Expression of Oncofoetal Marker Carcino Embryonic Antigen in Oral Squamous Cell Carcinoma
Objective: Expression of the oncofoetal glycoprotein, carcinoembryonic antigen (CEA), has been extensively studied, particularly regarding its potential role as a marker of early cancer and as a prognostic indicator. CEA has been the hallmark of many neoplasms and has been observed in several malignancies and is also being pursued as a target for anti-cancer therapy. This study explored the status of this biochemical entity in the oral squamous cell carcinoma (SCC). Method: The data analyzed in the current study relate to a total of 100 patients. Out of which 25 were in the control group and 75 were Patients presenting with stage I or Stage II tumors of the oral cavity. This study was conducted in MSRDC University Hospital in the Department of Oral & Maxillofacial Surgery and its associated satellite centers during Jan 2012 to June 2016. Only patients diagnosed with primary OSCC, previously untreated, presenting with tumours of oral cavity were included in the study. All samples were studied immunohistochemically. Result: The results showed that all samples in control group had negative CEA expression and CEA was expressed at an elevated level (60 out of 75 samples ie 80%) in majority of grade I and the grade II SCC. Conclusion: In Conclusion, Expression of CEA in elevated levels were noticed in majority of grade I and grade II OSCC. If the results from this study can be validated with a larger sample size, a role can be attributed to this tumour marker in oral neoplasia.
Introduction
Oral Cancer is a disease of antiquity. Sushruta Samhita, a Sanskrit treatise of surgery, written in the Indian context gives a description of oral cancer. Its aggressiveness to spread locally involving surrounding structures causes disfigurement, affects function, and leads to physical and psychological discomfort ultimately affecting the quality of life. Oral cancer [more than 90% are oral squamous cell carcinomas (OSCC)] [1] is the third most common cancer in India [2] with an average 5-year survival rate of approximately 60% [1]. This poor survival rate has not improved in the past 3 decades despite improvements in therapeutic strategies [3]. This may be due to most of the OSCC cases are diagnosed at a late stage and no reliable early diagnostic marker is available. Detection of OSCC is currently based on expert clinical examination and histological analysis of suspicious areas, but it may be undetectable in hidden sites. Therefore, sensitive and specific biomarkers for OSCC may be helpful to screening high-risk patients [4]. Coons, et al. in 1941[5] first described an immune fluorescence technique for detecting cellular antigens in tissue sections. This marked the beginning of immunehistochemistry (IHC) [6]. Initially begun as a diagnostic tool, immunohistochemistry (IHC) today has far surpassed its initial expectations. Today, we are indeed in an era of “translational crossroads for biomarkers,” and IHC will remain centre stage in the demonstration of newer monoclonal antibodies [7]. Carcinoembryonic antigen (CEA) is an oncofetal antigen which was discovered by Gold & Freeman [8, 9]. The antigen was first isolated from human fetal intestine and adult colon cancer tissue [8, 9]. Initially, CEA was thought to be specific for colon cancer but several studies have showed its versatility. CEA has been the hallmark of many neoplasms and its levels were reported to be elevated in the early stage of head and neck cancers [10]. This antigen has been extensively studied, particularly regarding its potential role as a marker of early cancer and as a prognostic indicator [11]. In this study, we have explored the expression of this biochemical entityoncofoetal marker carcino embryonic antigen in early oral squamous cell carcinoma. This study is in continuation of a previous pilot study. The pilot study was conducted in Kidwai memorial institute of oncology, Bangalore. The observations of the study were published in 2006 by one of the authors of the current study. The current study in addition to exploring the status of CEA in OSCC also aims to validate the observations of the previous pilot study.
Materials and Methods
This study was conducted in MSRDC University Hospital. OSCC samples were collected in the Department of Oral & Maxillofacial Surgery at MSRDC University Hospital during Jan 2012 to June 2016. Only patients diagnosed with primary OSCC, previously untreated, presenting with tumours of oral cavity were included in the study. Diagnoses were confirmed from hematoxylin and eosin-stained sections and graded by the same experienced pathologist at MSRDC University Hospital. TNM status was based on clinical examination. Normal tissue obtained from operculectomy, canine exposures and around partially impacted wisdom tooth were included in the control group. All test samples were collected prior to treatment, and the primary treatment consisted exclusively of surgical resection of the tumor. Sample size was calculated using Master software (CMC Vellore, version 1. From the cited study concomitant analysis of salivary tumor markers, assuming the sensitivity of CEA for detecting oral cancer from samples to be 71%, with a relative precision (allowable error) of 10% and desired confidence interval of 95%, the required number of sample size was 75 patients. The patients were informed about the study and their consent was sought for their participation in the study. Detection systems used were Ultravision Quanto detection system HRP & UltraVision DAB plus substrate system. Polyclonal antibody was used.
Tissue Specimens and Immunohistochemistry
The tissue specimens were fixed in 10% formalin before embedding in paraffin wax. For immune reactivity studies with CEA Ultravision Quanto detection system HRP & UltraVision DAB plus substrate systems were used. 3 microns’ thick sections were mounted on slides coated with Poly-L-Lysine and placed in an incubator at 60°C for 01 hour. The sections were deparaffinized in 3 changes of Xylene for 5 minutes each. The sections were then rehydrated in 3 changes of Alcohol for 5 minutes each. The slides were then washed under running tap water for 5 minutes. Antigen was retrieved by HIER method in decloaking chamber using citrate buffer pH 6. Slides were then cooled in jar containing buffer for 20 mins. The slides were washed again under running tap water for 5 minutes. The Slides were then incubated in 3% hydrogen peroxide block for 20 minutes to block endogenous peroxidase. The slides were washed under running tap water for 5 minutes. The slides were incubated in Tris buffer for 5 minutes. Protein block was applied and incubated for 5 minutes at room temperature to block nonspecific background staining. Primary antibody was applied and incubated as per manufacturer's recommended protocol. Two changes of Tris buffer for 5 minutes each was carried out. Primary antibody enhancer was applied and incubated for 10 min at room temperature. Two changes of Tris buffer for 5 minutes each was carried out. HRP polymer was applied and incubated for 15 minutes at room temperature. Two changes of Tris buffer for 5 minutes each was done. Incubation with DAB plus substrate system for 5 minutes was done. Slides were washed in distilled water. They were then counterstained with hematoxyline for few seconds. Dehydration in 3 changes of alcohol was carried out. Clear in changes of Xylene and Mounted in D.P.X. Analyses for the immunoreactivity of the antibodies were performed under light microscopy.
Scoring of Immunostaining
To determine the CEA immunostaining score, we used the design proposed elsewhere, with modifications [12]. In brief, this semi-quantitative score was established as: each sample was scored twice—(A) for the percentage of IHC Positive cells. The extent of marker expression was quantified by evaluating the percentage of the positive staining cells in relation to the whole cancer cells in the core. A score of 0 = 0%, 1= <30%, 2=30-60%, 3= >60%. The Image J software was used to count the cells and (B) for the intensity of the immunostaining. The intensity of marker expression was quantified using the following scores: 0 = negative, 1 =weakly positive, 2 = moderately positive, 3 = strongly positive. Addition of both scores allowed the final Score ranging from 0–6. We further categorised the score as 0 = Negative, 1-2 = Mild positive, 3-4 = Moderately Positive, 5-6 =Strongly Positive. A double-blind analysis was performed by two independent observers (Tables 1 & 2).
Measure of Agreement
| I | No. of | No. of | d | % of | ||||||||||||
| K | app | a | ||||||||||||||
| samples | samples | samples | 9 | 5% C | I | P | -Value | |||||||||
| (κ) | ||||||||||||||||
| nspected | matche | Matched | ||||||||||||||
| 75 | 66 | 88.00% | 78.44 - 94.36 | 0.9361 | <0.001* |
Table 1: Assessment agreement between the two examiners.
*denotes that the agreement was statistically significant Table 1: Assessment agreement between the two examiners.
| Rater | Kappa | SE of Kappa | P-Value | |||||||
| A | 0.9348 | 0.0428 | <0.001* | |||||||
| B | 0.9349 | 0.0428 | <0.001* |
Table 2: Assessment agreement for the number of trails within each examiner.
*denotes that the agreement was statistically significant Table 2: Assessment agreement for the number of trails within each examiner.
Statistical Test
Chi Squared test, Multivariate analysis and Kappa analysis were used. R analysis software package was used to carry out the statistical tests.
Results
Patient Data
The data analyzed in the current study relate to a total of 100 patients. Out of which 25 including 8 males & 17 females were in the control group and 75 including 31 males & 44 females were Patients presenting with stage I or Stage II tumors of the oral cavity. The age of the patients ranged from 14 to 60 years (Mean being 29 yrs) in the control group and 29 to 80 years in the test group. The mean age of the group was found to be 56yrs. 39 Patients in the study group were <56yrs and 36 Patients were ≥56yrs of age. 43 (57%) of cases enrolled in the study were diagnosed as SCC, grade I; 24 (32%) as SCC, Grade II and 8(11%) as SCC, Grade III. All the tumors in the study were of clinical Stage I and stage II. 29(39%) were stage I and 46(61%) were stage II. There was significant association noticed between CEA expression and the two study groups. In the test group the expression of CEA was as follows: 9 (12%) were negative, 13 (17.33%) were mild positive, 34 (45.33%) were moderately positive, 19 (25.33) were strongly positive. All the samples in the control group showed negative expression of CEA. The association between the grading of the tumor and the expression of the CEA was found to be not significant statistically. However, out of 43 samples that were graded as grade I, 32 (74%) samples showed moderate to strong positive. The association between stage group and CEA expression was found to be statistically significant (P<0.05). Those with moderate and severe CEA expression were found to be more in Stage 2. 63 (84%) were found to be users of tobacco. 12(16%) have never used any form of tobacco or alcohol. The association between CEA expression and tobacco use (both groups included) was found to be statistically significant (P<0.001). Higher number of samples who had negative CEA expression was found to be non-users of tobacco while those with a positive CEA expression were found to be users of tobacco (Table 3,4).
| Tobacco Use=Yes | Tobacco Use=No | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CEA Expression | χ2 | P-Value | |||||||||||||||||
| n | % | n | % | ||||||||||||||||
| Negative | 15 | 21% | 19 | 66% | 18.167 | <0.001* | |||||||||||||
| Mild | 22 | 31% | 4 | 14% | |||||||||||||||
| Moderate | 26 | 37% | 5 | 17% | |||||||||||||||
| Severe | 8 | 11% | 1 | 3% | |||||||||||||||
| Total | 71 | 100% | 29 | 100% |
Table 3: Association between CEA expression and tobacco use (both groups together).
*denotes significant association Table 3: Association between CEA expression and tobacco use (both groups together).
| CEA | ||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Negative | Mild | Moderate | Strong | p-value | ||||||||||||||||||||||||||||
| N | % | N | % | N | % | N | % | |||||||||||||||||||||||||
| 1 | 6 | 14.00% | 5 | 11.60% | 21 | 48.80% | 11 | 25.60% | ||||||||||||||||||||||||
| HP | 2 | 1 | 4.20% | 7 | 29.20% | 9 | 37.50% | 7 | 29.20% | 0.371 | ||||||||||||||||||||||
| 3 | 2 | 25.00% | 1 | 12.50% | 4 | 50.00% | 1 | 12.50% | ||||||||||||||||||||||||
| 1 | 7 | 24.10% | 8 | 27.60% | 11 | 37.90% | 3 | 10.30% | ||||||||||||||||||||||||
| Stage | 0.004* | |||||||||||||||||||||||||||||||
| 2 | 2 | 4.30% | 5 | 10.90% | 23 | 50.00% | 16 | 34.80% | ||||||||||||||||||||||||
| No | 2 | 16.70% | 3 | 25.00% | 4 | 33.30% | 3 | 25.00% | ||||||||||||||||||||||||
| Tobacco | 0.753 | |||||||||||||||||||||||||||||||
| Yes | 7 | 11.10% | 10 | 15.90% | 30 | 47.60% | 16 | 25.40% | ||||||||||||||||||||||||
Table 4: correlation of CEA with the histopathological grading, Tumor staging and usage of tobacco.
* denotes statistical significance Table 4: correlation of CEA with the histopathological grading, Tumor staging and usage of tobacco.
In our study, we noticed that the immunoreactivity was always confined to the tumour cells, but there was occasional vascular staining (Table 5). Staining was in the cytoplasm of tumour cells and restricted to the
| CEA – Dependant variable | ||||
|---|---|---|---|---|
| Standardized Coefficients | 95.0% Confidence Interval | |||
| p-value | ||||
| Beta | Lower | Upper | ||
| Age | -.091 | .435 | -.045 | .020 |
| Sex | .243 | .036 | .055 | 1.579 |
| HP | -.061 | .605 | -.716 | .420 |
| Stage | .402 | <0.001* | .642 | 2.096 |
| Tobacco | .111 | .345 | -.549 | 1.549 |
Table 5: Multivariate analysis.
* denotes statistical significance Table 5: Multivariate analysis.
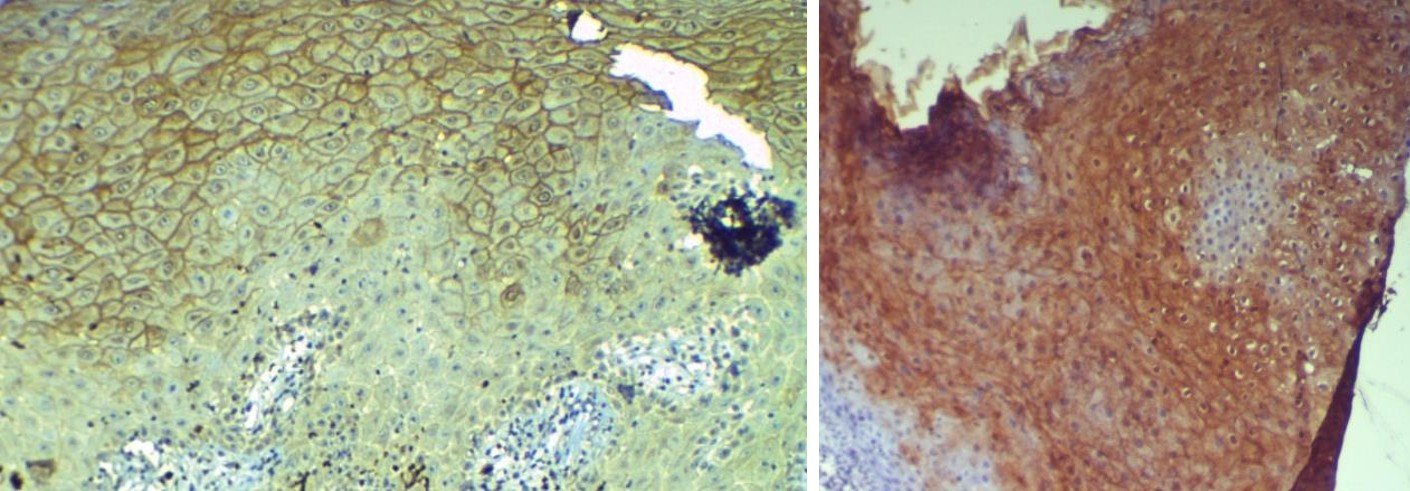
Figure 1a Figure 1b
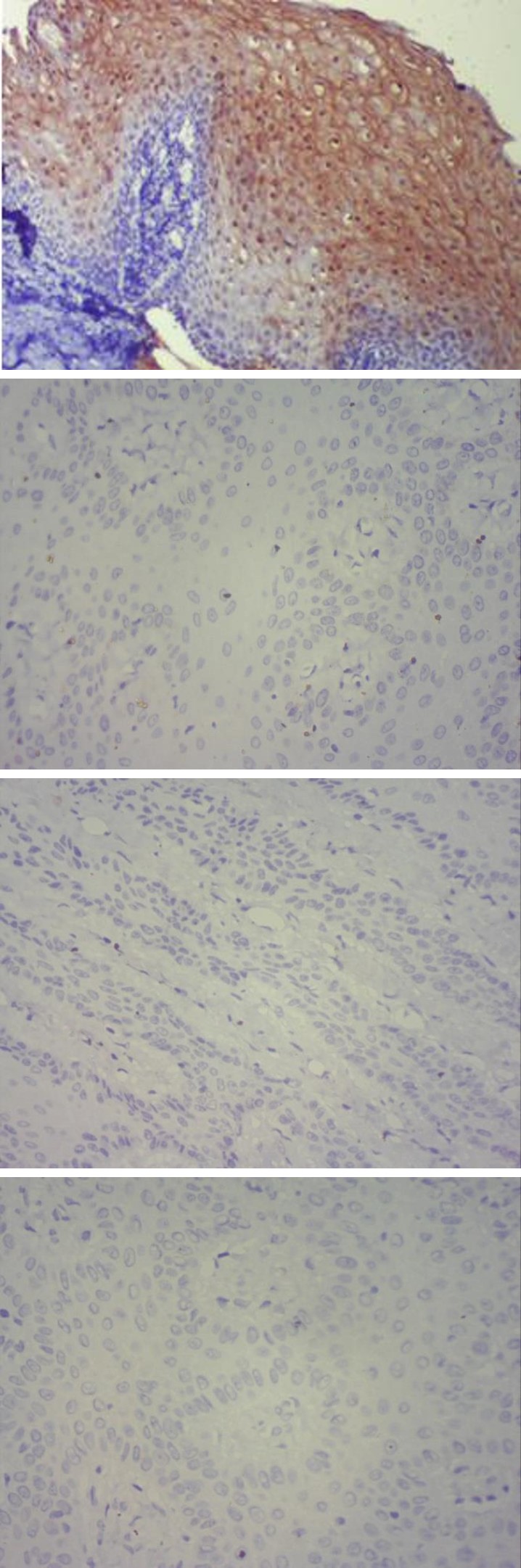
Figure 1c
Figure 1(a,b,c): Carcinomatous mucosa showing positivereaction to CEA
Figure 2a
Figure 2b
Figure 2c Figure 2(a,b,c): Normal mucosa showing negative reaction to CEA.
Discussion
In the current study the expression of oncofoetal marker CEA in OSCC has been examined. The study shows that in the oral oncogenic process induced by the insult due to tobacco habits, CEA is expressed at an elevated level (60 out of 75 samples i.e., 80%) in majority of grade I and the grade II SCC. Honarmand MH, et al. [13] found that salivary CEA was elevated in OSCC samples when compared to the controls suggesting the application of CEA in early detection of patients. Barak V, et al. [14] stated in their study that CEA severs as a useful tumor marker in head & neck cancer patients. Chuanshu Yuan, et al. [15] concluded that CEA had diagnostic values for patients with Oral/OroPharyngeal Squamous (OSCC/OPSCC) Cell Carcinoma. Kuo WR, et al. [16] found that 28% of head and neck cancers tested positive for CEA [16]. Kass ES, et al. [17] reported a high percentage of head and neck cancers to be positive for CEA in their study [17]. Yanagawa T [18] in his study found 40% of the oral tumours were positive for CEA in comparison to 78% of the tumours of maxillary origin [18]. Kulpa J, et al. [19] in their study found that CEA, SCC-Ag, CYFRA 21-1, and NSE were increased above the cutoffs in squamous cell lung cancer patients [19]. Yuan C [15] also found that CEA had high sensitivity and specificity in OSCC/OPSCC. Inal E [20] in his study found sensitivity rates as follows: 10.7% for ferritin, 21.4% for CEA, 42.9% for SCC antigen. The specificity was 100% for all the markers [20]. In our study, we obtained a sensitivity of 88%, specificity of 100% and accuracy of 91%. Saghravanian N, et al. [21] in their study found that immunohistochemistry can be helpful for differential diagnosis of Adenoid cystic carcinoma (AdCC) and polymorphous low-grade adenocarcinoma (PLGA), particularly that for CEA. He H, et al. [22] in their study Concluded saying the measurement of CEA and CA-50 levels in saliva were more sensitive than in serum. This may be more useful as prognostic indicators in early diagnosis of oral and salivary malignant tumors. Pai, et al. [10] in their study found that CEA was expressed at an elevated level in grade I and most the grade II SCC. In the present study, the association between the grading of the tumor and the expression of the CEA was found to be not significant statistically. However, out of 43 samples that were graded as grade I, 32 (74%) samples showed moderate - strong positive. Experimental studies with CEA-expressing cells from head and neck cancers have demonstrated that induction of CEA-mediated cytotoxic T lymphocytic response may be feasible in these cancer cells to inhibit their growth [10]. Additional studies with larger sample size and in conjunction with other tumour-specific markers should provide insights into the possible utility of CEA in Oral Squamous cell carcinoma which causes high morbidity and mortality. However, the current study has a few drawbacks. Firstly, we have looked for the expression of tissue CEA in OSCC. Comparing the values of tissue CEA with serum or/and salivary CEA would probably add more value to this study. Secondly, comparing the expression of two or more tumor markers may have provided valuable insight. As this was a self-funded study, financial constraints could be attributed to the drawbacks.
Conclusion
In the current study the expression of CEA in cell blocks was measured by immunohistochemistry and we found that all samples in control group had negative CEA expression while 66 (88%) samples in test group had different levels of CEA expression for early stages of oral cancer. The association between the grading of the tumor and the expression of the CEA was found to be not significant statistically. However, CEA was expressed at an elevated level in majority of grade I and the grade II SCC (60 out of 75 samples ie 80%). Out of 43 samples that were graded as grade I, 32 (74%) samples showed moderate - strong positive.
Acknowledgment
All authors had the opportunity to review the analysis plan and outcome, participated in the preparation of this report, and provided final approval. The corresponding author had full access to the data and takes final responsibility for the decision to submit this manuscript for publication. We would like to acknowledge Mr Thejasvi & Dr Kalyan for their statistical support.
References
-
Rethman MP, Carpenter W, Cohen EE, Epstein J, Evans CA, et al. (2010) Evidence-based clinical recommendations regarding screening for oral squamous cell carcinomas. J Am Dent Assoc 141(5): 509-520.
-
Globacon (2012) Estimated cancer incidence, Mortality & Prevalence worldwide in 2012. IARC section of cancer surveillance.
-
Elashoff D, Zhou H, Reiss J, Wang J, Xiao H, et al. Prevalidation of Salivary Biomarkers for Oral Cancer Detection. Cancer Epidemiol Biomarkers Prev 21(4): 664-672.
-
Wu JY, Yi C, Chung HR, Wang DJ, Chang WC, et al. Potential biomarkers in saliva for oral squamous cell carcinoma. Oral Oncol 46(4): 226-231.
-
Coons AH, Creech HJ, Jones RN (1941) Immunological properties of an antibody containing a fluorescent group. Proc Soc Exp Biol Med 47: 200-202.
-
Ramos-Vara JA (2005) Technical Aspects of Immunohistochemistry. Vet Pathol 42(4): 405-426.
-
Jambhekar NA, Chaturvedi AC, Madur BP (2008) Immunohistochemistry in surgical pathology practice: a current perspective of a simple, powerful, yet complex, tool. Indian J Path Microbiol 51(1): 2-11.
-
Gold P, Freeman SO (1965) Demonstration of tumor- specific antigens in human colonic carcinoma by immunological tolerance and absorption techniques. J Exp Med 121: 439-462.
-
Gold P, Freeman SO (1965) Specific carcinoembryonic antigens of the human digestive system. J Exp Med 122(3): 467-481.
-
Pai SB, Pai RB, Lalitha RM, Kumaraswamy SV, Lalitha N, et al. (2006) Expression of oncofoetal marker carcinoembryonic antigen in oral cancers in South India-a pilot study. Int J Oral Maxillofac Surg 35(8): 746-749.
-
Veronesia G, Pelosib G, Sonzognib A, Leon ME, D’Aiutoa M, et al. (2005) Tumour CEA as predictor of better outcome in squamous cell carcinoma of the lung. Lung Cancer 48(2): 233-240.
-
Klein M, Picard E, Vignaud JM, Marie B, Bresler L, et al. (1999) Vascular endothelial growth factor gene and protein: strong expression in thyroiditis and thyroid carcinoma. J Endocrinol 161: 41-49.
-
Honarmand MH, Farhad-Mollashahi L, Nakhaee A, Nehi M (2016) Salivary Levels of ErbB2 and CEA in Oral Squamous Cell Carcinoma Patients. Asian Pac J Cancer Prev 17 (3): 77-80.
-
Barak V, Meirovitz A, Leibovici V, Rachmut J, Peretz T, et al. (2015) The Diagnostic and Prognostic Value of Tumor Markers (CEA, SCC, CYFRA 21-1, TPS) in Head and Neck Cancer Patients. Anticancer Res 35(10): 5519-5524.
-
Yuan C, Yang K, Tang H, Chen D (2016) Diagnostic values of serum tumor markers Cyfra21-1, SCCAg, ferritin, CEA, CA19-9, and AFP in oral/oropharyngeal squamous cell carcinoma. OncoTargets Ther 9: 3381- 3386.
-
Kuo WR, Lee KW, Ho KY, Tsai SM, Chiang FY, et al. (1999) Tissue polypeptide antigen, carcinoembryonic antigen, carbohydrate antigen, and CA125 levels as tumor markers in squamous cell carcinoma of the head and neck. Kaohsiung J Med Sci 15(3): 152-158.
-
Kass ES, Greiner JW, Kantor JA, Tsang KY, Guadagni F, et al. (2002) Carcinoembryonic antigen as a target for specific antitumor immunotherapy of head and neck cancer. Cancer Res 62(17): 5049-5057.
-
Yanagawa T, Hayashi Y, Nishida T, Yoshida H, Yura Y, et al. (1986) Immunohistochemical demonstration of carcinoembryonic antigen (CEA) on tissue sections from squamous cell head and neck cancer and plasma CEA levels of the patients. Int J Oral Maxillofac Surg 15(3): 296-306.
-
Kulpa J, Wójcik E, Reinfuss M, Kołodziejski L (2002) Carcinoembryonic antigen, squamous cell carcinoma antigen, CYFRA 21-1, and neuron-specific enolase in squamous cell lung cancer patients. Clin Chem 48(11): 1931-1937.
-
Inal E, Laçin M, Asal K, Ceylan A, Köybaşioğlu A, et al. (2004) The significance of ferritin, lipid-associated sialic acid, CEA, squamous cell carcinoma (SCC) antigen, and CYFRA 21-1 levels in SCC of the head and neck. Kulak Burun Bogaz Ihtis Derg 12(1-2): 23-30.
-
Saghravanian N, Mohtasham N, Jafarzadeh H (2009) Comparison of immunohistochemical markers between adenoid cystic carcinoma and polymorphous low-grade adenocarcinoma. J Oral Sci 51(4): 509-514.
-
He H, Chen G, Zhou L, Liu Y (2009) A joint detection of CEA and CA-50 levels in saliva and serum of patients with tumors in oral region and salivary gland. J Cancer Res Clin Oncol 135(10): 1315-1321.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells