Oral Mucocele: The Lingering Lump of the Lower Lip-A Case Report
Mucocele is a common lesion of the oral mucosa that results from an alteration of minor salivary glands due to a mucous accumulation causing limited swelling. It is formed when the main duct of a minor or major salivary gland is obstructed or torn with subsequent extravasation of the mucus into the fibrous connective tissue so that a cyst like cavity is produced. Although non-threatening and painless, it can be bothersome for patients while eating and speaking. Thus, it is essential for a dentist to visually recognize oral lesions such as mucocele for its timely management.
RK, Prasanna KR and Gowri PB
AJ Institute of Dental Sciences, Kuntikana, NH-66. Mangaluru, PIN– 575004, Karnataka, India, Tel: +918905102696; E-mail: geonpauly@gmail.com essential for a dentist to visually recognize oral lesions such as mucocele for its timely management.
Keywords: Mucocele; Extravasation; Minor Salivary Gland; Diascopy
Introduction
A mucocele is a mucus retention phenomenon of the major and more commonly the minor salivary glands. This lesion has also been called a mucus extravasation phenomenon. Mucoceles are usually formed secondary to rupture of an excretory duct of a salivary gland, which leads to an outpouring of saliva into the surrounding tissues [1]. They are found to occur most commonly on the lower lip, followed by the floor of the mouth and the buccal mucosa being the next most frequent sites [2]. Hereby, we present a case of a recurrent mucocele of the lower lip in a 22-year-old male patient with emphasis on the histological and the treatment aspects.
Case Report
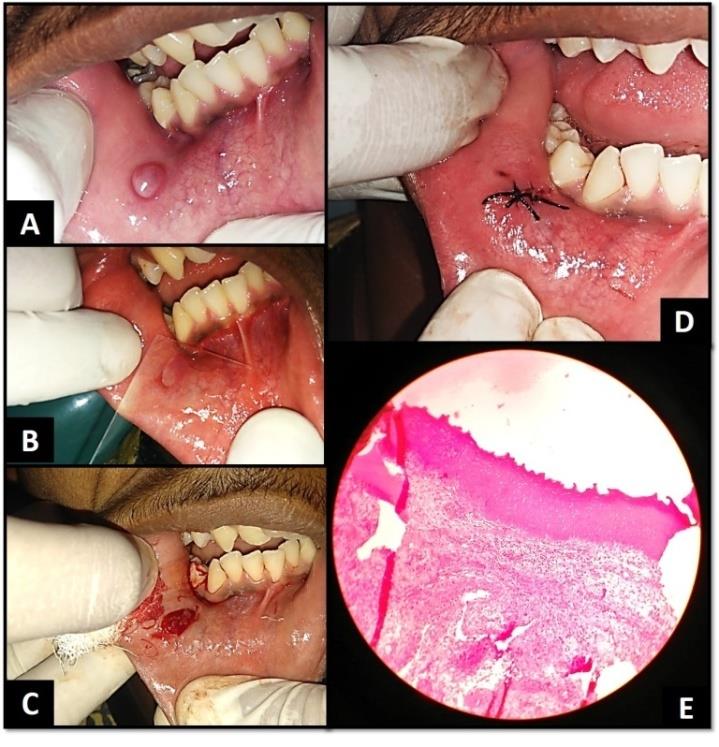
A 22-year-old male patient reported with a chief complaint of a growth inside the mouth on the right side of the lower lip since 9 months. He gave a history of recurrent growth in the same region which would rupture on its own and recur in a short time. The present growth which was rapidly growing in nature and was not associated with any type of pain had been since 1 week. His medical and dental histories were non-contributory. Clinical examination revealed a well-defined, raised solitary, pale pink, oval, translucent nodular growth with smooth surface and surrounding areas of erythema seen distal to the canine region on the labial mucosa on the right side located mid-way between the vermillion border of the lower lip and the labial sulcus. It was approximately 1 cm * 1 cm in size (Figure 1A). It was compressible, non- tender to touch and had a s sessile base. Based on the history and clinical examination a provisional diagnosis of mucocele was established. As a first line of investigation, a diascopy test was done which revealed the lesion did blanch (Figure 1B). After medical evaluation and obtaining informed consent, an excisional biopsy was performed under local anaesthesia and a single suture was placed across to approximate and arrest the bleeding (Figure 1C,D). An analgesic was prescribed for one day to prevent any possible pain that could result and post-operative instructions were given. Histopathological section revealed para-keratinized stratified squamous epithelium, with the adjacent deeper tissue showing an area of spilled mucin surrounded by chronic inflammatory cells (Figure 1E). The clinical and histological findings thus co-related and confirmed the final diagnosis as superficial mucocele of the lower lip. Patient was recalled after 1, 3 and 6 months without any episodes of recurrence.
Discussion
Mucocele are defined as mucus-filled cavities, which can appear in the oral cavity, appendix, gallbladder, paranasal sinuses, and lacrimal sac. The term mucocele is derived from a Latin word, ‘mucus’ and ‘cocele’ which means cavity. Mucocele is the 17th most common salivary gland lesions seen in the oral cavity [3]. It results from an alteration of the major or minor salivary glands due to a mucous accumulation or extravasation causing limited swelling. Two types of mucocele can appear - extravasation and retention. Extravasation mucocele results from trauma to salivary glands duct and the consequent spillage into the soft tissues around this gland. Retention mucocele appears due to a decrease or absence of glandular secretion produced by blockage of the salivary gland ducts [4]. Yamasoba, et al. [5] highlighted two etiological factors in mucocele: Traumatism and obstruction of salivary gland ducts. Mucocele of the minor salivary gland are very rarely larger in diameter and moreover always superficial [3]. They have no age or gender predilection but mainly occur in the children and young adults due to more chances of trauma. The lower lip is reported to be the most common site where the maxillary canine impinges on it. They usually present as discrete, small, translucent, soft, painless swelling of the mucosa ranging from normal pink to deep blue in color [6]. Spontaneous drainage of mucin especially in superficial lesions followed by subsequent recurrence may occur. The surface of long standing lesions may show fibrosis [7]. Superficial lesions take on a bluish to translucent hue, whereas deep lesions have normal mucosal coloration and bleeding into the swelling may impart a bright red and vascular appearance. The patient may relate a history of recent or past trauma to the mouth or face or the patient may have a habit of biting the lip. The differential diagnosis which can be considered are Blandin- Nuhn mucocele, benign or malignant salivary gland neoplasms, oral hemangioma, oral lymphangioma, venousvarix or venous lake, lipoma, soft irritation fibroma, Oral lymphoepithelial cyst, gingival cyst in adults, soft tissue abscess, and cysticercosis. Superficial mucoceles may be confused with cicatricial pemphigoid, bullous lichen planus and minor aphthous ulcers [8, 9]. Soft tissue swellings of lower lip usually invite the inclusion of traumatic fibroma (focal fibrous hyperplasia) and mucocele as the first candidates in list of provisional diagnosis. However, there have been reported cases where in a soft tissue swelling of the lower has even turned out to be an uncommon neural neoplasm such as a schwannoma [10, 11]. Mucocele is mostly a self-limiting condition and it often ruptures and leaves slightly painful erosions that usually heal within few days. Medications used widely include use of intralesional corticosteroid injections and gamma linolenic acid [12, 13]. There are three possible surgical approaches to management of Mucocele of the lips, cheeks and palate; complete excision, marsupialization and dissecting [11]. Surgical excision with removal of the involved accessory salivary gland has been indicated in cases of acute and chronic recurrences [14]. The excised tissue should always be submitted for the pathological investigation to confirm the diagnosis and to rule out other pathology of the salivary glands [14, 15]. Other treatment approaches such as Laser ablation, cryosurgery, and electrocautery have been used for conventional mucocele with variable success rates [15]. Vaporization by CO2 laser was suggested by Huang, et al. [16] but this technique was questioned since it does not allow histological examination of the lesion. Recent studies revealed that Erbium, KTP, and Diode lasers were ideal devices for oral soft tissues biopsy with poor thermal damage permitting a correct histological diagnosis [17]. The advantages of using laser include greater precision, a relatively bloodless surgical and postsurgical course, sterilization of the surgical area, minimal swelling and scarring, coagulation, vaporization, cutting, minimal or no suturing, and less or no postsurgical pain. The diode lasers have the ability to cut the tissue to perform coagulation and hemostasis and have a higher tissue ablation capacity and enough bleeding hemostatic properties compared to most laser systems [18]. Cryotherapy works on the principle of destroying tissues by application of extreme cold via different cryogen agents such as nitrous oxide gas, liquid nitrogen spray. As nitrous oxide gas is released from a high pressure to a low pressure into the cryotip, the drop in temperature results in freezing of tissues which is in accordance with the fact that for cell death to occur. The benefits of cryotherapy include absence of postoperative discomfort, bloodless surgical site, minimal to zero scarring, and excellent cosmetic results [19]. Moreover, cryotherapy carries the advantage of usefulness in candidates in whom surgery is contraindicated owing to any reason. Furthermore, this therapy is localized in action and can be repeated without any permanent side effects. On the other hand, cryosurgery has certain disadvantages such as unpredictable degree of swelling, lack of precision of depth in area of freezing, slight degree of necrosis, and sloughing which results in delayed healing which can be a bit problematic [19, 20]. Another novel technique in practice is the use of alginate impression material to define the boundaries of the lesion. In this technique to improve the visual access of the lesion, a thin mix of alginate impression material is injected into the lesion through a ruptured wall and then surgical removal with a scalpel blade is performed. This is an effective, safe and economical way of treating, especially an anterior lingual salivary gland mucocele, whilst ensuring complete removal and minimal chance of recurrence. If performed correctly, this technique should prove to improve the surgical compliance thereby curtailing the recurrence of oral mucocele [21].
Conclusion
Mucocele is predominately asymptomatic and self- limiting in nature. However, it could become irritating and also pose as an aesthetic or masticatory hindrance to the patient. Hence, a school based educational awareness program for both the child and parent at regular intervals and interception of the oral habit among children should in turn be a key factor for timely diagnosis and treatment of the asymptomatic ones. So, as dental professionals time to time monitoring is not just the first step in prevention but also our professional and moral obligation, for as it aptly said – “Care is an absolute, prevention is the ideal.”
References
-
Mustapha IZ, Boucree SA (2004) Mucocele of the Upper Lip: Case Report of an Uncommon Presentation and its Differential Diagnosis. J Can Dent Assoc 70(5): 318-21.
-
Singh RK, Singh A, Vivek R, Tripathi AA (2012) Mucocele: Review and a Case Report. Healtalk-A Journal of Clinical Dentistry 4(3): 38-39.
-
Nallasivam KU, Sudha BR (2015) Oral Mucocele: Review of Literature and a Case Report. J Pharm Bioallied Sci 7(2): 731-733.
-
Badjatia RG, Badjatia S, Kulkarni VK, Sharma DS (2014) National Journal of Dental Sciences and Research 2(1): 13-16.
-
Yamasoba T, Tayama N, Syoji M, Fukuta M (1990) Clinicostatistical Study of Lower Lip Mucoceles. Head Neck 12(4): 316-320.
-
Singh N, Chandra P, Agarwal S (2014) Orla Mucocele: A Case Report. J Dentofacial Sci 3(1): 47-50.
-
Indiarti IS, Ariawan D (2013) A Case Report of Mucocele. International Journal of Clinical Preventive Dentistry 9(4): 253-256.
-
Tabassum R, Shelat S, Parab S (2016) Extravasation Mucocele – A Case Report. International Journal of Life-Sciences Scientific Research 2(4): 404-406.
-
Rao PK, Shetty SR, Chatra L, Shenai P (2012) Oral Mucocele - A Mini Review. Dentistry 2: 153.
-
Gudi SS, Sikkerimath BC, Puranik RS, Kasbe SS (2013) Swelling on lower lip…not always a mucocele!!! Ann Maxillofac Surg 3(1): 98-99.
-
Baderca F, Cojocaru S, Lazăr E, Lăzureanu C, Faur A, et al. (2008) Schwannoma of the lip: Case report and review of the literature. Rom J Morphol Embryol 49(3): 391-398.
-
Ganguly R, Mukherjee M, Pal TK (2015) Laser Excision of a Mucocele: A Case Report. Journal of the International Clinical Dental Research Organization 7(2): 168-170.
-
Marathe S, Hebbal M, Nisa SU, Harchandani N (2014) Oral Mucocele: Presentation at a Rare Site with Review. International Journal of Advances in Health Sciences 1(4): 14-18.
-
Sangeetha KM, Srinivasasagar B, Rashmi G Chour (2014) Mucocele of Lower Lip-Case Report and its Differential Diagnosis. The Journal of Ayurveda and Holistic Medicine 2(9): 61-63.
-
Nayak V, Kini R, Rao PK, Bhandarkar GP, Kashyap RR, et al. (2016) Mucocele - A Benign Lesion of Minor Salivary Gland. Pacific Journal of Medical Sciences. 16(2): 35-38.
-
Huang IY, Chen CM, Kao YH, Worthington P (2007) Treatment of mucocele of the lower lip with carbon dioxide laser. J Oral Maxillofac Surg 65(5): 855-858.
-
Romeo U, Palaia G, Tenore G, Vecchio AD, Nammour S (2013) Excision of oral mucocele by different wavelength lasers. Indian J Dent Res 24(2): 211-215.
-
Sharma M (2015) An 810-nm Diode Laser for the Treatment of Mucocele. International Journal of Laser Dentistry 5(1): 22-25.
-
Moraes PC, Teixeira RG, Thomaz LA, Arsati F, Junqueira JL, et al. (2012) Liquid nitrogen cryosurgery for treatment of mucoceles in children. Pediatr Dent 34(2): 159-161.
-
Narula R, Malik B (2012) Role of cryosurgery in the management of benign and premalignant lesions of the maxillofacial region. Indian J Dent Sci 4(2): 63-66.
-
Kumaresan R, Karthikeyan P, Mohammed F, Fairozekhan AT (2013) A Novel Technique for the Management of Blandin-Nuhn Mucocele: A Case Report. International Journal of Clinical Pediatric Dentistry 6(3): 201-204.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells