Antibiotics in Dentistry-Double-Edged Sword
Since the advent of Antibiotics, the outlook of the Physician about the power drugs can have on diseases has changed. Antibiotics in the recent years have become one of the most frequently used as well as misused drugs. As a result, acquired drug resistance has become a major clinical problem. Antibiotics are regularly prescribed by the dentist for the prophylactic and therapeutic purposes for orodental infections. However, their enormous use & misuse has raised a growing concern, for rising public as well as professional awareness regarding the ill effects of their over usage and development of drug resistance. Preventive measures for avoiding drug resistance as well as appropriate use of antibiotics can overcome major clinical problems.
Introduction
The usage of Antibiotics have become extensive since the advent of antibiotics and the outlook of the physician about the power, drugs can have on diseases has changed. Antibiotics are regularly prescribed by the dentist for the prophylactic and therapeutic purposes for orodental infections. However, they have become one of the most frequently used as well as misused drugs in the recent times. Indiscriminate and inappropriate use of antibiotics has led to a global public health threat [1, 2] as declared by the WHO and announced the theme for the year 2011 as “Antibiotic resistance: “No action today, No cure tomorrow” [3]. India was the world’s largest consumer of antibiotics for human health in 2010 and first among the top global consumers consuming around 13 billion SU (standard units) [1, 4]. Antimicrobial resistance has resulted in difficulty in controlling the diseases not only at the national level but also worldwide. In the public health point of view it is important to emphasize on this global phenomenon and the strategies required for tackling this problem.
History
The term Antimicrobial Agents (AMA) is used to designate both synthetic as well as naturally obtained drugs that attenuate microorganisms. History of chemotherapeutic agents dates back to 350–550 CE with the traces of tetracycline found in the human skeletal remains from ancient Sudanese Nubia [5]. There have been histological studies suggesting of ancient antibiotic exposure from samples taken from the femoral midshafts of the late Roman period skeletons from the Dakhleh Oasis, Egypt (Cook et al., 1989) [6]. The Ehrlich’s phase in the history of chemotherapy (1890-1935) is marked by development of arsenicals-atoxyl for sleeping sickness, arsphenamine in 1906 and Neoarsphenamine in 1909 for syphilis. During the same period Paul Ehrlich also proposed the term “chemotherapy” [7]. The modern era of antibiotics was initiated in 1935 by demonstrating the therapeutic effect of a sulfonamide dye in pyogenic infection. Subsequently Sulfapyridine was the sulfonamide to be marketed in 1938. In 1929 Alexander Fleming discovered the Penicillin which could destroy the staphylococcus on the culture plate, but could not purify it. However, in the same year an Oxford team led by Howard Florey and Ernest Chain published a paper describing the purification of penicillin quantities sufficient for clinical testing [8]. In 1940s, Waksman and colleagues undertook a systematic search and of actinomycetes as a source of antibiotics and discovered Streptomycin in 1944 [7].
Antibiotic Use and Antibiotic Resistance in Dental Practice
The relationship between antibiotic usage and development of antibiotic resistance is highly multifaceted [9]. Antibiotic resistance refers to the unresponsiveness of a microorganism to an Antimicrobial agent, which could be either natural or acquired. Bacterial resistance has been defined by the CDC as ‘the result of bacteria changing in ways that reduce or eliminate the effectiveness of drugs, chemicals, or other agents to cure or prevent infections’ [10]. Acquired resistance due to usage of an AMA over a period of time poses a major clinical problem. Consumption of antibiotic in humans is increasing worldwide. In a study conducted by Thomas P Van Boeckel, et al. it was found that between 2000 and 2010, worldwide consumption of antibiotics by humans increased by 36%, with Brazil, Russia, India, China, and South Africa accounting for 76% of the increase, despite collectively representing only 40% of the world’s population [11]. Among the countries consuming the most antibiotics overall in 2010 India ranked number one with 13 billion SU. An estimated 80 percent of all antibiotics are used outside hospitals [4]. Also, there has been a tremendous increase in consumption of carbapenems (45%) and polymixins (13%) which are considered as the two last-resort classes of antibiotic drugs [1, 2, 11]. There has been an increased emergence of methicillin- resistant Staphylococcus aureus (MRSA), causing 54.8% surgical infections, as documented in India, and a steep rise in resistance was found from an isolation percentage of 29% in 2009 to 47% in 2014 from private labs [12]. Escherichia coli and related bacteria have become resistant to newer third-generation cephalosporins, indicating that they are difficult-to-treat extended- spectrum beta-lactamase (ESBL) producers [13]. In India, from 2008 to 2013, E. coli resistance to third-generation cephalosporins increased from 70 to 83 percent, and fluoroquinolone resistance increased from 78 to 85 percent. Among K. pneumoniae isolates, third-generation cephalosporin resistance decreased from 90 to 80 percent, and fluoroquinolone resistance increased from 57 to 73 percent. In 2014, carbapenem resistance was 57 and 12 percent among K. pneumoniae and E. coli isolates, respectively. Fawziah Marra et al founded that from 1996 to 2013, overall antibiotic use declined from 18.24 DID to 15.91 DID, and physician prescribing declined 18.2%, from 17.25 DID to 14.11 DID [14]. However, dental prescribing increased 62.2%, from 0.98 DID to 1.59 DID, and its proportionate contribution increased from 6.7% to 11.3% of antibiotic prescriptions. The prescribing practice of dentists is considered to be the second most prescribing profession in British Columbia [13, 14, 15, 16]. Although antibiotics have a wide range of application in dentistry from treating odontogenic infections, non- odontogenic infections and as a prophylaxis against focal and local infection, they should be used only as an adjunct to dental treatment and never alone as the first line of care [17]. The definitive indications for use of antibiotics in dentistry are limited and specific [18]. In a study conducted for studying the current trend of antimicrobial prescription for oral Implant surgery among dentists in India, it was concluded that there is a trend of antimicrobial agent misuse both in terms of drugs used and the protocols prescribed [19]. Prophylactic antibiotic for each implant surgery is not mandatory, however appropriate antibiotics are useful in preventing postoperative infections after implant placement [20].
Self Medication and Antibiotic Resistance
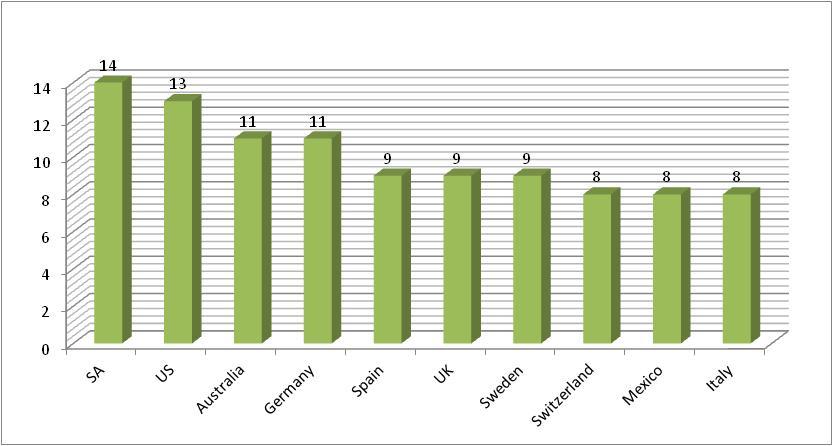
Another most common and obvious contributing factor of antibiotic resistant pathogens is self-medication [21]. Self-medication can be defined as obtaining and consuming one (or more) drug(s) without the advice of a physician either for diagnosis, prescription or surveillance of treatment. One of the primary reasons for people to indulge in self medication is the expensive healthcare system. When people in the developing countries cannot afford to pay for their health services due to the expensive healthcare system, they resort to self medication. Advertisements on television, radio and print media in addition to advice from family and friends are amongst other most common reason for people to start using medicines without professional help. Likewise, Australian studies have demonstrated a high rate of polypharmacy and self-directed medication use [21]. The frequency of dispensing antibiotics without a prescription was reported to be 22.3% in Saudi Arabia [22]. Previous studies have shown that in India the prevalence of self- medication was 37% & 17% in urban and rural population respectively [23]. Several studies show that self-medication is a global phenomenon resulting in major problems of wastage of resourses, increased drug resistance and causes serious health hazards such as adverse reactions and prolonged suffering [24, 25, 26]. The issue of medication misuse is not isolated to India alone, but it is an issue that needs to be addressed in any context where pharmaceuticals are widely available. The prevalence of self-medication in various countries is shown in Figure 1 [24].
Measures to Control Antibiotic Resistance
In 2001, WHO published the WHO Global Strategy for Containment of Antimicrobial resistance. Some of the measures to be taken to control the Antibiotic Resistance are: a) Development of comprehensive policies on antibiotics use including, bringing systematic interventions to educate healthcare professionals about prescribing antibiotics, developing infections control guidelines and keeping a control on the marketing and sales of the antibiotics. b) Develop a national surveillance system to determine antibiotic encounters in the community and identify targets for intervention, and could be used subsequently to assess the impact of interventions specifically in countries where there is a paucity of information on antibiotic use and a lack of drug registries or databases. c) Reduction in antibiotic resistance can only occur following a significant reduction in antibiotic use [9]. Most dental infections can be treated successfully by removal of the source and hence an emphasis must be made on appropriate prescription of antibiotics.
d) Constructive interactions with the pharmaceutical industry for ensuring appropriate licensure, promotion and marketing of existing antimicrobials and for encouraging the development of new drugs and vaccines [27].
Prevention of Antibiotic Resistance
In the pretext of Self medication, it is mandatory that the national governments show interest in this issue and formulate proper healthcare policies to combat the problem and regulate responsible self-medication. In addition the general population should also be educated about the appropriate use, advantages and limitations of the common antibiotic drugs that are used most often. Self-medication which is considered as an important cause of antibiotic resistance can be prevented or minimized by increased awareness and education in society [24]. Policy-makers need to consider the interplay between systemic, provider, dispenser and consumer factors in order to address the serious concern. An education campaign for health providers, pharmacists and the public around the risks of inappropriate use of antibiotics is warranted [21].
Conclusion
The emergence of antibiotic-resistant bacteria within the oral flora will have an impact on the prescribing of antibiotics in dentistry. The rise of antibiotic consumption and the increase in use of last-resort antibiotic drugs raises serious concerns for public health. If dentists, along with medical practitioners, can reduce the number of antibiotic prescriptions, the rate of resistance development may decline. Development of a surveillance system, to ascertain the numbers of prescriptions written and their appropriateness in dental practice are recommended.
References
-
Laxminarayan R, Chaudhury RR (2016) Antibiotic Resistance in India: Drivers and Opportunities for Action. PLoS Med 13: 1-7.
-
Laxminarayan R, Matsoso P, Pant S, Brower C, Røttingen JA, et al. (2016) Access to effective antimicrobials: A worldwide challenge. Lancet 387(10014): 168-175.
-
Suchi K, Praveen J (2015) Antibiotics in Dentistry a boon or a bane. J Dent App 2(1): 132-137.
-
Gelband H, Petrie MM, Pant S, Gandra S, Levinson J, et al. (2015) Center for Disease Dynamics, Economics & Policy. State of the World's Antibiotics, 2015. CDDEP: Washington, DC.
-
Bassett EJ, Keith MS, Armelagos GJ, Martin DL, Villanueva AR (1980) Tetracycline-labeled human bone from ancient Sudanese Nubia (A.D. 350). Science 209(4464): 1532-1534.
-
Aminov RI (2010) A brief history of the antibiotic era: lessons learned and challenges for the future. Front Microbiol 1: 134.
-
KD Tripathi Essentials of Pharmacology for Dentistry. Jaypee Brothers Medical Publishers 3rd (edn) Antimicrobial drugs: General Considerations.
-
Chain E, Florey HW, Gardner AD, Heatley NG, Jennings MA, et al. (2005) THE CLASSIC: Penicillin as a chemotherapeutic agent 1940. Clin Orthop Relat Res 439: 23-26.
-
Sweeney LC, Dave J, Philip AC, Heritage J (2004) Antibiotic resistance in general dental practice-a cause for concern. J Antimicrob Chemother 53: 567- 576.
-
Sujith JC, Thomas K, Mathai E, Antonisamy B, Holloway KA, et al. (2013) Patterns of antibiotic use in the community and challenges of antibiotic surveillance in a lower-middle-income country setting: A repeated cross-sectional study in Vellore, south India. J Antimicrob Chemother 68(1): 229-236.
-
Boeckel TPV, Gandra S, Ashok A, Caudron Q, Grenfell BT, et al. (2014) Global antibiotic consumption 2000 to 2010: An analysis of national pharmaceutical sales data. Lancet Infect Dis 14(8): 742-750.
-
Patel I, Hussain R, Khan A, Ahmad A, Khan MU, et al. (2017) Antimicrobial resistance in India. J Pharm Policy Pract 10: 1-2.
-
Garg AK, Agrawal N, Tewari RK, Kumar A, Chandra A (2014) Antibiotic prescription pattern among Indian oral healthcare providers: A cross-sectional survey. J Antimicrob Chemother 69(2): 526-528.
-
Marra F, George D, Chong M, Sutherland S (2016) Antibiotic prescribing by dentists has increased. JADA 147(5): 320-327.
-
Dar-Odeh NS, Abu-Hammad OA, Al-Omiri MK, Khraisat AS, Shehabi AA (2010) Antibiotic prescribing practices by dentists: a review. Ther Clin Risk Manag 6: 301-306.
-
Naveen N, Guru Suhas P, Vanishree N, Patnaik S, Bharath C, et al. (2015) Current Trends in Prescription of Antibiotics among Dentists Working in Various Dental Colleges of Bangalore City, India- A Cross Sectional Study. Int J Oral Health Med Res 2: 8- 14.
-
Ramu C, Padmanabhan TV (2012) Indications of antibiotic prophylaxis in dental practice- Review. Asian Pac J Trop Biomed 2(9): 749-754.
-
Ramasamy A (2014) A review of use of antibiotics in dentistry and recommendations for rational antibiotic usage by dentists. Int Arab J Antimicrob Agents 4: 1-15.
-
Datta R, Grewal YBJS, Singh A (2014) Current Trend of Antimicrobial Prescription for Oral Implant Surgery Among Dentists in India. J Maxillofac Oral Surg 13(4): 503-507.
-
Surapaneni H, Yalamanchili PS, Basha MH, Potluri S, Elisetti N, et al. (2016) Antibiotics in dental implants: A review of literature. J Pharm Bioallied Sci 8: 28-31.
-
Porter G, Grills N (2015) Medication misuse in India: a major public health issue in India. J Public Health 38(2): 150-157.
-
Aljadhey H, Assiri GA, Mahmoud MA, Al-Aqeel S, Murray M (2015) Self-medication in Central Saudi Arabia. Saudi Med J 36(3): 328-334.
-
Keshari SS, Kesarwani P, Mishra M (2014) Prevalence and pattern of self-medication practices in rural area of Barabanki. Indian Journal of Clinical Practice 25(7): 636-639.
-
Bennadi D (2014) Self medication: A current challenge. J Basic Clin Pharm 5(1): 19-23.
-
Rather IA, Kim BC, Bajpai VK, Park YH (2017) Self- medication and antibiotic resistance: Crisis, current challenges, and prevention. Saudi J Biol Sci 24(4): 808-812.
-
Montastruc JL, Bagheri H, Geraud T, Lapeyre-Mestre M (1997) Pharmacovigilance of self-medication. Therapie 52(2): 105-110.
-
Kumar GS, Adithan C, Harish BN, Sujatha S, Roy G, et al. (2013) Antimicrobial resistance in India: A review. J Nat Sci Biol Med 4(2): 286-291.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells