Alternative Option to Treat Crowding by Direct Veneering Layering (Case Report)
Introduction: A thirty one years old male patient attended our private dental clinic complaining of crowding in the mandibular six anterior teeth. The patient refused any kind of orthodontics treatment. Also he refused any kind of treatment includes teeth preparation. After extra and intra-oral examination, a diagnostic cast was fabricated to analyze the patient’s smile line. Despite the fact that most of the corrected cases for orthodontics measures carried by indirect ceramic veneers, a direct veneering layering technique has been considered as the treatment option for this case .So the aim of this study is to introduce an alternative method to orthodontic approach for the management of crowded mandibular anterior teeth. Materials and Methods: Empress direct material® was selected for this case to carry out direct veneering layering technique. It is a product of Ivoclar Vivadent Company. A wax up pattern was made on a diagnostic cast to analyze the smile line and to estimate the level of the mandibular arch to get the best final aesthetic result. All the six anterior teeth were etched with 37% phosphoric acid and a fifth generation bonding of ivoclar was used (Excite F)..)® Results: A cosmetically acceptable aesthetic smile line has been achieved and the de-arrangement of the crowding was corrected with an acceptable level. The patient was satisfied with the results. Conclusion: For some cases, direct composite veneer layering is suitable, hassle free and cost effective alternative to orthodontic treatment or traditional porcelain veneers, with reasonable aesthetic results.
Introduction
The term Cosmetic Dentistry has become one of the most used terms in modern dentistry. Today, the term cosmetic dentistry has become vernacular across the globe. The interpretation of beauty may vary from one viewpoint to another but generally we may say the human smile is universal and it is a common thread to us all because it is a part of the beauty of the face and the main target for our patients is to match all the forms of beauty in the face. So in cosmetic dentistry you have to feel your patient and go deep inside his or her spirit because you are not just changing the smile but you may change the personality of your patient as this may be reflected on the psychology of your patient. Many patients may visit us in our daily practice looking for cosmetic correction and we may hear the following comment "Doctor I want that Hollywood smile, I am shy, I cannot smile freely" and some patients may say “I am always keeping my hand upon my face to hide my smile”. Accordingly, our treatment will not include restoring the structure of the teeth but the beauty as well. Still other factors have to be considered which are the treatment method, types of materials and techniques, socio- economic status of the patient in respect to the cost of the treatment and the longevity of the success in respect to prognosis of the treatment. Furthermore, the role of the treatment could be reflected on the main complaint of the patient. That means the main complaint of many patients could be aesthetic correction before functional demand and this may affect method and the type of treatment. Different methods of treatment are available in restoring the teeth with aesthetic dentistry. These may include indirect crowns, veneers (direct veneer or indirect veneer), lumineers, onlays, inlays, whitening bleaching and invisible orthodontics treatment. The choice of treatment depends on many factors and as it was mentioned the socio-economic status of the patient may change the whole treatment plan even if it was the most suitably selected one. Regarding veneers aspects, many studies started long time ago. Most of the studies were concerned with indirect veneering and the effect of the bonding to the tooth structure. Then other studies started to compare the advantages and disadvantages of indirect and direct veneers. Garber DA [1] in 1989 studied the effect of direct composite veneers versus etched porcelain laminate veneers. It was concluded that the etched porcelain restoration offers the advantages of increased strength, color, stability and biocompatibility for a veneering material using composite merely as a luting agent [1], where as Pape FW, et al. [2] in 1991 studied the Bond strength of etched In-Ceram(R) to tooth enamel and they concluded that under the environmental condition of the mouth In- Ceram porcelain, even if it is layered with Vitadur porcelain, cannot be durably bonded to enamel at present [2]. Then further studies were conducted, Calamia JR [3] in 1996 made a review of the current status of etched porcelain veneer restorations and reached a conclusion that the union of etched porcelain, composite resin cement and etched enamel has proven over this time to be an exceptionally durable and highly esthetic restoration [3]. As the time was passing the introduction of direct veneer layering became familiar in the field of cosmetic dentistry. Behle C [4] in 2000 presented a case study of Placement of direct composite veneers utilizing a silicone buildup guide and intraoral mock-up. The study presented a simplified technique that combines function with aesthetics by utilizing an intraoral composite mock- up for initial communication and a lingual/incisal silicone stent of the mock-up to transfer the information to the definitive restorative buildup .Also it was mentioned that the availability of composite materials with improved physical and optical characteristics facilitates the development of enhanced aesthetics while maintaining vital function [4]. Since that time many studies were carried out and many clinical cases were presented concerned with direct veneer layering techniques. Stefano Ardu & Ivo Krejci [5] in 2006 presented a biomimetic direct composite stratification technique for the restoration of anterior teeth. They described a simplified layering technique based on a biomimetic approach for large anterior Class 4 restorations. The proposed layering technique is based on a modified layering technique where palatal enamel and dentin masses are replaced with the same quantity of a micro hybrid enamel and dentin shade composites, respectively, while for the thin buccal enamel layer a micro filled resin composite is used. Transparencies and, whenever necessary, white spot characterizations, are created by interposing blue and white effect masses between dentin mamelons, under buccal enamel. The combination of a microfilled composite with a microhybrid composite substituting the same quantity of lost enamel and dentin better mimics the physical and optical characteristics of the natural tooth. The biomimetic composite restoration may be considered an interesting alternative to ceramics, minimizing invasiveness, chair time and costs for patients [5]. On other hand, further studies started to present the advantages of restoring fractured teeth with direct composite veneering technique. In 2007 Vivien Thiemy Sakai, et al. [6] presented a clinical case report which indicated a Predictable esthetic treatment of fractured anterior teeth. It was stated that placement of direct composite restorations allows clinicians a conservative method of restoring fractured anterior teeth to the original shape and color. In addition to that, it was concluded that after finishing and polishing, an esthetic and natural-looking restoration was achieved, which completely satisfied the functional and esthetic expectation of the patient and dental team [6]. Also in 2008 Michael Koczarski [7] presented a method of Smile makeover by utilizing direct composite resin veneers. It was mentioned that one must take into account the entire aesthetic zone, along with the mechanics of restoring the teeth to proper form and function. To make this effort even more challenging, the clinician is in full control and completely accountable for making the direct composite resin restorations from which the smile is created [7]. On other hand many cases were reported indicating treatment plan for orthodontics complains by cosmetic correction. Süha Türkaslan & Kivanç Utku Ulusoy in 2009 reported clinical case of esthetic rehabilitation of crowded maxillary anterior teeth utilizing ceramic veneers. The paper described ceramic veneers can be an alternative treatment to orthodontic therapy under variety of preparation forms when patient has anterior mal alignment and rejects the orthodontic treatment and it was concluded the new smile line was satisfactory for the patient and the esthetics was considered as excellent [8]. Also by Suha Türkaslan & Çagri Turna in 2009 reported clinical case of esthetic rehabilitation of misplaced dental arch after fracture of anterior maxillae and it was concluded that Ceramic veneers can be a solution for patients with mal positioned anterior teeth even the situation is severe and excessive tooth reduction is need [9]. Furthermore, Ji-Eun Moon, et al. [10] in 2010 reported a clinical case of esthetic restorations of maxillary anterior teeth with orthodontic treatment and porcelain laminate veneers. They described satisfying esthetic results obtained by the distribution of space for restoration by orthodontic treatment and porcelain laminate veneers in uneven space between maxillary anterior teeth. It is proposed that the use of orthodontic treatment for re-distribution of the space and the use of porcelain laminate veneers to alter crown anatomy provide maximum esthetic and functional correction for patients with irregular interdentally spacing [10]. Still other reports indicated the use of direct veneer layering to facilitate the most acceptable aesthetic results also in many reports they used template with direct veneering layers. Martin B Goldstein [11] in 2010 used Template-assisted technique in direct composite veneers procedures [11]. Whereas Pontons-Melo JC, et al. [12] in 2011 reported a direct composite resin stratification technique for restoration of the smile. They mentioned that Composite resins can be used to improve the esthetics of the smile at a low cost and with relatively high clinical performance and they described an approach to restore and enhance the esthetic appearance of the anterior dentition through vital tooth whitening and the direct layering of composite resin during predictable esthetic procedures [12]. This article discusses a clinical case report concerned with aesthetic demand .In other words, the main complain of the patient is aesthetic correction for crowding of the lower anterior teeth but the patient refused orthodontics treatment and teeth preparation approach . The patient was clinically examined extra orally and intra orally and after complete assessment a certain method of treatment was decided which is direct veneers correction.
Materials and Method
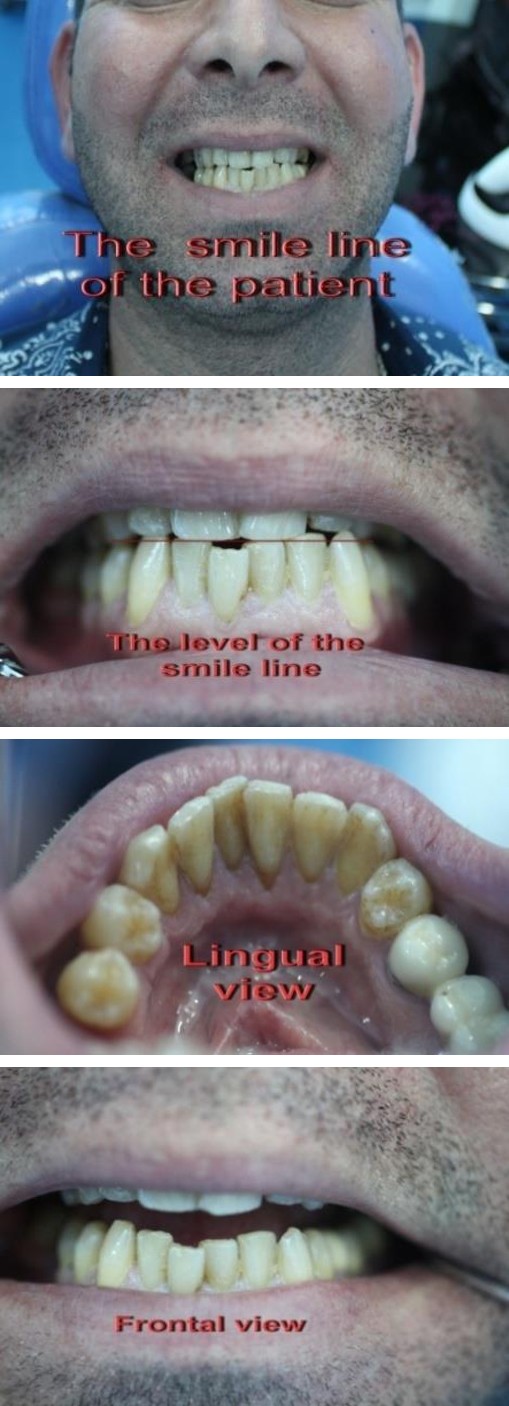
A young adult male 31 years old attended our private clinic complaining of aesthetic problem (Figure 1-A). By intra oral examination it was found that lower anterior teeth were crowded. The smile line for the patient was checked (Figure 1-B). The main complain of the patient was correction of the smile line and the crowding of the lower mandibular anterior teeth but the patient refused any kind of orthodontics treatment (Figure 1-C). The patient visited many dental clinics. The solution he received was orthodontics treatment. Some dentists gave him the opinion of full preparation bridge coverage of the six anterior teeth which was completely rejected by the patient. So the main demand of the patient was: 1. Any treatment plant that does not include any kind of orthodontics treatment and gives final esthetic result. 2. Any treatment plan that does not include any kind of teeth preparation and give final esthetic result. Accordingly, we started to analyze the smile line of the patient after taking an impression in which a study cast was fabricated .Then we started wax up on the diagnostic cast to estimate the level of the smile line and to estimate the final picture result of the six anterior teeth labially and lingually (Figure1-D).
| A B | ||
| C D | ||
| Figure 1 (A-D): Aesthetic problem in a young adult. | ||
| Hence, our choice of treatment was direct veneering layering technique | ||
| according to the demand of the patient. Here it should be mentioned that | ||
| the treatment plan could be one of the following options: | ||
| 1. Orthodontics treatment (i.e. 3dorthline aligners). | ||
| 2. Lumineer. | ||
| 3. Veneers-which could be direct veneer (which was our choice of | ||
| treatment), or indirect veneer | ||
Clinical approach
One of the advantages of our direct approach is the avoidance of pain preparation which means no anesthesia is required. This is a great advantage especially for apprehensive patient .So we started with good scaling and polishing for the entire teeth and motivated our patient for two important considerations: 1-To keep maintaining good oral hygiene avoiding as much as possible smoking.
Regarding the selection of the desired color, the desired overall shade should be selected by holding the Vita shade tab in the middle third of the tooth prior to desiccation. Then the whole six anterior teeth were etched with 37% phosphoric acid for at least 1-2 minutes despite the fact that 20 seconds are required (Figure 2-B) .Then after washing and drying, a fifth generation bonding by ivoclar was used which is Excite F (Figure 2-C). Then each tooth was completed using simplified Empress direct layering technique where Dead-Soft foil (Den-Mat) was used to isolate the tooth to be veneered from the adjacent. Then final polishing and blistering was carried out by using polishing discs made by pentron clinical (Figure 2-D).
| A B C | ||
| D | ||
| Figure 2 (A-D): Many materials are used 3M (Supreme Feltik, Z350), etc. | ||
Result and Discussion
| A B | ||
| C D | ||
| Figure 3 (A-D): Lingual surface was adapted as well to a comfortable level | ||
| concerning the incisal margin level. | ||

On the other hand the lingual surface was adapted as well to a comfortable level concerning the incisal margin level (Figure 3-C). Discussing the final results with our patient revealed the satisfaction of our patient. The patient was very happy with a comfortable feeling (Figure 3-D). Although such a treatment may take from two to three hours and sometimes even more, but our patient was completely satisfied and this is our main goal for any kind of treatment but still we have to refer to the education level of the patient followed by maintaining good oral hygiene (Figure 4- A, B, C, D, E, F, G, H).
| A B | ||
| C D | ||
| G H | ||
| Figure 4 (A-H): Completely satisfied and maintaining good oral hygiene. |

Conclusion
Through displaying most of orthodontics cases corrected by cosmetic approach and not by direct orthodontics treatment, we found that most of the cases were treated with indirect veneers where facial preparation is needed with anesthesia. In many occasion the patient demand may play a role in determining the treatment plan. Our approach in this clinical case report granted us certain advantages in which we can say that Direct Composite veneers layering are generally good for patients who are looking to enhance the look of their smile without the cost, time and pain involved with traditional porcelain veneers. Also the length of the direct veneers procedure varies with each individual patient. Some people choose to quickly patch up one or two teeth, while others change their entire smile, which may result in a two to three hour appointment like in our existing case. So in this case there is no laboratory procedure which means that the treatment may be finished in one session. On the other hand, the matching of the color and adjusting the high spot with very nice final result is under the control of the clinician and this can be an impressive predictable method to achieve the maximum benefit of esthetic result. Still we have to mention that although direct veneers are not as strong as porcelain veneers and require more maintenance (they are known to chip and stain more easily than porcelain veneers); direct composite veneers typically last up to four to eight years. The good news is that unlike porcelain veneers, composite veneers can be easily repaired and even removed if you have the desire to do so. Finally, directveneers are by far the most affordable and direct veneer option on the market. The reason that they are so reasonably priced when compared to porcelain veneers is because the procedure takes less time and is a more simple process(no laboratory procedure is involved). Overalls a conclusion, direct composite veneers are one of many great choices if your patients are looking to enhance their smile.
References
-
Garber DA (1989) Direct composite veneers versus etched porcelain laminate Veneers. Dent Clin North Am 33(2): 301-304.
-
Pape FW, Pfeiffer P, Marx R (1991) Bond strength of etched In-Ceram(R) to tooth enamel, ZWR 100(7): 450-453.
-
Calamia JR (1996) The current status of etched porcelain veneer restorations. J Philipp Dent Assoc 47(4): 35-41.
-
Behle C (2000) Placement of direct composite veneers utilizing a silicone buildup guide and intraoral mock-up. Pract Periodontics Aesthet Dent 12(3): 259-266.
-
Ardu S, Krejci I (2006) Biomimetic direct composite stratification technique for the restoration of anterior teeth. Quintessence Int 37(3): 167-174.
-
Sakai VT, Anzai A, Silva SM, Santos CF, Machado MA (2007) Predictable esthetic treatment of fractured anterior teeth: a clinical report. Dent Traumatol 23(6): 371-375.
-
Koczarski M (2008) Smile makeover utilizing direct composite resin veneers, Dent Today 27 (12): 76-79.
-
Türkaslan S, Ulusoy K (2009) Esthetic rehabilitation of crowded maxillary anterior teeth utilizing ceramic veneers: a case report. Cases J 2: 8329.
-
Türkaslan S, Turna C (2009) The esthetic rehabilitation of misplaced dental arch after fracture of anterior maxillae: a case report. Cases J 2: 8723.
-
Moon JE, Kim SH, Han JS, Yang JH, Lee JB (2010) Esthetic restorations of maxillary anterior teeth with orthodontic treatment and porcelain laminate veneers: a case report, J Adv Prosthodont 2(2): 61-63.
-
Martin B Goldstein (2010) Template-assisted direct composite veneers. Dent Today 29(2): 124, 128-129.
-
Pontons-Melo JC, Furuse AY, Mondelli J (2011) A direct composite resin stratification technique for restoration of the smile. Quintessence Int 42(3): 205- 211.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells