratory animals and this does not mean that simvastatin has the same effects on the human brain, so the results of the present study need further studies and experiments in the future.
Conclusion
Simvastatin degenerated neurons in the hippocampal region CA1 but had no adverse effect on cerebellar Purkinje neurons.
References
-
Shinohara M, Sato N, Shimamura M, Kurinami H, Hamasaki T, et al. (2014) Possible modification of Alzheimer’s disease by statins in midlife: interactions with genetic and non-genetic risk factors. Front Aging Neurosci 6: 71.
-
Brown MS, Goldstein JL (1999) A proteolytic pathway that controls the cholesterol content of membranes, cells, and blood. Proc Natl Acad Sci 96(20): 11041-11048.
-
Taylor F, Huffman MD, Macedo AF, Moore THM, Burke M, et al. (2013) Statins for the primary prevention of cardiovascular disease. Cochrane Database Syst Rev 2013(1): CD004816.
-
Karalis DG (2009) Intensive lowering of low-density lipoprotein cholesterol levels for primary prevention of coronary artery disease. Mayo Clin Proc 84(4): 345-352.
-
Liao JK, Laufs U (2005) Pleiotropic effects of statins. Annu Rev Pharmacol Toxicol 45: 89-118.
-
Farooqui AA, Ong WY, Horrocks LA, Chen P, Farooqui T (2007) Comparison of biochemical effects of statins and fish oil in brain: the battle of the titans. Brain Research Reviews 56(2): 443-471.
-
Botti RE, Pan HY, Triscari J, Zayat J (1991) Concentrations of pravastatin and lovastatin in cerebrospinal fluid in healthy subjects. Clin Neuropharmacol 14(3): 256-261.
-
Saheki A, Terasaki T, Tsuji A (1994) In vivo and in vitro blood–brain barrier transport of 3-hydroxy-3- methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors. Pharm Res 11(2): 305-311.
-
Dayem AA, Choi HY, Kim JH, Cho SG (2010) Role of oxidative stress in stem, cancer, and cancer stem cells. Cancers (Basel) 2(2): 859-884.
-
Tandon VR, Sharma S, Mahajan A, Bardi (2005) Oxidative stress: a novel strategy in cancer treatment. JK Science 7(1): 1-3.
-
Poli G, Leonarduzzi G, Biasi F, Chiarpotto E (2004) Oxidative stress and cell signalling. Curr Med Chem 11(9): 1163-1182.
-
Davignon J, Jacob RF, Mason RP (2004) The antioxidant effects of statins. Coron Artery Dis 15(5): 251-258.
-
Stoll LL, McCormick ML, Denning GM, Weintraub NL (2004) Antioxidant effects of statins. Drugs Today (Barc) 40(12): 975-990.
-
Harrison D, Griendling KK, Landmesser U, Hornig B, Drexler H (2003) Role of oxidative stress in atherosclerosis. Am J Cardiol 91(3A): 7A-11A.
-
Gomes ACP, Reilly S, Brandes RP, Casadei B (2014) Targeting inflammation and oxidative stress in atrial fibrillation: role of 3-hydroxy-3-methylglutaryl- coenzyme a reductase inhibition with statins. Antioxid Redox Signal 20(8): 1268-1285.
-
Cheng WH, Ho WY, Chang CF, Lu PJ, Cheng PW, et al. (2013) Simvastatin induces a central hypotensive effect via Ras‐mediated signalling to cause eNOS up‐regulation. Br J Pharmacol 170(4): 847-858.
-
Hughes BD, Harris SS, Krall EA, Dallal GE (1997) Effect of calcium and vitamin D supplementation on bone density in men and women 65 years of age or older. N Engl J Med 337(10): 670-676.
-
Moosavi M, Naghdi N, Maghsoudi N, Asi SZ (2006) The effect of intrahippocampal insulin microinjection on spatial learning and memory. Hormones and Behavior 50(5): 748-752.
-
Paxinos G, Watson C (2005) The rat brain in stereotaxic coordinates. Academic Press, San Diego, London, UK.
-
Azad N, Rasoolijazi H, Joghataie MT, Soleimani S (2011) Neuroprotective effects of carnosic acid in an experimental model of Alzheimer’s disease in rats. Cell J 13(1): 39-44.
-
Sadeghi A, Ghahari L, Yousefpour M (2019) Vitamin E Supplementation Reduces Oxidative Stress in the Male Wistar Rats’ Brain Against Polyvinyl Chloride Products. Annals of Military and Health Sciences Research 17(2): e92768.
-
Thaipong K, Boonprakob U, Crosby K, Zevallos LC, Byrne DH (2006) Comparison of ABTS, DPPH, FRAP, and ORAC assays for estimating antioxidant activity from guava fruit extracts. Journal of food composition and analysis 19(6-7): 669-675.
-
Narwal V, Deswal R, Batrac B, Kalra V, Hood R, et al. (2019) Cholesterol biosensors: A review. Steroids 143: 6-17.
-
Pignone M, Phillips C, Mulrow C (2000) Use of lipid lowering drugs for primary prevention of coronary heart disease: meta-analysis of randomised trials. BMJ 321(7267): 983.
-
Schreurs BG (2010) The effects of cholesterol on learning and memory. Neuroscience & Biobehavioral Reviews 34(8): 1366-1379.
-
Johnson-Anuna LN, Eckert GP, Keller JH, Igbavboa U, Franke C, et al. (2005) Chronic administration of statins alters multiple gene expression patterns in mouse cerebral cortex. Journal of Pharmacology and Experimental Therapeutics 312(2): 786-793.
-
Paintlia AS, Paintlia MK, Khan M, Vollmer T, Singh AK, et al. (2005) HMG-CoA reductase inhibitor augments survival and differentiation of oligodendrocyte progenitors in animal model of multiple sclerosis. The FASEB journal 19(11): 1407-1421.
-
Langan TJ, Volpe JJ (1986) Obligatory relationship between the sterol biosynthetic pathway and DNA synthesis and cellular proliferation in glial primary cultures. Journal of neurochemistry 46(4): 1283-1291.
-
März P, Otten U, Miserez AR (2007) Statins induce differentiation and cell death in neurons and astroglia. Glia 55(1): 1-12.
-
Michikawa M, Yanagisawa K (1999) Inhibition of cholesterol production but not of nonsterol isoprenoid products induces neuronal cell death. Journal of neurochemistry 72(6): 2278-2285.
-
Garcı́a-Román N, Alvarez AM, Toro MJ, Montes A, Lorenzo MJ (2001) Lovastatin induces apoptosis of spontaneously immortalized rat brain neuroblasts: involvement of nonsterol isoprenoid biosynthesis inhibition. Molecular and Cellular Neuroscience 17(2): 329-341.
-
Mauch DH, Nägler K, Schumacher S, Göritz C, Müller EC, et al. (2001) CNS synaptogenesis promoted by glia- derived cholesterol. Science 294(5545): 1354-1357.
-
Padala KP, Padala PR, Potter JF (2006) Simvastatin- induced decline in cognition. Annals of Pharmacotherapy 40(10): 1880-1883.
-
Bergstrom JD, Bostedor RG, Rew DJ, Geissler WM, Wright SD, et al. (1998) Hepatic responses to inhibition of 3-hydroxy-3-methylglutaryl-CoA reductase: a comparison of atorvastatin and simvastatin. Biochimica et Biophysica Acta (BBA)-Lipids and Lipid Metabolism 1389(3): 213-221.
-
Mosley ST, Kalinowski SS, Schafer BL, Tanaka RD (1989) Tissue-selective acute effects of inhibitors of 3-hydroxy- 3-methylglutaryl coenzyme A reductase on cholesterol biosynthesis in lens. Journal of lipid research 30(9): 1411-1420.
-
Rossoni LV, Wareing M, Wenceslau CF, Al-Abri M, Cobb C, et al. (2011) Acute simvastatin increases endothelial nitric oxide synthase phosphorylation via AMP-activated protein kinase and reduces contractility of isolated rat mesenteric resistance arteries. Clinical Science 121(10): 449-458.
-
Endres M, Laufs U, Huang Z, Nakamura T, Huang P, et al. (1998) Stroke protection by 3-hydroxy-3-methylglutaryl (HMG)-CoA reductase inhibitors mediated by endothelial nitric oxide synthase. Proceedings of the National Academy of Sciences 95(15): 8880-8885.
-
Ramos MC, Sierra S, Ramirez C, Velasco J, Burgos JS (2012) Simvastatin modulates the Alzheimer’s disease- related gene seladin-1. Journal of Alzheimer’s Disease 28(2): 297-301.
-
Hu X, i Song C, Fang M, Li C (2018) Simvastatin inhibits the apoptosis of hippocampal cells in a mouse model of Alzheimer’s disease. Experimental and therapeutic medicine 15(2): 1795-1802.
-
Sun J, Xie C, Liu W, Lu D, Qiao W, et al. (2012) The effects of simvastatin on hippocampal caspase-3 and Bcl-2 expression following kainate-induced seizures in rats. International Journal of molecular medicine 30(4): 739- 746.
-
Doraiswamy PM, Steffens DC, McQuoid DR (2004) Statin use and hippocampal volumes in elderly subjects at risk for Alzheimer’s disease: a pilot observational study. Am J Alzheimers Dis Other Demen 19(5): 275-278.
-
Sparks DL, Lemieux SK, Haut MW, Baxter LC, Johnson SC, et al. (2008) Hippocampal volume change in the Alzheimer disease Cholesterol-Lowering Treatment trial. Cleve Clin J Med 75(2): S87-93.
-
Xiang Z, Reeves SA (2009) Simvastatin induces cell death in a mouse cerebellar slice culture (CSC) model of developmental myelination. Exp Neurol 215(1): 41-47.
-
Segatto M, Trapani L, Lecis C, Pallottini V (2012) Regulation of cholesterol biosynthetic pathway in different regions of the rat central nervous system. Acta Physiol (Oxf) 206(1): 62-71.
-
Kaminsky YG, Kosenko EA (2010) Molecular mechanisms of toxicity of simvastatin, widely used cholesterol- lowering drug. A review. Cent Eur J med 5(3): 269-279.
-
Miron VE, Zehntner SP, Kuhlmann T, Ludwin SK, Owens T, et al. (2009) Statin therapy inhibits remyelination in the central nervous system. Am J Pathol 174(5): 1880- 1890.
-
Decker L, ffrench-Constant C (2004) Lipid rafts and integrin activation regulate oligodendrocyte survival. J Neurosci 24(15): 3816-3825.
-
Suzumura K, Yasuhara M, Tanaka K, Suzuki T (1999) Protective effect of fluvastatin sodium (XU-62-320), a 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitor, on oxidative modification of human low-density lipoprotein in vitro. Biochem Pharmacol 57(6): 697-703.
-
Yamamoto A, Hoshi K, Ichihara K (1998) Fluvastatin, an inhibitor of 3-hydroxy-3-methylglutaryl-CoA reductase, scavenges free radicals and inhibits lipid peroxidation in rat liver microsomes. Eur J Pharmacol 361(1): 143-149.
-
Athyros VG, Kakafika AI, Tziomalos K, Karagiannis A, Mikhailidis DP, et al. (2009) Pleiotropic effects of statins- clinical evidence. Curr Pharm Des 15(5): 479-489.
-
Broncel M, Koter-Michalak M, Chojnowska-Jezierska J (2006) The effect of statins on lipids peroxidation and activities of antioxidants enzymes in patients with dyslipidemia. Przegl Lek 63(9): 738-742.
-
Esterbauer H, Schaur RJ, Zollner H (1991) Chemistry and biochemistry of 4-hydroxynonenal, malonaldehyde and related aldehydes. Free Radic Biol Med 11(1): 81-128.
-
Kaya C, Pabuccu R, Cengiz SD, Dünder I (2010) Comparison of the effects of atorvastatin and simvastatin in women with polycystic ovary syndrome: A prospective, randomized study. Exp Clin Endocrinol Diabetes 118(3): 161-166.
-
Sathyapalan T, Shepherd J, Coady AM, Kilpatrick ES, Atkin SL, et al. (2012) Atorvastatin reduces malondialdehyde concentrations in patients with polycystic ovary syndrome. J Clin Endocrinol Metab 97(11): 3951-3955.
-
Li J, Sun YM, Wang LF, Li ZQ, Pan W, et al. (2010) Comparison of effects of simvastatin versus atorvastatin on oxidative stress in patients with coronary heart disease. Clin Cardiol 33(4): 222-227.
-
Samy W, Hassanian MA (2011) Paraoxonase-1 activity, malondialdehyde and glutathione peroxidase in non- alcoholic fatty liver disease and the effect of atorvastatin. Arab J Gastroenterol 12(2): 80-85.
-
Tavridou A, Efthimiadis A, Efthimiadis I, Paschalidou H (2006) Antioxidant effects of simvastatin in primary and secondary prevention of coronary heart disease. Eur J Clin Pharmacol 62(6): 485-489.
-
Majsterek I, Malinowska K, Stanczyk M, Kowalski M, Blaszczyk J, et al. (2011) Evaluation of oxidative stress markers in pathogenesis of primary open-angle glaucoma. Experimental and molecular pathology 90(2): 231-237.
-
Shin MJ, Chung N, Lee JH, Jang Y, Park E, et al. (2007) Effects of simvastatin on plasma antioxidant status and vitamins in hypercholesterolemic patients. Int J Cardiol 118(2): 173-177.
-
Strzyżewski KW, Pioruńska-Stolzmann M, Majewski W, Kasprzak M, Strzyżewski W, et al. (2013) Effect of surgical treatment on lipid peroxidation parameters and antioxidant status in the serum of patients with peripheral arterial disease. Dis Markers 35(6): 647-652.
-
Shahsavari G, Raoufi A, Toolabi A, Hosseninejadmir N, Ahmadvand H, et al. (2017) The effect of atorvastatin treatment duration on oxidative stress markers and lipid profile in patients with coronary artery diseases: A case series study. ARYA Atheroscler 13(6): 282-287.
-
Piechota-Polanczyk A, Goraca A, Demyanets S, Mittlboeck M, Domenig C, et al. (2012) Simvastatin decreases free radicals formation in the human abdominal aortic aneurysm wall via NF-κB. Eur J Vasc Endovasc Surg 44(2): 133-137.
-
Moon GJ, Kim SJ, Cho YH, Ryoo S, Bang OY, et al. (2014) Antioxidant effects of statins in patients with atherosclerotic cerebrovascular disease. J Clin Neurol 10(2): 140-147.
-
Carneado J, Alvarez de Sotomayor M, Perez-Guerrero C, Jimenez L, Herrera MD, et al. (2002) Simvastatin improves endothelial function in spontaneously hypertensive rats through a superoxide dismutase mediated antioxidant effect. J Hypertens 20(3): 429-437.
-
Tousoulis D, Antoniades C, Vassiliadou C, Toutouza M, Pitsavos C, et al. (2005) Effects of combined administration of low dose atorvastatin and vitamin E on inflammatory markers and endothelial function in patients with heart failure. Eur J Heart Fail 7(7): 1126- 1132.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury