How to Manage a Disaster: Clinical Case
Introduction: Early and correct management of dental trauma has overwhelming importance on the survival of the tooth in the arch as well as the social life and comfort of the human individual. Methods: This article presents the case of a young patient who suffered a dental trauma 9 years ago, and who was not treated properly, leading to chronic infection in the affected tooth’ periapical area. The double fracture of the tooth led to the development of chronic apical periodontitis with subsequent inflammatory root resorption, discomfort and pain. The tooth was treated 9 years later employing orthograde and surgical intervention. Discussion: The healing process goes unexpectedly well, presenting no clinical signs 1 year after the intervention with the preservation of the tooth on the arch and lack of clinical symptoms. Conclusion: Early diagnosis and adequate treatments manage to preserve essential teeth on the arch in most of the trauma cases. The lack of communication with the patient as well as delayed treatments exposes the patient to unwanted complications which have effect on the patient’s comfort and social life.
Introduction
Dental traumas are always complicated cases that raise many questions in many aspects. These aspects are mainly related to the restorability of the tooth and the survival of the tooth on the arch, but also to the therapy that must be applied on a case-by-case basis. This therapy is influenced by the patient’s age, the type of trauma, the complications of the trauma, and in the case of fractures it depends a lot on the location and direction of the fracture line. This case presents a double fracture located in the apical third of the root with the loss of the coronal aspect of the left upper central, in a relatively young patient, as a result of a trauma suffered 9 years ago and was never treated properly.
Case Presentation
A 31-years-old male was referred to our practice after had his post and crown on upper left central (tooth 21-FDI) decemented. Besides the decemented restoration, the patient complained of the long-lasting presence of a draining sinus tract and tenderness to pressure in the sulcus related to tooth 21(FDI). During the examination, a draining sinus tract was evident in the buccal aspect of the gum corresponding with the apex of 21, a sign of a long-standing chronic periapical lesion. No swelling was evident in the sulcus, while a serous- citrine-like liquid was draining from the sinus tract, on pressure. The remaining tooth structure was limited to a retained root with an incomplete ferrule closure. Percussion testing elicited normal response but the area of the apex was tender to pressure applied horizontally. The root canal was free of debris, while the porcelain bonded crown was still attached to the cast metal post. The radiographic periapical image revealed a short root along with a large circumlucent lesion related with the apex of tooth 21(FDI), with widened periodontal ligament and inflammatory root resorption which had a strange oblique trajectory going disto-mesially in an apico-coronal direction on the mesial aspect of the root (Figure 1A). No pathologic mobility was recorded while there was no evident pathologic probing depth, nor bleeding on probing. Upon review of the medical history, no systemic disease was declared, the patient denying taking any medications. The diagnosis of apical periodontitis was established.
The patient mentioned a history of trauma that affected the tooth 9 years ago, which led to the complete loss of the coronal aspect of the tooth. Following it, the patient was assessed at the hospital by oral surgeons who mentioned to him that there is no point in doing any apical surgery and referred him back to his general dentist, who provided the tooth with a root filling and subsequent post and crown restoration. Ever since then his tooth started developing a sinus tract which was draining continuously. The patient wasn’t aware of any diagnosis made on his tooth by the dentist or the oral surgeon 9 years ago, his concern being the aesthetic detriment of his de-cemented post and crown, given that he was supposed to attend a wedding that weekend. He asked for one session of permanent treatment. The patient consented to the treatment and the treatment commenced.
No local anesthesia was provided, thus helping to preserve the tactile sensations during the treatment, allowing the clinician to be very aware when irrigating or shaping the root canal, to any sensitivity reported by the patient. The tooth was isolated under a rubber dam (Coltene Whaledent, Altstaten, Switzerland) and liquid dam (Cerkamed, Stalowa Wola, Poland) to keep the rubber sheet in place. No root filling or its remnant nor cement was evident in the canal. It is possible that the only root filling the tooth received was the post and the cement. The lack of cement in the canal facilitated access, inspection and the subsequent root canal treatment. The root was examined under loupe magnification, searching for possible perforations or crack lines, finding nothing abnormal. No bleeding was recorded during the procedure. A “zero” apex locator (NSK iPex II, Kanuma, Tochigi, Japan) reading was obtained at 11mm depth. The working length was deemed to be 0.5mm shorter than the diagnostic length. The canal was debrided with size 40-90 K-files (Mani Inc., Utsunomiya, Tochigi, Japan) using the brushing movement till the canal looked clean under magnification. Irrigation using 5,25% NaOCl (sodium hypochlorite) (Cerkamed, Stalowa Wola, Poland) and 17% EDTA (ethylene-diamine-tetra-acetic acid) (Meta-Biomed Co Ltd., Chungbuk, Korea) was carried out under manual-dynamic agitation for 5 minutes, using a cone(Sendoline, Taby, Sweden) fitted to working length -2mm to avoid irrigant extrusion. The canal was shaped and finished using manual k-file to Maximum Apical File (MAF) 90/0.02, and subsequently dried using paper points (Sendoline, Taby, Sweden) size 2, inserted reversely into the canal. A piece of collagen (Gelatamp, Coltene-Whaledent, Altstaten, Switzerland) was placed apically to prevent the overextension of the MTA apical plug apically. MTA (Angelus, Londrina, Brasil) was placed using a single-use MTA carrier (IM3, Duleek, Ireland). A control PeriApical (PA) x-ray was taken (Figure 1B). The radiograph confirms working length and the presence of the apical plug. Additional MTA was placed to achieve an apical plug of 2-3mm. Since the metal post ended approximately at the level of the fracture, it was shortened with 2-3 mm so the root can accommodate the MTA plug (Figure 1C). Cement remnants were also removed from the post’s surface. After 45 minutes of waiting for MTA setting the post and crown were tried in, confirming a good occlusion and marginal fit. The post and crown were recemented with Riva Luting Plus cement (SDI, Bayswater, Australia). The excess cement was cleared and flossed through contact points. The occlusion was checked again in protrusive, retrusive and lateral movements. A postoperative radiograph was taken and looks satisfactory (Figure 1C). The patient attended his recall appointment 3 months later, during which a new radiographic examination was carried out (Figure 1D). On the x-ray, due to the subsiding radiolucency, the broken apical could be located along with the oblique trajectory of the fracture line. Considering that the apical fragment was necrotic, the patient was referred to an oral surgeon to have the root fragment removed surgically. On the 1-year follow-up radiograph, there is evident healing present at the site of the former apical fragment (Figure 1E). Clinically, the sinus tract healed and there was no more tenderness reported to pressure on the buccal aspect of the alveolar bone related to the root of 21. The stability of the tooth was preserved, no pathologic mobility was recorded.
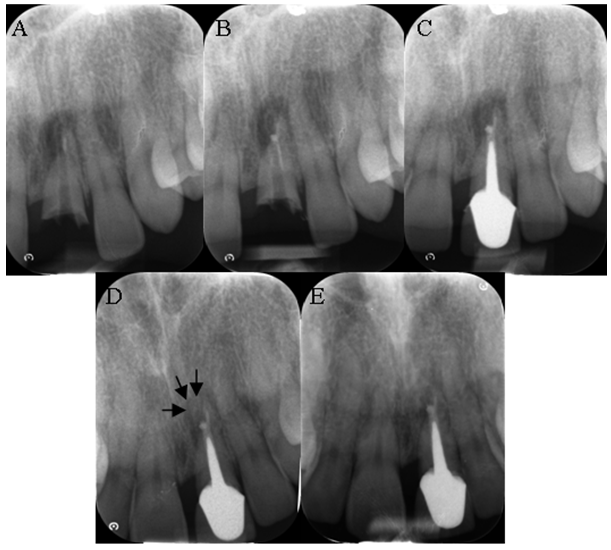
Figure 1A-E: A: Initial Radiograph; B: MTA apical plug; C: Post OP radiograph; D: 3 months follow-up radiograph, arrows pointing to the broken apical fragment; E: 1 year follow-up radiograph after the apicoectomy.
Discussion
As shown previously, fractures are areas of kinetic energy disruption that spares the periodontal support tissue (especially the alveolar bone) from the harmful mechanical shock [1]. As we know, luxations require stricter trauma management measures, which begin with the repositioning and suture of the dilacerated soft tissues [2], the repositioning of the tooth, its elastic immobilization [2, 3, 4, 5], and the subsequent complications that vary from tooth discoloration to canal obliteration or root resorption. Therefore, luxations have a poorer prognosis than fractures [2, 6].
Of all the types of root fractures, the present case is not a happy one. The fracture of the apical third generally does not pose problems for the survival of the tooth compared to the fracture of the coronal or middle third. In this case, we have a double fracture, complete crown fracture accompanied by root fracture in the apical third. Sometimes the apical fragment remains vital, and the coronary one becomes necrotic shortly after trauma [7]. Well, it is not the case of the present tooth which needed apicoectomy, and even if we have no information about the onset of the necrosis, it is assumable that it happened soon after the trauma, given the double fracture. There was no luxation involved in this case, so the recovery of the tooth was quick and without further complications, the tooth being restored shortly after the initial trauma and root canal treatment. The healing was by the interposition of periodontal ligament alone. The non-healing inflammatory process was perpetuated by the necrotic apical fragment and the leaking coronal restoration. An ameliorating factor of the present pathology could be the sinus tract and the possible coronary percolation that allowed the trans-dental and trans-osseous drainage of the periapical secretions.
Tooth’s restorability and long term prognosis are arguable. The crown-root ratio of approximately 1 is unfavorable. Another arguable aspect is the thickness of the MTA plug which, being not more than 2-3mm is prone to bacterial penetration and subsequent flare-ups [8]. Although the 12 months recall x-ray shows subsiding radiolucency, on the long term the prognosis is guarded. The way the fracture line goes obliquely doesn’t favor the prognosis either, exposing a big chunk of the apical plug which couldn’t be compacted properly apically. Moreover, this oblique orientation of the fracture line further prevented the clinician to provide a thorough mechanical debriding of the most apical section of the coronal fragment of the root. A better outcome could have been achieved if calcium hydroxide was used as an inter-appointment medicament to reduce the pH of the area to ensure a better action of MTA and to ensure a complete resolution of the apical periodontitis, but the patient’s hasty to have a functional tooth for that weekend prevented the clinician to phase the treatment. Sometimes the calcium hydroxide prolonged application in the canal and the fracture site, manages to close the gap between the two broken fragments if the gap between them is not too wide. MTA was reported to be successfully used for this purpose too [9, 10]. There were reports of preserved vitality in similar cases, where the gap between the fragments was less than 1mm and the tooth healed by means of hard tissue deposition [11] or there was a closure of the gap by means of a calcific barrier that allowed the root canal treatment to the level of the barrier without its overextension to the apical fragment [7]. Unfortunately, there are no details about the post-traumatic onset of the necrosis nor could the patient remember if there were any attempts to reposition and splint the broken coronal fragment. Even if the fragment had been repositioned, the long term prognosis of these teeth is poor due to the increased risk of new luxation or injury [11, 12].
Conclusion
The management of dental traumas has been and remains a delicate aspect of modern dentistry, on which the very survival of the tooth depends, on the medium and long term. This aspect is closely related to the patient’s inner comfort, self-esteem and social life, the loss of a tooth affecting all these aspects related to the social integration of the individual. Proper early treatment is essential in many ways, and this treatment must take into account the patient’s age and priorities. The patient must be informed about the treatment options and most especially, of the immediate or late complications of the traumas. His decision on what treatment to opt for has to be fully informed. In this case, the patient was poorly informed about his condition, not being aware of the broken apical fragment, not being warned about the perpetrated apical infection maintained by the fragment, and the inflammatory root resorption caused by the infection. All these aspects unjustifiably impeded on the patient’s well-being and comfort.
References
-
Andreasen JO (1970) Etiology and pathogenesis of traumatic dental injuries. A clinical study of 1,298 cases. Scand J Dent Res 78(1-4): 329-342.
-
Andreasen JO (1994) Textbook and color atlas of traumatic injuries to the teeth. 3rd (Edn.), Copenhagen: Munksgaard.
-
Oikarinen K (1990) Tooth splinting: a review of the literature and consideration of the versatility of a wire- composite splint. Endod Dent Traumatol 6(6): 237-250.
-
Oikarinen K, Andreasen JO, Andreasen FM (1992) Rigidity of various fixation methods used as dental splints. Endod Dent Traumatol 8(3): 113-119.
-
McDonald N, Strassler HE (1999) Evaluation for tooth stabilization and treatment of traumatized teeth. Dent Clin North Am 43(1): 135-149.
-
Robertson A, Andreasen FM, Andreasen JO, Noren JG (2000) Longterm prognosis of crown-fractured permanent incisors. The effect of stage of root development and associated luxation injury. Int J Paed Dent 10(3): 191-199.
-
Cvek M, Mejare I, Andreasen JO (2004) Conservative endodontic treatment of teeth fractured in the middle or apical part of the root. Dent Traumatol 20(5): 261-269.
-
Al Kahtani A, Shostad S, Schifferle R, Bhambhani S (2005) In-vitro evaluation of microleakage of an orthograde apical plug of mineral trioxide aggregate in permanent teeth with simulated immature apices. JOE 31(2): 117-
-
Cohen S, Hargreaves KM (2006) Pathways of the pulp. 9th (Edn.), St. Louis: Elsevier Mosby.
-
Bramante CM, Menezes R, Moraes IG, Bernardinelli N, Garcia RB, et al. (2006) Use of MTA and intracanal post reinforcement in a horizontally fractured tooth: a case report. Dent Traumatol 22(5): 275-278.
-
Andreasen JO, Andreasen FM, Mejare I, Cvek M (2004) Healing of 400 intra-alveolar root fractures. 1. Effect of pre-injury and injury factors such as sex, age, stage of root development, fracture type, location of fracture and severity of dislocation. Dent Traumatol 20(4): 192-202.
-
Welbury R, Kinirons MJ, Day P, Humphreys K, Gregg TA (2002) Outcomes for root-fractured permanent incisors: a retrospective study. Pediatr Dent 24(2): 98-102.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells