Neurotization of Musculocutaneous Nerve with Intercostal Nerves Assisted with Videothoracoscopy Clinical Case of a Patient with Brachial Plexus Palsy
In total brachial plexus preganglionic lesions (C5 for T1), different extraplexual neurotizations are indicated for partial motor function restitution specially for the elbow flexion. Neurotization with intercostal nerves (ICN) [Spanish Acronym] to musculocutaneous nerve has been known and accepted during many years with different results. The customary technique as described by various authors is carried out by means of a large submammary incision to harvest three or four intercostal nerves. Then are anatomosed by direct suture or grafts to the musculocutaneous nerve or its motor branches. Based on a previous study by the author on the possibility of performing the dissection of the intercostal nerves by videothoracoscopy, we present a clinical case of a 29-year-old patient with a complete brachial plexus injury in which we performed this technique and its results at 2 years.
Case Description
A 24-year-old patient who had a traffic accident (motorcycle) presented a right brachial plexus palsy associated with a recovered head trauma as the primary diagnosis.
Clinically, the patient didn’t show any spontaneous recovery of his motor and sensory function in the affected limb after 5 months since the injury.
In the exploration, the muscle atrophy of the upper limb stood out; the trapezius muscle showed normal contraction (M5) and absence of supraescapular, rhomboids, and serratus anterior (M0) muscle function.
Scapulohumeral subluxation was evidenced. There was a diminution of sensitivity in all the limb, especially in dermatomes corresponding to root nerves C8-T1 (Figure 1).

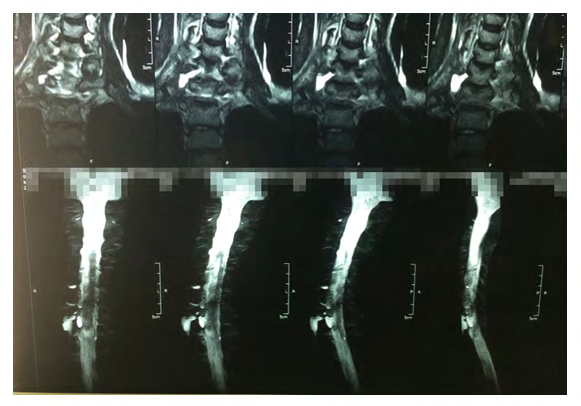
A electromyogram informed of severe denervation signs in all the plexus nerve roots that suggest radicular avulsions with no signs of reinnervation. In the magnetic resonance with myelography effect images suggesting dural injury at all the roots (Pseudomeningoceles) (Figure 2).
Intervention
Nerve reconstruction surgery was carried out after 5 months since the accident took place.
Technique Description
The surgery was started with general anesthesia and selective intubation with double-lumen tube on the left side, verifying the collapse of the right lung.
Cervical Time
Patient in supine decubitus position with thorax elevation and lateralization of head on the contralateral side. Approach the supra and infraclavicular plexus by an inverted-L incision through the posterior edge of the sternocleidomastoid muscle, parallel to the clavicle (Figure 3). Identification of roots C5-C6-C7-C8 and D1. The macroscopic aspect verified the avulsion and the presence of rootlets at the proximal level. The phrenic nerve showed no response to stimulation.
The identification and preparation of the musculocutaneous nerve at the infraclavicular level were carried out with an incision through the deltopectoral groove (Figure 4).

The neurotization of the suprascapular nerve with the spinal nerve through a termino-terminal suture with a monofilament of 9/0 as carried out (Figure 5).

Endoscopic Time Preparation
Endoscopic time (Figure 6)
- The patient was placed in the left lateral decubitus position.
- A 1 cm incision on the seventh right intercostal space on the mid-axillary line was carried out. A 10 mm trocar was introduced and a 10 mm optic was placed. The total collapse of the lung was verified.
- A 1 cm incision on the fourth right intercostal space of the sub-mammary region was carried out and a 10 mm trocar was introduced.
- A 0.5 cm incision on the fourth right intercostal space near the scapula, a 5 mm trocar, was introduced.
- A 1 cm incision on the sixth right posterior intercostal space and a 10 mm trocar as accessory port were introduced parietal pleura and the vascular-nervous intercostal branch was recognized.
- The third, fourth, and fifth intercostal spaces were identified.
- A parallel incision above the upper rib of the intercostal spaces previously described was carried out.
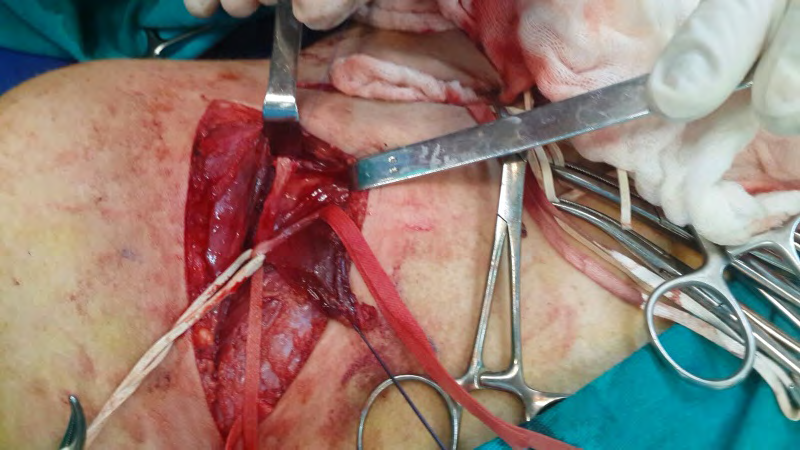
- The intercostal nerves were dissected from front to rear with blunt techniques, using Maryland and Grassper forceps and pulling rubber strip, while considering the internal mammary artery as the anterior boundary.
- With blunt techniques, the nerves were released clipping crossing vessels from the vascular bundle.
- Nerves were cut in the posterior side of the thoracic cavity. Each nerve was individually exteriorized in its most anterior and rear areas.
- The cavity was cleaned with 300 ml of physiological saline solution at room temperature.
- A 28 Fr chest tube was placed through the seventh right intercostal space toward the posterior side.
A tube oscillation and bubbling was noted. It was all closed with absorbable thread 1/0.
13. A complete expansion was verified and the trocars were removed under direct supervision. 14. Aponeuroses closure with absorbable thread 1/0. 15. Skin closure with non-absorbable thread 3/0.
The dissection time of each intercostal nerve was around 30 to 45 minutes.

Common Time
A small 4 cm incision in the axillary region was carried out in order to put the three dissected nerves back to this level.
It was followed by the adhesion of the intercostal nerves with fibrin glue and then by the relocation, at this level, of the musculocutaneous nerve. Two intercostal nerves were sutured with a termino-terminal technique and a small 2 cm graft was placed in. A small 2 cm graft was placed in the third intercostal nerve through a suture (Figure 7).

The patient stayed hospitalized for 3 days. On the third day, after the radiological control, the chest drainage tube was removed without complication. Total time of surgery is 4:30 hours.
Results
In the post-surgery control after two years, the shoulder was seen stable with recovery from the 30-degree abduction and the 90-degree elbow flexure (biceps strength M3) (Figures 8 & 9).

Figures 8: Result of biceps flexure M3 and 30-degree abduction.
Figures 9: Result of biceps flexure M3 and 30-degree abduction.
Discussion
In the brachial plexus surgery, one of the standard neurotizations for elbow flexure in the case of radicular avulsions, is that of the intercostal nerves with the musculocutaneous nerve [1, 2, 3]. The results vary between 40% and 75%, according to scholars [4, 5, 6]. Some authors even carry it out in cases with phrenic nerve plasy [7].
The described technique usually takes place through a sub-mammary approach with sub-periosteal dissection of the rib and release of the intercostal nerve, which is behind the former.
We describe the endoscopic technique, which presents the following advantages: immediate identification of the intercostal nerve by transparency at the level of the parietal pleura, easy-to-carry-out dissection, minimal number of incisions for the placement of trocars, and a small one to collect the three nerves. We could mention disadvantages such as the lesion of the parietal pleura and the need for a post-surgery pleural drainage [8, 9].
It is worth mentioning that it is likely to injure the intercostal nerve when using the monopolar dissecting hook (L-shaped tip) for dissecting the pleura. Similarly, we initially presented difficulty collecting the three nerves in a common place and creating a new window for this purpose.
In this case, we opted for the neurotization of the intercostal nerves, being these the only ones available given the absence of function of the phrenic nerve and the use of the spinal nerve accessory for the neurotization with the suprascapular nerve [10].
It is worth highlighting that this technique requires the intervention of a thoracic surgeon specializing in thoracoscopy to benefit from the advantages of this minimal- invasion surgery compared to open surgery.
Conclusion
After the start of the clinical application of an experimental work based on the neurotization of the intercostal nerves obtained through video-thoracoscopy with the musculocutaneous nerve (there is no such work on this technique’s use in the existing literature) and with the obtained result, it is possible to argue that this is a reproducible technique with many advantages for open surgery.
References
-
Lykissas MG, Kostas-Agnantis IP, Korompilias AV, Vekris MD, Beris AE (2013) Use of intercostal nerves for different target neurotization in brachial plexus reconstruction. World J Orthop 4(3): 107-111.
-
Alnot JY, Daunois O, Oberlin C, Bleton R (1992) Total paralysis of the brachial plexus caused by supra-clavicular lesions [in French]. Rev Chir Orthop Reparatrice Appar Mot 78(8): 495-504.
-
Chuang DCC (2010) Brachial plexus injury: nerve reconstruction and functioning muscle transplantation. Seminars in plastic surgery 24(1): 57-66.
-
Malessy MJ, Thomeer RT (1998) Evaluation of intercostal to musculocutaneous nerve transfer in reconstructive brachial plexus surgery. J Neurosur 88(2): 266-271.
-
Yuan-Kun T, Yi-Jung T, Chih-Han C, Fong-Chin S, Chih- Kun H, et al. (2014) Surgical Treatment for total root avulsion type brachial plexus injuries by neurotization: a prospective comparison study between total and hemicontralateral C7 nerve root transfer. Microsurgery 34(2): 91-101.
-
Liu Y, Lao J, Zhao X (2015) Comparative study of phrenic and intercostal nerve transfers for elbow flexion after global brachial plexus injury. Injury 46(4): 671-675.
-
Chuang DC, Epstein MID, Yeh MC, Wei FC (1993) Functional restoration of elbow flexion in brachial plexus injuries; resuls in 167 patients (excluding obstetric brachial plexus injury). J Han Surg 18(2): 285-291.
-
Caceres JP, Palazzi S, Palazzi JL Llusa M, Sanz M (2013) Dissection of intercostal nervs by means of assisted video thoracoscopy: experimental study. Journal of brachial plexus and peripheral nerve injury 8: 1-3.
-
Xu WD, Gu YD, Xu JG, Tan LJ (2002) Full-length phrenic nerve transfer by jeans of video-assisted thoracic surgery in treating brachial plexus avulsion injury. Plastic Reconstr Surg 110(1): 104-109.
-
Bonnard C, Anastaks DI (2001) Complete palsy. In: Gilbert A (Ed.), Brachial plexus injuries. Martin Dunitz, London, pp: 67-75.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury