Calcifying Epithelial Odontogenic Tumor
The calcifying epithelial odontogenic tumor is a rare benign odontogenic tumor that was first described by Pindborg in 1955. Later Shafer, et al. coined the term Pindborg tumor. It accounts for less than1% of all odontogenic neoplasms. This lesion is a locally aggressive benign odontogenic neoplasm arising from epithelial tissue. It occurs most commonly in 4th-5th decade of life and bears no gender predilection.
Introduction
Calcifying epithelial odontogenic tumor (CEOT) was first described by Pindborg in 1955. Pindborg tumor is a rare odontogenic neoplasm. World Health Organization in 1992 classified it as a benign odontogenic tumor, which is exclusively epithelial in the origin and posterior part of the mandible is more common. Commonly in 4th -5th decade of life. There is no gender predilection, unknown aetiology and no predisposing factors have been identified. Histologically it is characterized by squamous epithelial cells, calcifying masses, and homogeneous acellular material admixed with the tumor epithelium and stroma that have been identified as amyloid. The differential diagnosis for CEOT should include adenomatoid odontogenic tumor (AOT), calcifying odontogenic cyst (COC), ameloblastic fibroodontoma (AFO), and odontoma [1, 2, 3, 4, 5, 6, 7, 8, 9].
Case Report
A 40 year old female patient reported to the oral and maxillofacial pathology department G.Pullareddy dental college and hospital, Kurnool with a chief complaint of swelling in the lower front teeth region since 1 year and history of pain in that region since 2 months, which is severe, continues and relieves by itself and aggravates after eating. Her history revealed that she had trauma by a cricket ball 3 months back from then the size of swelling increased and pain also aggravated. She also had sleep disturbance since 3 months. On general examination she was well nourished and moderately built (Figures 1 & 2).

On intra oral examination a solitary swelling noticed
along the lower anterior teeth region of size 4.0×4.5cms and round oval in shape extending from 33 to 43 region and superioinferiorly from the buccal aspect to lingual aspect of lower anterior. The surface of the swelling is reddish when compared to adjacent mucosa, difficulty in mouth opening. On palpation the swelling is firm in consistency with tenderness


The patient was subjected to radiographic examination the panaromic view demonstrated well defined unilocular lesion extending from periapical region of 35 to 44 and superior inferiorly from alveolar crest region 31, 41 to inferior boarder of the mandible with well- defined sclerotic border the internal structure revels curved septa which are ill defined borders. Displacement of 31,32,41,42 with no evidence of rootresorption (Figures 3-5).


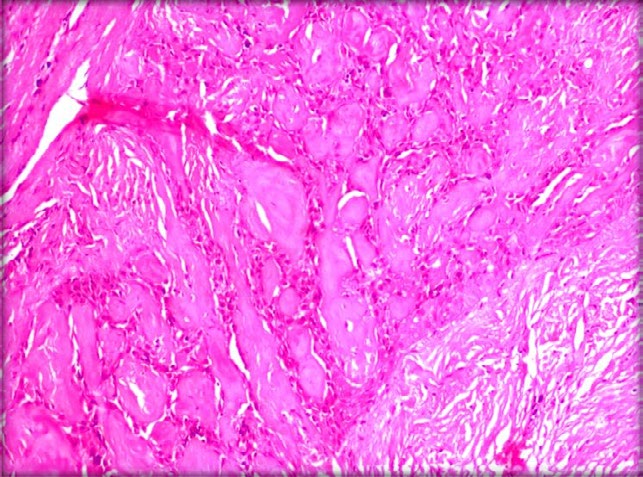
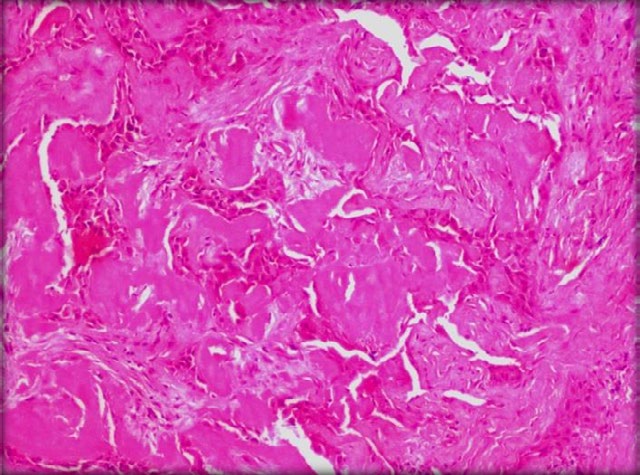
H&E stained soft tissue section on histopathological examination showed fibro vascular connective tissue and islands of epithelial cells. Areas of extensive deposition of homogenous eosinophilic material resembling amyloid are
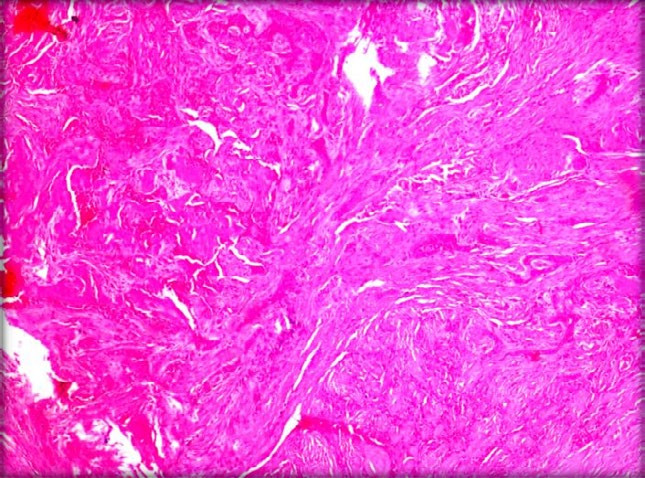
present all over the tissue. Individual cells are hyperchromatic and loosely cohesive at some areas. Connective tissue contains irregularly arranged collagen fibres with spindle shaped fibroblasts. Multiple haemorrhagic sites are also seen. Histopathological features suggestive of Calcifying epithelial odontogenic tumour.
Discussion
The Pindborg tumor (CEOT) was first reported by Pindborg in 1955, also referred as unusual ameloblastoma by Tuy, cysticodontoma by Stoppack, and Adenoid adamantoblastoma by Thoma. Calcifying epithelial odontogenic tumor is a rare odontogenic epithelial tumor. It accounts for <1% of all odontogenic tumors. CEOT present as painless slow growing mass in the mandible. Despite its odontogenic origin, its histogenesis is uncertain. The tumoral cells of the interosseous variant present morphology similar to the cells of stratum intermedium of enamel, shows a high activity of alkaline phosphatase and adenosine triphosphate [3]. Literature also states that the amyloid deposits within the Pindborg tumor are an immunologic response to these stratum intermedium cells. Some authors state that it arises from the remnants of dental lamina which are more likely to be the true progenitor cell known as the extraosseous type, it is also derived from the basal cells of gingival epithelium. The mean age is 40 with equal prevalence in men and women. CEOT present among the intraosseous is most common about 85% whereas extraosseous is less common about6% but both has similar histological features. Intraosseous CEOT is by far the most common, usually shows local invasiveness. They present as a painless mass with slow growth where as in this case the tumor started as a painful jaw swelling. When CEOT is located in maxilla the patient may complain of nasal congestion, epitasis and headache.
Extra osseous CEOT-this is a variant of CEOT which appears most commonly as a painless firm gingival mass the mucosa may show ulcerations due to trauma. It can be confused with fibrous hyperplasia, peripheral giant cell granuloma and epulis. There is a wide variation in clinical, radiological and histological aspects. Most investigators agree that the central type is usually located in the premolar and molar regions, with a mandibular to maxillary ratio of 2:1 or 3:1 [5]. Most CEOT cases, nearly 52%, are associated with impacted or unerupted teeth or odontomas. The prevalence in the molar region is 3 times greater than that of the premolar area and only some cases have been found around first and second molars [5].
Radiographically intraosseous shows radiolucency with calcifications while extraosseous shows bone erosion near the tumour. On histogenisis of intraosseous is believed to be from stratum intermedium and extrosseous is from dental lamina, epithelial rests or basal rests of gingival epithelium. Intraosseous is more aggressive. On histopathological examination reveals polyhedral neoplastic cells, with abundant eosinophilic finely granular cytoplasm with nuclear pleomorphism and prominent nucleoli. Most of the cells are arranged in anastomosing sheet like masses. An extracellular eosinophilic homogenous material staining like amyloid is characteristic of this tumor. The Presence of calcification is another defining feature of Pindborg tumor. The extent and shape of calcification can vary from minimal small round concretions to Liesegang rings and large aggregates. According to Krolls and Pindborg, the presence or absence of calcification in CEOT has prognostic implications. A lack of calcification indicates less tumor differentiation and has more chance of recurrence. He also reported recurrence after removal in a CEOT that had minimal calcifications.
Conclusion
The present case showed characteristic histopathological features of CEOT, such as fibro vascular connective tissue and islands of epithelial cells. Areas of extensive deposition of homogenous eosinophilic material resembling amyloid are present all over the tissue. Individual cells are hyperchromatic and loosely cohesive at some areas. Connective tissue contains irregularly arranged collagen fibres with spindle shaped fibroblasts. Multiple haemorrhagic sites are also seen. The treatment will depend on multiple factors such as size and location of the tumor, patient’s general condition, histopathological findings. Small intrabony lesions are treated by enucleation and curettage, whereas large tumors require aggressive approach, either by hemimandibulectomy or hemimaxillectomy. The recurrence rate is 10%–20% was reported hence, periodic follow‑up is essential to prevent further recurrence.
References
-
Santosh K, Gowri S, Dinakar J (2016) Pindborg tumor. Contemp Clin Dent 7(1): 95-97.
-
Chatterjee RP, Gayen S, Kundu S, Chattaraj M, Pal M, et al. (2017) A unique case of clear cell variant of calcifying epithelialodontogenic tumor involving the maxilla. Dent Res J 14(4): 293-296.
-
Gotmare SS, Pereira T, Shetty S, Kesarkar KS (2018) Pindborgtumor: Pathology with special stains. Indian J Pathol Microbiol 61(2): 239-241.
-
Kaushal S, Mathur SR, Vijay M, Rustagi A (2012) Calcifying epithelial odontogenic tumor (Pindborg tumor) withoutcalcification: A rare entity. J Oral Maxillofac Pathol 16(1): 110-112.
-
Deboni MC, Naclério Homem MG, Pinto JDS, Traina AA, Cavalcanti MG (2006) Clinical, radiological and histological features of calcifying epithelial odontogenic tumor: Case report. Braz Dent J 17(2): 171.
-
Afroz N, Jain A, Maheshwari V, Ahmad SS (2013) Non- calcifying variant of calcifying epithelial odontogenic tumor with clear cells-first case report of an extraosseous (Peripheral) presentation. Eur J Gen Dent 2(1): 80-82.
-
Sahni P, Nayak MT, Singhvi A, Sharma J (2012) Clear cell calcifying epithelial odontogenic (Pindborg) tumor involving the maxillary sinus: A case report and review of literature. J Oral Maxillofac Pathol 16(3): 454-459.
-
Wadhwan V, Sharma P, Bansal V (2015) A rare case of hybrid odontogenic tumor: Calcifying epithelial odontogenic tumor combined with ameloblastoma. J Oral Maxillofac Pathol 19(2): 268.
-
Singh N, Sahai S, Singh S, Singh S (2011) Calcifying epithelial odontogenic tumor (Pindborg tumor). Natl J Maxillofac Surg 2(2): 225-227.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells