A Simplified Technique for Repair an Abutment Tooth under Preexisting Crown: A Case Report
This paper describes a simplified technique to repair an abutment using an old metal ceramic crown .this method uses a direct build up composite technique after bonding a tapered glass-fiber post followed buy by retrofitting the existing crown with a dual composite core material. This case report describes an innovative chairside technique for the recementation of a metal -ceramic crown overlaying a fractured maxillary second m left premolar.
Introduction
After many years of cementation of a metal ceramic crown, it is possible that patients may present with fractured post and core caused by fracture of an endodontically treated and crowned tooth in the esthetic zone may be embarrassing to both the patient and clinician [1]. Fracture of abutment tooth/teeth is not uncommon in clinical practice. It can be due to caries, trauma, composite debonding, occlusal overload, trauma during removal of a crown [2]. Fracture due to ferrules are based on the type of post used. Non repairable fracture are seen with less than 2mm ferrule and casted post and core localized below CEJ. Repairable fracture are seen with 2mm ferrule and using a fiber reinforced post and localized above cement-enamel junction. The cast dowel with 2 mm ferrule had a high fracture resistance but led to non-repairable fracture. Without ferrule, fiber post had a high incidence of repairable fracture [3]. Various authors have suggested different methods to replace or fabricate a post and core using retrograde post- supported core build up with the pre-existing crown or fixed partial denture [4, 5, 6, 7].
Using the retrofitting technique for fractured already restored abutment may be as a preferred option [8] whereas, the existing crown should fit precisely on the pre-existing finish line [9].
A 48-year-old healthy female presented to Prince Sultan specialist dental center in emergency with a dislodged metal ceramic crown overlaying a fractured core (Figure 1) on the maxillary left second premolar in an esthetic zone (Figure 2).
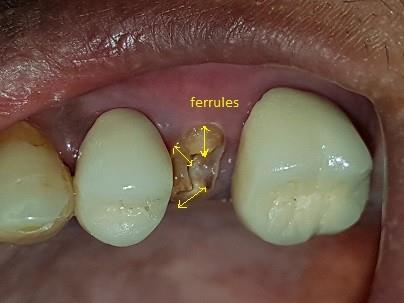

On examination, Patient had no medical history. Dental history did not reveal any past present symptom. She seeked for a rapid esthetic solution. Before the existing intact prosthesis is reused, a thorough investigation is mandatory to rule out any root fracture, violation of the biologic width due to trauma or damage to the supporting tissues [10]. Abutment tooth was thoroughly investigated, residual caries, existing restoration and cement were remove [11]. The maxillary left second damaged Premolar exhibits a sound dentine height of more than 2mm of ferrule (Figure 1) (arrows). It was properly endodontically treated and with a remaining fiber post in the post space (Figure 3).
The patient was given the option of retrograde fiber post-supported core build up and recementation the same metal ceramic crown, or fabrication of a new crown. Because of the costs and duration involved in the fabrication of a new metal ceramic crown the patient chose the same crown recemented. All the remnants of the old composite left on the fractured abutment were removed by using an ultrasonic scaler and the remaining fiber post was removed by using the combination diamond plus Largo burs (Figure 4) [12]. Nevertheless utmost care should be taken during removing to avoid a root perforation. On another hand the remaining fractured abutment was also removed from the inner surface of the metal ceramic crown (Figure 5).


After Preparation of the post space, the tooth was cleaned with water and air dry, then an etchant (Total etch, Ivoclar Vivadent, Schaan, Liechtenstein) was applied to the remaining tooth surfaces and post space for 15 seconds, rinsed, and air dried. Two coats of the bonding material (Prime and Bond NT, Dentsply) were applied to the tooth surface coronally to the finish line and light- polymerize for 20 seconds and then applied again in the post space. A prefabricated light post (D. T. Light-Posts; Bisco Inc. Illinois, USA) of appropriate size was adhesively cemented using dual-cure resin cement (Duoloink, BiscoInc, Schaumburg, USA) (Figure 6) [9].


Small amounts of dual-polymerizing core foundation composite (Bis-Core; Bisco Inc. Schaumburg, Illinois, USA) were used to build up layer by layer the core (Figure 7).

The post length was adjusted coronally and the new abutment was trimmed in an empirical way (Figures 8 & 9) till the ceramo metal crown seated completely with accurate margin fitting and with the same static and dynamic occlusal as before abutment fracture.

Figures 8 & 9: Removing of the excess of composite core.

The intaglio surface was lubricated with petroleum jelly, which allowed for easy removal of the crown and then filled with dual-polymerizing core foundation composite (Bis-Core; Bisco Inc. Schaumburg, Illinois, USA), then the patient was asked to close in the position of maximum intercuspation (MI) (Figure 11).

After an initial polymeristion with a light-polymerizing unit (QHL 75 Curing light, Dentsply) for 5 seconds and the excess composite material was gently removed from the margin with a probe. After removing the crowns, the core foundation composite was light-polymerized for 40 seconds the core surface was finished with a fine finishing bur with a fine grit diamond point. After sandblasting the inner surface of the crown in the lab, it was cemented in the clinic with using luting cement (RelyX Capsule, 3M, St. Paul, MN, USA) (Figure 12).

Discussion
Both bonded composite cores and amalgam required the presence of a minimum of 1.5-2 mm height of ferrule after crown preparation [13]. In our clinic case the remaining sound dentin (ferrule) was more than 2mm, so a fiber post and composite core foundation was a suitable option. Glass and quartz-fiber reinforced dowel systems compared to casted post and core have elastic moduli comparable to that of dentin [14]. Using the intaglio surface of the pre-existing crown fitted with dual cure composite allows the core to be placed exactly in the same location as the previous core because slight change in core location may change the path of insertion of the crown compromising its adequate stability and retention [9]. This technique compared to the technique using of a vacuum-formed thermoplastic template adapted to the PVS putty index obtained from the inner aspect of the crown [8] is more accurate, because there is no chance Corso, et al. and Kambhampati, et al. studied the effect of temperature changes (ranged from 4°C to 40°C and 25°C, 37°C, and 42° respectively) on the dimensional stability of PVS impression materials and found that though the changes in storage temperature had a statistically significant effect on the dimensional stability [15, 16]. This procedure eases chairside repair, reduced time and reduced cost. It was carried out in one appointment without temporization.
Conclusion
The technique described in this short clinical report enables clinicians to rebuild a composite post-and-core foundation using the existing crown without the original die or its replica and without temporization. It is simple, effective, affordable and time-saving way.
Acknowledgment
The author wishes to thank Professor Jilani Saafi, Professor in fixed prosthodontics at the faculty of dentistry of Monastir (Tunisia) for the great help and support in preparing this case report.
References
-
Lee JH (2017) A Digital Approach to Retrofitting a Post and Core Restoration to an Existing Crown. J Prosthodont.
-
De Backer H, Van Maele G, Decock V, Van den Berghe L (2007) Long-term survival of complete crowns, fixed dental prostheses, and cantilever fixed dental prostheses with posts and cores on root canal-treated teeth. Int J Prosthodont 20(3): 229-234.
-
Aggarwal V, Singla M, Yadav S, Yadav H, Sharma V, et al. (2014) The effect of ferrule presence and type of dowel on fracture resistance of endodontically treated teeth restored with metal-ceramic crowns. J Conserv Dent 17(2): 183-187.
-
Jahangiri L, Feng J (2002) A simple technique for retrofitting a post and core to a crown. J Prosthet Dent 88(2): 234-235.
-
Chan DC (2003) Technique for repair of multiple abutment teeth under pre-existing crowns. J Prosthet Dent 89(1): 91-92.
-
Sabbak SA (2000) Simplified technique for refabrication of cast posts and cores. J Prosthet Dent 83(6): 686-687.
-
Berksun S (2005) Rebuilding core foundations for existing crowns using a custom-made template. J Prosthet Dent 93(2): 201-203.
-
Patil PG, Tay K (2016) Modified technique to retrofit the crown on fractured core. J Interdiscip Dentistry 6(1): 50-53.
-
Mascarenas K, Aras MA, Fernandes AS (2013) Repair of fractured abutment teeth under pre-existing crowns: An alternative approach. Indian J Dent Res 24(1): 136-138.
-
Bhandari S, Rajagopal P, Bakshi S (2011) An interdisciplinary approach to reconstruct a fractured tooth under an intact all ceramic crown: Case report with four years follow up. Indian J Dent Res 22(4): 587-590.
-
Christensen GJ (1996) When to use fillers, build-ups or posts and cores. J Am Dent Assoc 127(9): 1397- 1398.
-
Gesi A, Magnolfi S, Goracci C, Ferrari M (2003) Comparison of Two Techniques for Removing Fiber Posts. Journal of endodontics 29(9): 580-582.
-
Ng CC, Dumbrigue HB, Al-Bayat MI, Griggs JA, Wakefield CW (2006) Influence of remaining coronal tooth structure location on the fracture resistance of restored endodontically treated anterior teeth. J Prosthet Dent 95(4): 290-296.
-
Tay FR, Pashley DH (2007) Monoblocks in root canals: A hypothetical or a tangible goal. J Endod 33(4): 391-398.
-
Corso M, Abanomy A, Di Canzio J, Zurakowski D, Morgano SM (1998) The effect of temperature changes on the dimensional stability of polyvinyl siloxane and polyether impression materials. J Prosthet Dent 79(6): 626-631.
-
Kambhampati S, Subhash V, Vijay C, Das A (2014) Effect of temperature changes on the dimensional stability of elastomeric impression materials. J Int Oral Health 6(1): 12-19.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells