Giant Cell Arteritis - A Disease not to be Missed in Acute Ischemic Stroke
Giant cell arteritis is described classically as a medium and large vessel inflammatory disease. It generally affects the external carotid vascular system and causes its typical symptoms. However, relatively uncommon is its involvement of internal carotid artery to cause visual disturbances and ischemic strokes. Typically, ultrasonography of the superficial temporal artery shows classical feature of the disease i.e., halo sign with a high sensitivity. Biopsy of the affected vessel, even though less sensitive, is diagnostic. We are describing such a case of giant cell arteritis involving both external and internal carotid vascular system which is negative on biopsy and did not show typical ultrasonographic features but diagnosed based on clinical criteria. Additionally the patient also had a severe atherosclerotic carotid vascular disease. Both of which may be associated with ischemic stroke.
Introduction
Stroke can be a devastating disease depending on its severity. It is one of the leading causes of disability and death world-wide. In elderly population, ischemic stroke is commonly due to atherosclerotic vascular disease. Generally the ischemic stroke is painless. Common causes of painful ischemic strokes are vascular dissection and vasculitis. Moreover, cerebral edema following an ischemic stroke can cause headache due to increased intracranial pressure, particularly in the cerebellar strokes. Headache in such a scenario is generally occipital or holocranial. We are reporting a case of new onset right hemicranial pain and right cerebral hemispheric acute ischemic stroke. Etiology presumably being both, atherosclerotic carotid vascular disease and giant cell arteritis which was diagnosed based only on clinical grounds as ultrasonography of temporal artery and biopsy were negative. Cerebral vascular imaging showed diffuse narrowing of right carotid vascular system presumably due to arteritis and a severe focal narrowing at the proximal internal carotid artery due to mixed atheroscletotic plaque.
Case Report
A 61 year old lady presented to the neurology OPD with the complaint of right sided headache of two weeks duration. She had tried several over the counter medications for the pain but had no sustained benefit. She visited our neurology OPD in the next couple of days with persistent pain. Pain was dull aching of moderate intensity, located in the right side of the head and corresponding region of the ear and jaw. Occasionally there were brief episodes of severe stabbing and pricking type of pain that lasted for a few minutes. The pain was continuous and there was no diurnal or positional variation. There was no aggravation of pain on eye or jaw movements. Along with the pain she also complained of occasional blurring of right eye vision that overlapped with the stabbing episodes of headache. There was no associated watering or redness in the right eye, nor there was any nasal stuffiness. She also complained of slight numbness in her left lower limb for the last couple of days but did not report any weakness.
Her past history was significant for uncontrolled diabetes with moderate to severe non-proliferative diabetic retinopathy with maculopathy. She also had a history of poorly controlled hypertension. She was treated for carcinoma rectum a decade ago and has an end colostomy in situ. She was admitted recently for bilateral pyelonephritis during which she was also worked up for possible neoplastic recurrence, but it was negative.
On examination she had local tenderness over right side of the scalp region with no pulsations of superficial temporal artery felt. The artery felt cord like and was tender. All other peripheral arterial pulsations were normally felt. There was no limb weakness but right plantar response was extensor. No was no signs of meningeal irritation. Cranial nerve examination, sensory and examination for coordination was unremarkable. There was no sign of other systemic involvement.
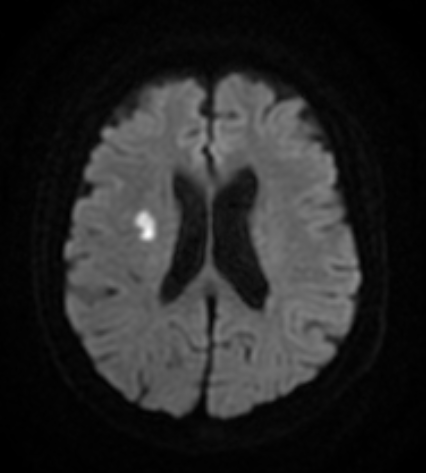
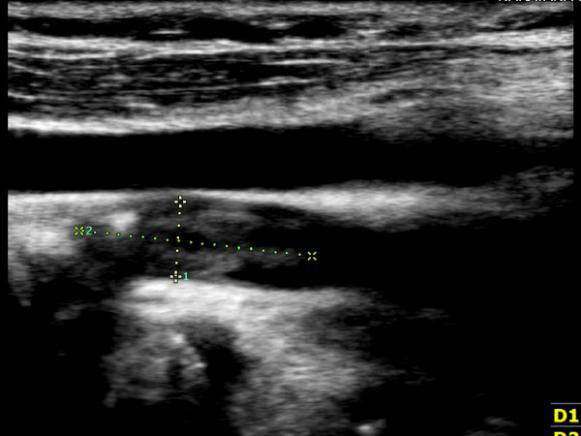
She underwent gadolinium enhanced MRI of brain with MRAngiography that showed an area of acute infarct in right central semiovale region (Figure 1). There was also a long segment narrowing of right carotid vascular system noted starting from the carotid bifurcation through the middle cerebral artery. The left counterpart was apparently normal (Figure 2). The doppler study of superficial temporal artery on the right side showed feeble arterial pulsation (Figure 3) and that of the carotid vasculature showed heterogenous plaque at the right carotid bifurcation causing 70-80% focal narrowing (Figure 4). Other laboratory parameters were significant for high blood sugar (382mg/dl) and ESR (68 mm at 1 hour) levels. Her other vasculitic markers including ANA, ANCA, APLA and viral serology were negative.


With the provisional diagnosis of giant cell arteritis and right hemispheric acute ischemic stroke she was initiated on corticosteroid therapy, antiplatelet and statin therapy with measures taken to address other risk factors for stroke. Superficial temporal arterial biopsy was taken and it was reported as normal. Her headache and right eye visual symptoms drastically improved with three days of high dose intravenous methylprednisolone therapy. She did not have any neurological progression and started improving on her left sided symptoms in the next few days. She was soon subjected to carotid endarterectomy for her carotid vascular disease. She is continued with oral prednisolone therapy and is asked for close follow up. It is further planned to treat her with tocilizumab and reduce the administration of corticosteroid based on her response to therapy considering her co-morbid conditions.
Discussion
Giant cell arteritis (GCA) is relatively a common cause of sytemic vasculitis affecting the large and medium sized vessels [1, 2, 3, 4, 5, 6]. It commonly affects the extracranial carotid vasculature [1, 2]. It commonly affects people more than 50 years of age and women are more commonly affected than men. It is a chronic granulomatous inflammatory condition but exact etiology of GCA is still unknown. Some familial clustering of this disorder is seen and an association with HLA-DR4 haplotype is proposed indicating a genetic predisposition [7, 8]. Some observations also suggest suggest an infectious origin particulary the ones caused by Mycoplasma pneumoniae, Chlamydia pneumoniae, and parvovirus B19 [9, 10, 11, 12, 13].
Clinically it can present with myalgia, low grade fever and other constitutional symptoms. Headache is a common presentation. The patients can also have jaw claudication, amaurosis fugax or sudden visual loss, abnormal temporal arterial pulsations and abnormal consistency of the vessel on palpation [1, 2, 3]. Other neurological manifestations such as transient ischmeic attack, ischemic stroke, dementia, mononeuropathies and polyneuropathies are also reported [14, 15, 16, 17, 18, 19].
The patients usually have anemia of chronic disease. ESR is very commonly elevated (higher than 50mm at 1 hour) in these patients and a normal ESR is exceptional [20, 21]. Diameter of the superficial temporal artery maybe increase and hypoechoic wall thickening (halo sign) may be seen on ultrasonography of temporal artery. It is proposed that the lack of a halo sign can in practice rule out a GCA [22, 23]. There can also be edematous arterial wall swelling and stenosis [24, 25]. The diagnosis should be confirmed by temporal arterial biopsy [26]. Histopathology may show features of vasculitis characterised by a predominance of mononuclear infiltrates or granulomas, usually with multinucleated giant cells. But in general the sensitivity of biopsy is low. Ultrasonographic guidance for site of biopsy may be useful to increase the yield.
The American College of Rheumatology has proposed a diagnostic criteria for GCA [27]. The features included in the criteria are
- Age at onset >50 years.
- New headache.
- Temporal arteries abnormalities.
- Erythrocyte sedimentation rate >50 mm/hour.
- Positive temporal artery biopsy.
Presence of three or more of these features has a high sensitivity and specificity for diagnosis.
Treatment of choice in GCA is corticosteroids [28, 29]. It is usually given as prednisolone at a dose of >0.75mg/kg (1- 1.5mg/kg) daily. The duration and tapering of steroid therapy is not very clear. To reduce the usage of corticosteroids owing to its side effect profile, tocilizumab can be used. In general the treatment is needed for several months to years depending on the response to therapy.
Conclusion
Acute ischemic stroke is a common neurological emergency. Atherosclerosis is a common etiology of stroke world-wide. Stroke preceded by (or associated with) headache should raise a suspicion of etiology other than atherosclerosis. Vasculitis, even though relatively an uncommon cause of stroke, is a common underlying etiology in painful strokes. In elderly population, GCA is a common vascular inflammatory disorder that can present with headache, visual symptoms and rarely, stroke. It is important to have a high index of suspicion to identify such vasculitic or other conditions that can cause stroke especially if stroke is associated with headache. Missing the ‘second’, often hidden underlying etiology of stroke can have unfavourable consequences.
References
-
Evans JM, Hunder GG (2000) Polymyalgia rheumatica and giant cell arteritis. Rheum Dis Clin North Am 26(3): 493-515.
-
Boiardi L, Cantini F, Salvarani C (2002) Polymyalgia rheumatica and giant-cell arteritis. N Engl J Med 347(4): 261-271.
-
Garcia-Porrua C, Gonzalez-Gay MA, Rivas MJ, Rodriguez- Ledo P, Llorca J (2001) Epidemiology of biopsy proven giant cell arteritis in northwestern Spain: trend over an 18 year period. Ann Rheum Dis 60(4): 367-371.
-
Armona J, Gonzalez-Gay MA, Rodríguez-Valverde V, Figueroa M, Fernández-Sueiro JL, et al. (1995) [Giant cell arteritis. A study of 191 patients]. Med Clin (Barc) 105(19): 734-737.
-
Calvo Romero JM, Magro Ledesma D, Ramos Salado JL, Bureo Dacal JC, Arrebola García JD, et al. (2000) Giant- cell arteritis: a descriptive study in southwestern Spain. Ann Med Interna (Madrid) 17(2): 67-70.
-
Alexandre C, Barouky R, Becourt-Verlomme C, et al. (2001) Inaugural symptoms of Horton’s disease in a series of 260 patients. Rev Med Interne 22(7): 631-637.
-
Dababneh A, García-Porrúa C, González-Gay MA, Hajeer A, Thomson W, et al. (1998) Giant cell arteritis and polymyalgia rheumatica can be differentiated by distinct patterns of HLA class II association. J Rheumatol 25(11): 2140-2145.
-
Fietta P, Manganelli P, Zanetti A, Neri TM (2002) Familial giant cell arteritis and polymyalgia rheumatica: aggregation in 2 families. J Rheumatol 29(7): 1551-1555.
-
Elling H, Elling P, Olsson AT (1996) Synchronous variations of the incidence of temporal arteritis and polymyalgia rheumatica in different regions of Denmark; association with epidemics of Mycoplasma penumoniae infection. J Rheumatol 23(1): 112-119.
-
Fresemann T, Gerard HC, Wagner AD, Schmidt WA, Gromnica-Ihle E, et al. (2000) Detection of Chlamydia pneumoniae in giant cell vasculitis and correlation with the topographic arrangement of tissue-infiltrating dendritic cells. Arthritis Rheum 43(7): 1543-1551.
-
Blasi F, Cosentini R, Rimenti G, Moling O, Pristerà R, et al. (2000) Temporal arteritis associated with Chlamydia pneumoniae DNA detected in an artery specimen. J Rheumatol 27(11): 2718-2720.
-
Bosshard S, Calvet A, Duhaut P, Pinede L, Demolombe- Rague S, et al. (1999) Giant cell arteritis, polymyalgia rheumatica, and viral hypotheses: a multicenter, prospective case-control study. Groupe de Recherche sur l’Arterite a Cellules Geantes. J Rheumatol 26(2): 361-369.
-
Erdman DD, Espy M, Gabriel SE, Bjornsson J, Smith TF, et al. (1999) The role of parvovirus B19 in the pathogenesis of giant cell arteritis: a preliminary evaluation. Arthritis Rheum 42(6): 1255-1258.
-
Giansiracusa DF, Reich KA, Strogwater SL (1990) Neurologic manifestations of giant cell arteritis. Am J Med 89(1): 67-72.
-
Davis TE, Pascuzzi RM, Ross KL (1989) Mental status abnormalities in temporal arteritis: a treatable cause of dementia in the elderly. Arthritis Rheum 32(10): 1308- 1311.
-
Caselli RJ (1990) Giant cell (temporal) arteritis: a treatable cause of multi-infarct dementia. Neurology 40(5): 753-755.
-
Ben-Ami H, Fruchter O, Schapira D, Gallimidi Z, Gaitini D, et al. (2002) Giant cell arteritis complicated by spinal cord infarction: a therapeutic dilemma. J Rheumatol 29(7): 1556-1558.
-
Caselli RJ, Daube JR, Hunder GG, Whisnant GP, et al. (1988) Peripheral neuropathic syndromes in giant cell (temporal) arteritis. Neurology 38(5): 685-689.
-
Barland P, Chowdhry IA, Sinha J (2002) Brachial plexopathy as a presenting symptom of giant cell arteritis. J Rheumatol 29(12): 2653-2657.
-
Armona J, Blanco R, Martinez-Taboada VM, Uriarte E, Figueroa M, et al. (2000) Giant cell arteritis with an erythrocyte sediemtation rate lower than 50. Clin Rheumatol 19(1): 73-75.
-
Hunder GG, Salvarani C (2001) Giant cell arteritis with low erythrocyte sedimentation rate: frequency of occurrence in a population-based study. Arthritis Rheum 45(2): 140-145.
-
Demasi RJ, Lesar CJ, Meier GH, Sood J, Nelms CR, et al. (2002) The utility of color duplex ultrasonography in the diagnosis of temporal arteritis. J Vasc Surg 36(6): 1154- 1160.
-
Mates M, Nesher G, Shemesh D, Sonnenblick M, Abramowitz HB, et al. (2002) The predictive value of the halo sign in color Doppler ultrasonography of the temporal arteries diagnosing giant cell arteritis 29(6): 1224-1226.
-
Younger DS (2019) Giant Cell Arteritis. Neurologic clinics 37(2): 335-344.
-
Kanakis MA, Karahaliou M, Papaspyrou S, Revenas K, Sfikakis PP, et al. (2006) Colour duplex sonography of temporal arteries before decision for biopsy: a prospective study in 55 patients with suspected giant cell arteritis. Arthritis research & therapy 8(4): R116.
-
Hall S, Hunder GG (1984) Is temporal artery biopsy prudent? Mayo Clin Proc 59: 793-796.
-
Bloch DA, Hunder GG, Michel BA, Stevens MB, Arend WP, et al. (1990) The American College of Rheumatology 1990 criteria for the classification of giant cell arteritis. Arthritis Rheum 33(8): 1122-1128.
-
Kyle V (1991) Treatment of polymyalgia rheumatica/ giant cell arteritis. Baillieres Clin Rheumatol 5(3): 485- 591.
-
Hazleman BL, Kyle V (1993) The clinical and laboratory course of polymyalgia rheumatica/giant cell arteritis after the first two months of treatment. Ann Rheum Dis 52(12): 847-850.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury