PEEK Biomaterial Use for Chairside CAD/CAM Dental Restorations: Bridging the Gap to Future
Background: Advanced computer-aided design and computer-aided manufacturing (CAD-CAM) technology led to the introduction of an increasing number of machinable materials suitable for dental prostheses. One of these materials is polyetheretherketone (PEEK), a high performance polymer recently used in dentistry with favorable physical, mechanical and chemical properties. Purpose: The aim of this study was to review the current published literature on the use of PEEK for the fabrication of dental prostheses with CAD-CAM techniques. Methods: Electronic database searches were performed using the terms “PEEK”, “CAD-CAM”, “dental”, “dentistry” to identify studies related to the use of PEEK for the fabrication of CAD-CAM prostheses. Results: A great number of in vitro studies are available in the current literature pointing out the noticeable properties of PEEK. The use of PEEK has been recommended for a wide range of CAD-CAM fabricated fixed and removable dental prostheses, occlusal splints, intra-radicular posts, implant abutments, customized healing abutments, space maintainers for pediatric dentistry, orthodontic appliances and provisional restorations. However, only a few clinical studies were identified. Conclusions: PEEK could be considered as a viable alternative for CAD-CAM dental appliances to well-established dental materials. Due to the scarcity of clinical data, clinical trials are needed to assess the longterm performance of PEEK prostheses
Introduction
Digital technologies and new materials are becoming popular, getting better and changing the way to do diagnosis and therapy in dentistry [1]. New digital technologies are taking hold in diagnosis, therapy and in dental laboratories. The digital world can help dentist in diagnosis and therapy through the acquisition of radiographic images (CBCT) or scanners which allow the creation of 3D digital models – about therapy thanks to dental CAD CAM system. It consists of design devices through a dedicated software CAD and then realize devices through CAM system [2].
The first chairside CAD/CAM produced inlay was made in 1985 using a ceramic block comprising fine grain feldspathic ceramic (Vita Mark I, Vita Zahnfabrik) [3]. Since the 80’s, different systems have been developed, such as known CEREC. Systems have evolved through a series of software and hardware. The current systems offer a three- dimensional (3-D) design program and can fabricate inlays, onlays, veneers, crowns, as well as three unit bridges from a variety of biomaterials [4].
The wide use of chairside CAD/CAM restorations has increased the diversity of the restorative material. PEEK is a high-performance thermoplastic polymer with high strength-to weight ratio and corrosion resistance that makes it suitable as a selectable material to replace metal. PEEK is a semi-crystalline polymer commercialized from 1978 and composed by repeating units of three phenyl rings, two ester groups and one keto group [5]. Considering PEEK original development (Victrex plc, Lancashire, UK), the fabrication process results in a number of properties including chemical stability, biostability, biocompatibility, creep and wear resistance, and superior mechanical behavior. These properties allow compatibility with medical diagnostic imaging, extending its use from industrial applications to those in the fields of dentistry [6].
For Dentistry, PEEK’s elastic modulus properties displaying a mechanical behavior more closely related to bone and shock absorbing properties drive the rising enthusiasm, enabling a uniform transfer of stress to the underlying bone and reducing potential deleterious effects of active stress points in the mouth [7]. This aspect is particularly important for patients with bruxing habits (involuntary gnashing, grinding or clenching of teeth associated with forceful lateral or protrusive jaw movements). Moreover, PEEK’s shock absorbing and biocompatibility features and the possibility of incorporating the polymer in computer-aided design and computer-aided manufacturing (CAD/CAM) workflows supported its use in the production of a series of devices including: dental implants, abutments, healing caps, crowns, removable prosthesis, fixed partial or full-arch dentures [8].
The historical perspective of implant framework materials includes the evolution from cast noble (gold, silver, etc) or base metal alloys (nickel and chromium) to the modern milled titanium and zirconium frameworks, the latter providing high biocompatibility, corrosion resistance, and the possibility of computer assisted-design/ computed assisted-manufacture (CAD/CAM), an important improvement to achieve a better fit between framework and dental implants [9]. Nevertheless, the high stiffness of these frameworks measured by the flexural strength (titanium: 434 MPa; zirconia: 900-1100 MPa) can be considered a potential disadvantage in shock absorption behavior of the prosthesis [10].
Over the last decades, PEEK has seen extensive use in highly demanding industrial (aerospace, automotive, oil and gas, electronic) and medical applications [11]. Specifically in the field of dentistry, PEEK has been used over the last decade in healing caps and temporary abutments. Due to its proven biocompatible nature and its shock absorbing characteristics, while maintaining the possibility of CAD/ CAM manufacture, such a material could be interesting for use in full-arch restorations as a nonmetal alternative [12]. Nevertheless, proof on its long-term outcome in implant-supported fixed rehabilitations is lacking, making it necessary to evaluate the outcome of implant supported fixed prosthetic rehabilitations using PEEK material.
In dentistry as in other dental specialties, digital technologies are replacing non-digital/analog technologies for creating prostheses and developing diagnostic scenarios toward the improvement of patient care. This article will review the CAD/CAM, and its potential to become the dominant means of care in dentistry was the aim of the current work with concentration to supply the dental community the feasibility of CAD/CAM to develop new PEEK-integrated restoration and validated CAD/CAM, which provides a foundation for future clinical applications, thus opening up many new possibilities.
Structure, Properties, Advantages, and Disadvantages of PEEK Polymer
PEEK consists of a high-performance polymer from the polyaryletherketone (PAEK) family. PEEK is a thermoplastic polymer that is typically used as a metal replacement, owing to its strength to weight ratio and corrosion resistance [13]. PEEK was originally developed in the United Kingdom in 1978 (ICI—now as Victrex plc) and requires a particular polymerization process, which enables the control of the length of the resulting polymer chains [14]. This polymer versatility allows the offering of a range of processing options and an array of formulations, ranging from unfilled grades with varying molecular weights, to image contrast, colored and carbon fiber-reinforced grades [5]. PEEK is a polycyclic, aromatic, thermoplastic polymer that is semi-crystalline and has a linear structure. This material is obtained as a result of the binding of ketone and ether functional groups between aryl rings and is an element which is tan-colored in its pure form (3) (Figure 1).
The Properties of PEEK Material
This material, which can be produced by casting under heat and pressure with the lost wax technique and by CAD-Cam technology. It has several positive properties like resistance to hydrolysis, has superior mechanical properties and is resistant to high temperatures. When PEEK material and components are examined, no evidence has been shown of cytotoxicity, mutagenicity, carcinogenicity or immunogenicity in the toxic form. It is a biologically inert material. It shows resistance to deterioration during various sterilization procedures. Melting point is >280°C. Therefore, it can be processed with hot sterilization methods. It shows high resistance to chemical wear. It can be modified together with various materials. The most important property of this material is that it has a low elasticity modulus (close to the elasticity modulus of bone). When an increase in the elasticity modulus is desired, the PEEK elasticity modulus can be brought to high levels with the addition of carbon fibers [15]. It is a very light material with a low density (1.32g / cm3). It allows magnetic resonance imaging (MRI). Radiation heat does not cause disintegration. Laboratory stages are simple. It is a low-cost material that can be easily prepared within the mouth [16].
PEEK is a sub family of the poly-aryl-ether-ketone (PAEK). It is a high performance thermoplastic linear homopolymer composed of similar repeating units. It imparts its stiffness from aromatic benzene rings and its ability to rotate in an axial direction thanks to ether oxygen bonds. This material can be sterilized and irradiated due to its stability at temperatures above 300°C [17]. With stiffness double that of lithium disilicate and similar to cortical bone, this material can alleviate excessive stress being directed on implants and provide lesser stress shielding. For this reason PEEK was recently described as a framework material over implants and teeth [18].
Since its introduction to the market in April 1998, PEEK-OPTIMA™ has gained increasing acceptance as a high performance implant material. Significant advantages over metals include: the elimination of imaging artefacts, the ability to view tissue/bone growth and repair using x-rays (which can often be obscured with metal parts) and, more generally in this and other applications, the avoidance of allergic tissue reaction to metallic ions. In diagnostics, as well as in postoperative inspection, it is increasingly important to monitor the healing process by modern imaging technologies, like X-ray, CT or MRI. In an X-ray image, the intensive shadow produced by a metal implant overlaps the area of importance for the surgeon, making it difficult, or even impossible, to adequately inspect. This is similar in CT-imaging where metal implants create artefacts. PEEK-OPTIMA™ LT polymer is transparent to X-rays and there are no artefacts created in CT images. Because plastics are non-magnetic MRI technologies still can be used with patients that have received a plastic implant [19].
As for allergic reactions to nickel and other metal ions, owing to the high purity of PEEK-OPTIMA™ LT polymer the total amount of metallic ions is very low (ppm and ppb levels) so no allergic reactions are to be expected. Surface modification technologies can be more easily applied to organic surfaces like PEEK-OPTIMA™ LT polymer than to metal surfaces, which offers additional benefits for components with direct blood contact. Plastic Processing technology and suitable joining technology as well as more freedom in design and shape offer additional benefits. PEEK- OPTIMA™ is a polyaromatic semicrystalline thermoplastic (30-35% crystallinity typically) with a melting temperature of ~343°C, a crystallisation peak of ~160°C and a glass transition temperature of ~145°C. It can be readily melt processed by injection moulding and extrusion using conventional methods. Three natural (unfilled) grades are available as high, medium and low viscosity variants. All are based on the same basic formula (-C6H4-O-C6H4-O-C6H4- CO-)n. Natural, unfilled PEEK-OPTIMA™ is characterised by its high strength, its extreme resistance to hydrolysis and its resistance to the affects of ionising radiation [19]. PEEK can be repeatedly sterilised using conventional steam, gamma and ethylene oxide without significant deterioration [20].
The application of PEEK in implant dentistry
It is thought that PEEK material could be an alternative to conventional materials in implantology. PEEK has become a material that is used in implant, abutment and prosthesis production. Under the headings of healing from PEEK material in implantology, it is also possible to manufacture screws providing bonding with implant abutment [21].
PEEK Implants
Metallic implant materials have some disadvantages such as bone resorption and subsequent implant loss, disintegration under radiation light, over-sensitivity reactions, allergic potential and surface deterioration related to peri-implantitis. The negative aspects of metallic implant materials could be overcome with the use of an implant produced from a non-metallic material such as PEEK [22]. In contrast to titanium has a high elastic modulus, shock absorbency is not shown during chewing actions. It has been suggested that as PEEK material has an elasticity modulus close to that of bone, the stresses occurring on the bone are reduced with the absorption of forces. Transfer onto the bone of the loading on a rigid structure implant leads to resorption in the bone. Due to PEEK shock absorbing property, there is the advantage of bone protection. When current research is examined, it can be seen that there are still no long-term studies of the efficacy of this material on patients. Therefore, PEEK implants are not widely used clinically [23].
titanium and alloys have several disadvantages such as corrosion and causing over-sensitivity reactions, they are the most frequently selected materials in the production of implants and abutments and have been accepted as the gold standard [24]. However, sometimes in cases where aesthetics are a priority, satisfactory results cannot be obtained. It has been suggested that PEEK can promote the bone remodeling process. Therefore, it has been reported that this material could be a suitable alternative to titanium in abutment production (Figures 2a & b) [23].
PEEK Implant Abutments
The abutment has to be a material that meets the mechanical, biological and aesthetic expectations. Various materials such as titanium, gold, zirconium and ceramics are made use of in the production of abutments. Although
![Figure 2: A) A new transitional abutment for immediate aesthetics and function and B) Use of high performance polymers as dental implant abutments and frameworks: a case series report [25].](/fulltextimages/7404/fig_2.png)
Considering PEEK’s shock absorbing properties, the authors attempted to apply the same protocol to more challenging rehabilitations: All-on-4® Hybrid rehabilitations [26]. These rehabilitations imply the use of zygomatic implants (with 38-50 mm of length) that are longer compared to standard implants, only using zygomatic bone anchorage, and inserted with a mesial tilting, implying an increased lever arm that represents more challenging biomechanical conditions. This is reflected in the incidence of mechanical complications occurred in these rehabilitations that can reach as high as 47.5% (including 27.5% of prosthesis fracture) considering a one year follow-up study [26].
A representative clinical case is illustrated in Figure 3.The results of three of 10 cases that reached 6 months of follow-up of an ongoing prospective study registered the absence of mechanical complications, adding to the 100% cumulative implant survival rate and absence of biological complications. These results, despite the short term follow- up, are positive and represent a potential broader scope of PEEK application to implant-supported fixed restorations [27].
![Figure 3: The results of three of 10 cases that reached 6 months of follow-up of an ongoing prospective study registered the absence of mechanical complications, adding to the 100% cumulative implant survival rate and absence of biological complications. These results, despite the short term follow- up, are positive and represent a potential broader scope of PEEK application to implant-supported fixed restorations [27].](/fulltextimages/7404/fig_3.png)
Figure 3: A) Poly-ether-ether-ketone (PEEK) disks (Juvora Ltd); B) PEEK infrastructure milled through Computer Assisted Design / Computer Assisted Manufacture (CAD/CAM) workflow; C) Finished PEEK - Polymethacrylate (PMA) - Lithium Disilicate (LD) hybrid prosthesis; D) Finished PEEK-PMA-LD hybrid prosthesis in the mouth; E) Orthopantomography of the PEEK-PMA-LD hybrid prosthesis with one year follow-up. Notice the prosthesis is supported by two anterior standard implants and two posterior zygomatic implants (All-on-4® Hybrid); F) Patient smiling with the PEEK-PMA-LD hybrid prosthesis with one year follow-up [27].
As limitations, the outcome of PEEK polymers when applied to implant-supported restorations benefit from a precise CAD/CAM planning and surface preparation in order to create the necessary physical and chemical retention to avoid veneer adhesion issues. As suggestion for future developments, PEEK polymers could benefit from a broader scope of lighter colors for aesthetic reasons. Overall, the characteristics of the PEEK polymer seem to benefit the implant biological outcome and may represent a valid alternative for the use of metal in prosthetic infra-structures, exhibiting a closer behavior to natural dentition from a biomechanical point of view [27].
Removable dental prostheses (RDPs)
CAD-CAM techniques can be also used to fabricate RDP frameworks. A previous clinical report has suggested PEEK frameworks combined with acrylic resin denture teeth and heat-cured acrylic resin denture bases as an alternative to conventional Co-Cr frameworks [28]. PEEK presents favorable properties such as excellent biocompatility, good mechanical properties, good thermal and chemical resistance, white color and low specific weight that permit the fabrication of lighter metal-free RPDs eliminating the esthetically unacceptable display of metal claps and the risk for metallic taste and allergies of conventional RDP metal frameworks [29]. Another study described the use of milled PEEK frameworks for the fabrication of a removable maxillary obturator prosthesis [30]. Both studies reported high patient satisfaction with regard to esthetics, retention and comfort [30]. Due to its high elasticity, PEEK could reduce stresses and distal torque on the abutment teeth during function [29].
Occlusal Splints, Intra-Radicular Posts and Provisional Restorations
The use of PEEK was additionally recommended for CAD-CAM fabricated occlusal splints. An in vitro study found lower loss of volume and change in roughness for PEEK occlusal splints after chewing simulation compared to other CAD-CAM materials such as vinyl acetate (EVA), polymethyl methacrylate (PMMA), polycarbonate (PC), and polyethyleneterephthalate (PETG) [31].
It was also claimed that milled PEEK intraradicular posts could be an alternative to glass-fiber and cast-metal posts. According to an in vitro study, PEEK posts presented higher tensile bond strength than metal and glass-fiber posts when used with the appropriate surface treatment and adhesive system [32]. Previous studies evaluated the performance of PEEK for CADCAM fabricated implant abutments, customized healing abutments and provisional crowns [33, 34, 35].
A finite element analysis comparing PEEK and zirconia customized abutments found higher stress values in restorative crowns for PEEK abutments [33]. A randomized clinical trial evaluated the use of CAD-CAM fabricated customized healing abutments and standard healing caps placed at the surgical stage for the creation of the desired emergence profile. After a healing period of 1–3 months PEEK customized healing abutments created a natural gingival architecture and required less prosthetic steps for the formation of the emergence profile compared to the use of standard healing caps [34].
Last but not least, Abdullah et al. in an in vitro study compared CAD-CAM provisional crowns with direct provisional crowns. The materials used were VITA CAD Temp, PEEK, Telio CAD-Temp, and Protemp 4. Based on the results of this study, digitally produced PEEK provisional restorations demonstrated better fit and fracture strength than conventional provisional crowns [35].
CAD-CAM of PEEK for Application to Removable Pediatric Space Maintainers (RSM)
The premature loss of primary teeth is a common problem in the pediatric dentistry hence, space maintainer (SM) are used for maintaining the space. The removable space maintainer (RSM) is a kind of SM that have several advantages including maintaining the proximal, distal, and mesial lengths of a space, while maintaining the vertical height, thus restoring the aesthetics of the teeth, preventing speech disorders, and eliminating habits such as unilateral chewing [36]. However, conventional RSMs incur some drawbacks [37], particularly in terms of their design and manufacture. For example, the manufacture of RSMs is complicated, because it is technically very sensitive, requires experienced technicians, and the product outcomes exhibit large individual variations. In addition, as the manufacture of RSMs features the use of curved snap rings and self-curing resin, it is difficult to ensure the precision of the snap rings within the space maintainers. During the polyreaction of the self-curing resin, shrinkage occurs [38], adversely affecting the fit between the tissue surface of the maintainer and the mucosa between the snap ring and the abutment. As a result, pediatric patients tend to adapt poorly to space maintainers. Furthermore, owing to the scarcity of artificial deciduous teeth products on the market, artificial permanent teeth products are usually modified to emulate the functionality of deciduous teeth; however, they do not accurately simulate their morphology. Hence, a precise, convenient, rapid design and manufacturing method is needed to address these problems.
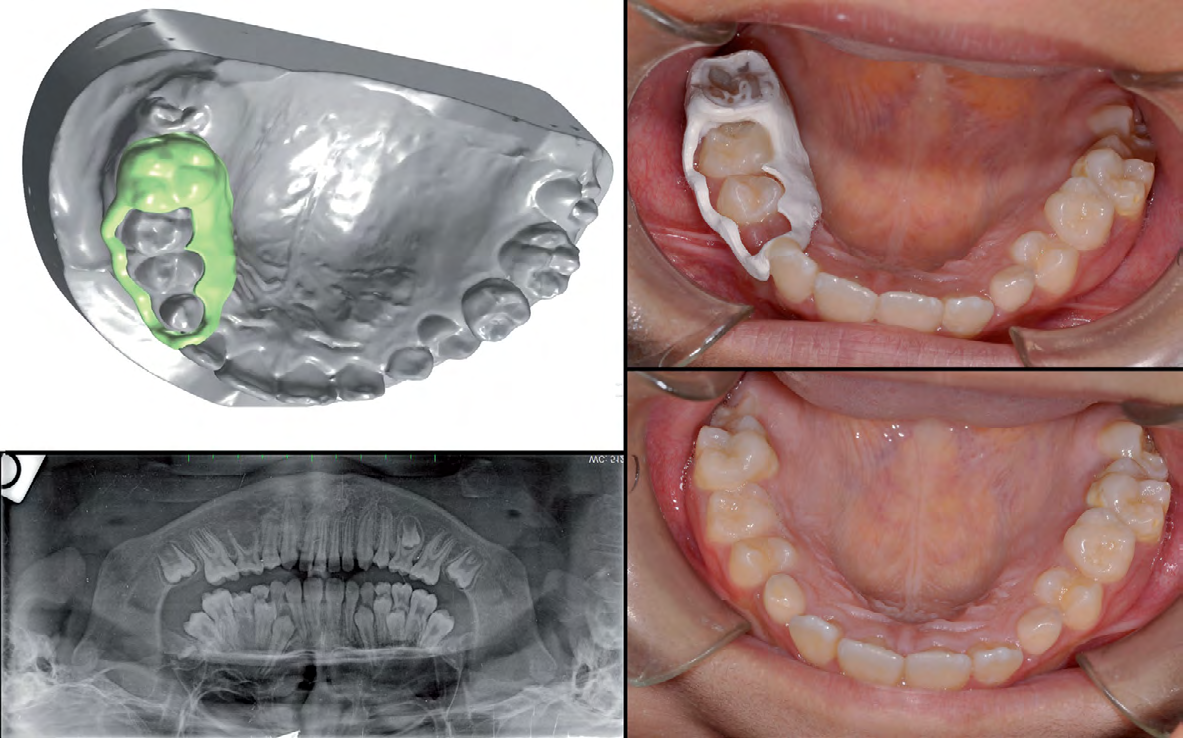
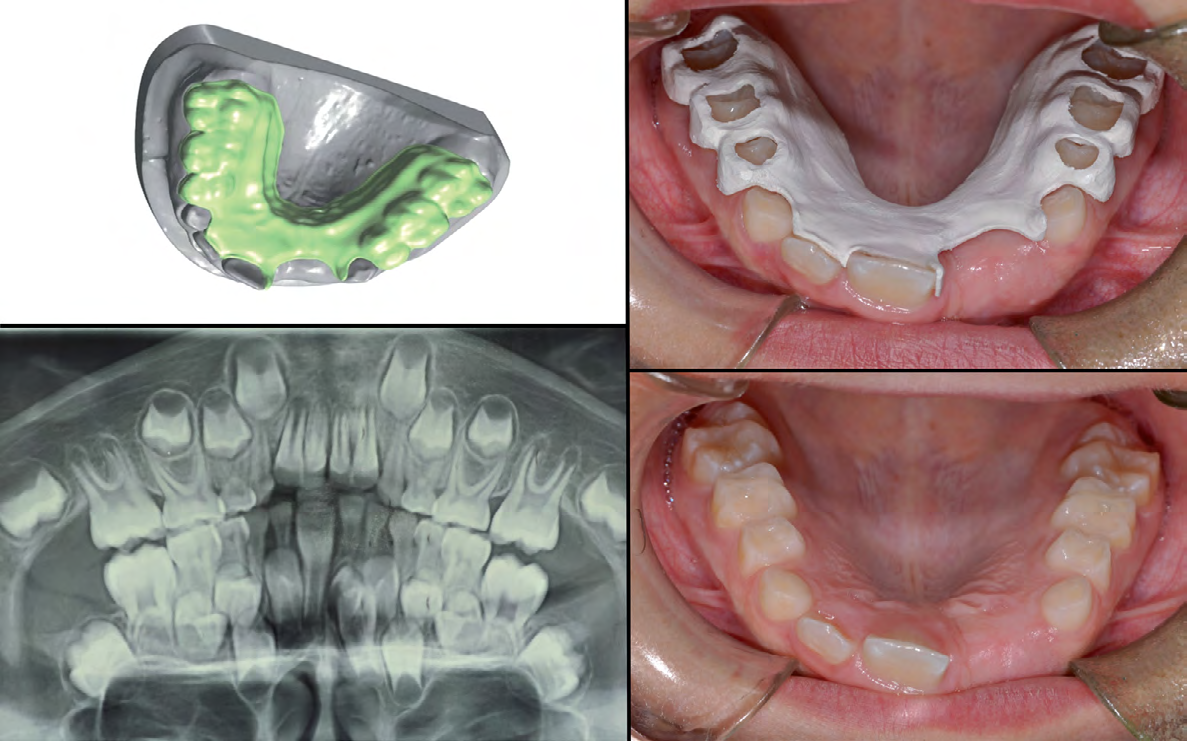
Ierardo, et al. conducted a pilot study using PEEK to fabricate an RSM with a dental CAD/CAM system, finding PEEK to be highly suitable for the fabrication of space maintainers [2]. Therefore, a study set out to investigate the application of CAD/CAM design of PEEK to the RSMs used in pediatric dentistry and to evaluate the suitability of the technique for clinical applications [39]. Example: Dental CAD software (Dental System 2017, 3Shape A/S, Denmark) and reverse engineering software (Geomagic Studio 2014, Geomagic Inc., USA) were jointly used to design all the components of the RSM. The finished set of RSM data were exported in stereolithography (STL) format (Figures 4a–h) [39].
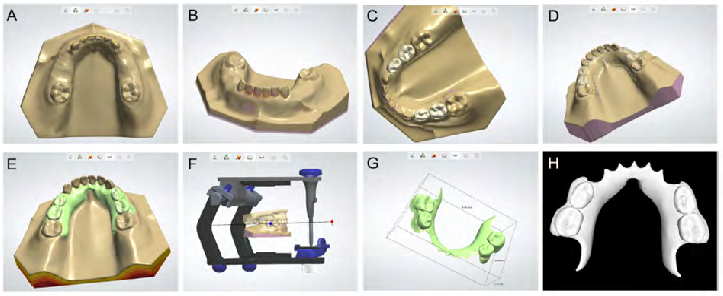
Figure 4: Digital design process for removable space maintainers; a) importing the model data; b) observing the model and filling in the voids; c) importing the artificial teeth model from the DIY deciduous teeth database into the software; d) constructing the profile of the major connector; e) composing the integrated removable space maintainer; f) using the fictitious articulator to perform occlusal adjustment; g) the final removable space maintainer; and h) the final removable space maintainer data exported in STL format.
PEEK in Orthodontics
A study has been making the orthodontic space maintainers in PEEK polymer through a digital workflow [2]. The study took place in Pediatric Dentistry Unit, Department of Oral and Maxillo-facial Sciences, “Sapienza” University of Rome, and began with the enrollment of 8-10 year old patients who needed space maintainers because of early loss of teeth for caries or extraction due to supernumerary tooth or abnormal inclination of permanent teeth. Three prototypes of orthodontic devices were made: lingual arch, band with loop and removable plate. These devices had the purpose to maintain the space in the mouth of children during the phase of dental commute helping the correct transition from deciduous teeth to permanent teeth either in patients with deciduous decayed teeth or in patients subjected to extractions in orthodontic purpose. Authors used CAD/CAM system, a technology began its dental life in 1970s [40].
The workflow has been divided into several steps [2] Step 1: After the enrollment of patients, dental precision impression were taken, models were poured and then digitalized models with a scanner in order to make a personalized appliance without standard measurements. They used an extraoral scanner (D810, 3Shape, Denmark). The scanned object was hit from all sides by light beams and then filmed with micro cameras. Since the scans are several and detected over the entire model the result was a cloud of points. The software connected the points and reconstructed a pattern of tiny polygons creating the virtual model.
Step 2: Once got virtual model, we had the model in all the screenings. Thanks to CAD (Computer Aided Design) software we designed personalized devices. The model has been archived and imported directly into 3Shape Dental Design software system using the zoom tools, rotating and panning allowed to view the model from different angles and magnifications facilitating the analysis of the model. This system allows to design devices and to determinate a lot of variables such as the material thickness, retention, undercuts, the space for the cementation, the points of support (Figure 5).
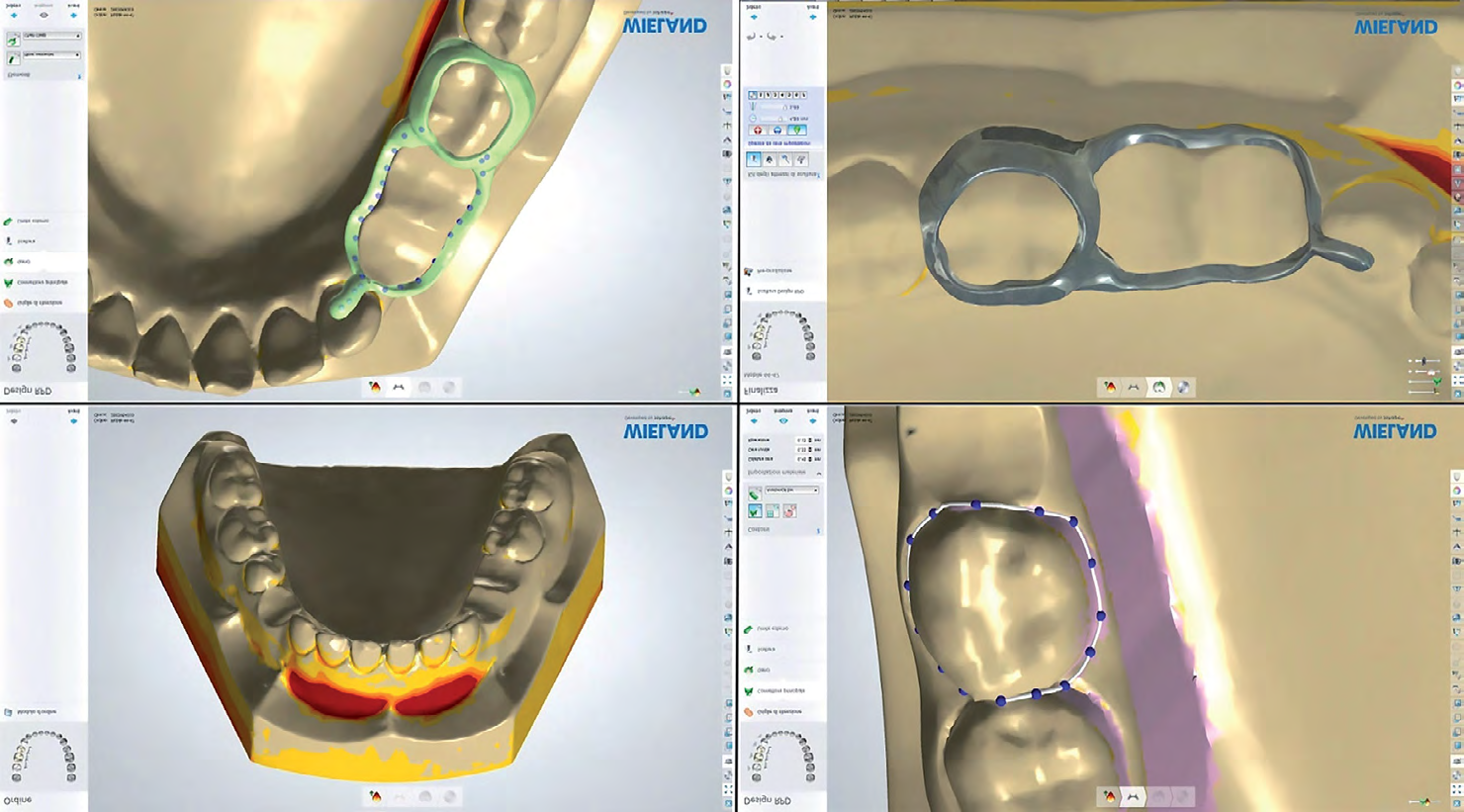
Step 3: At this point the file has been sent to the CAM and begun the construction of the building through milling Roland DWX-50 features 5-axis continuous movement, equipped with an automatic transmission of different tools. This is a manufacturing process by subtraction and thanks to these movements the block of chosen material was milled to get the form designed previously by software CAD (in about one hour). The three devices we made, were the following: lingual arch, band with loop and removable plate. The first patient was 8-year old child who needed a space maintainers to keep the space in the mandible to allow a proper eruption of the canines and premolar teeth.
The workflow allowed us to get a peek polymer 1.3mm thick lingual arch, in about one hour, which could get in touch with facial lingual. The device was also compose by two orthodontic bands cemented on the first lower molars (Figure 6).
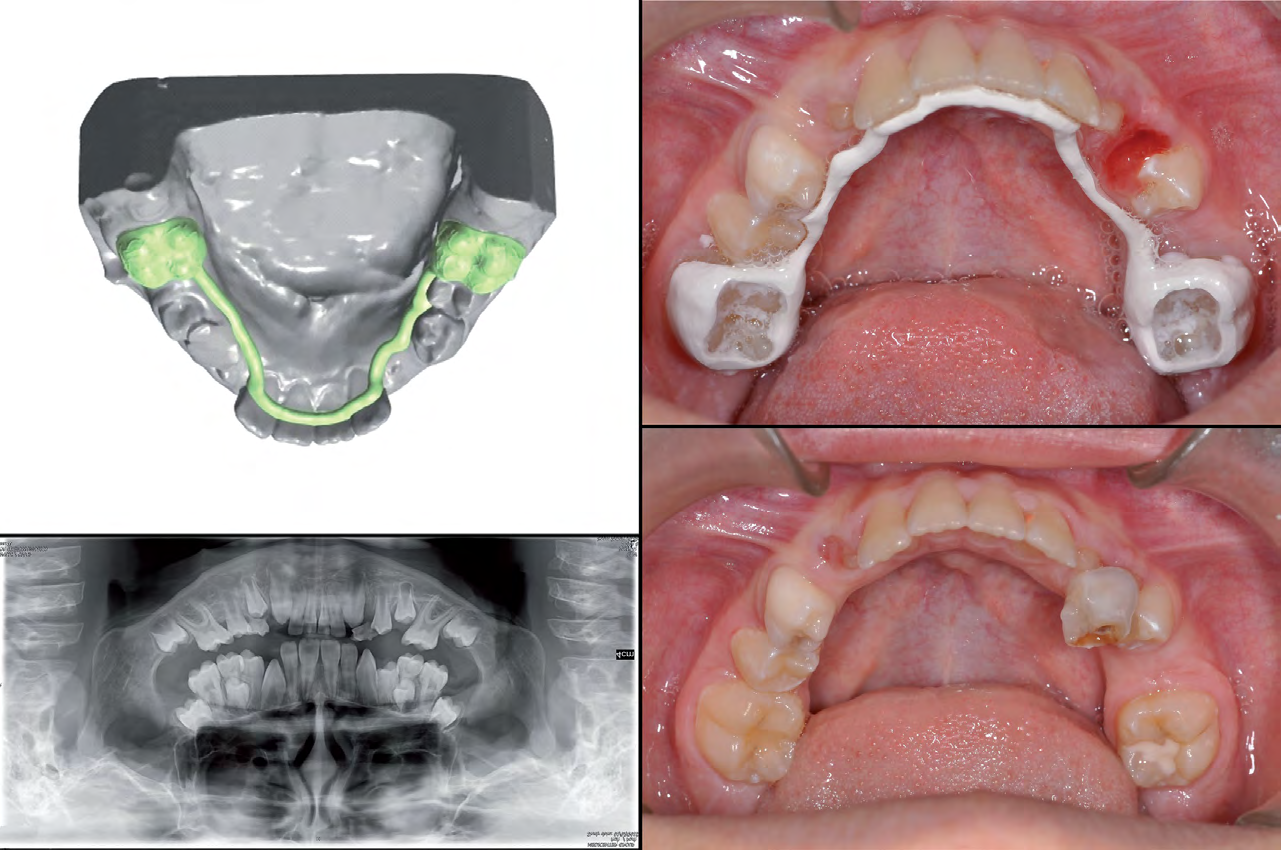
In the second case, the planned device was a band with loop. The patient was ten years old and had an abnormal inclination of the permanent right upper canine. After clinical and radiographic evaluation we decided to extract the deciduous canine to favor the spontaneous eruption of the permanent canine. It was necessary a band on the first right molar and a loop in contact with the lateral right incisors in order to maintain the necessary space (Figure 7).
The last case shows a removable plate. The patient was 8 years old, had a supernumerary which interfered with the proper central incisor eruption. The supernumerary caused a delay of incisor eruption. Thanks to the central incisor’s eruptive force, the treatment plan was to extract the deciduous incisor and the supernumerary and to maintain the space during the permanent incisor’s eruption (Figure 8).
According to a nine month- follow up all 3 patients found the devices comfortable and very satisfying because they were personalized and minimally visible. These devices were found suitable to maintain the space. Then they remained stable, no dis-cementation or fracture was observed. No allergy or presence of plaque was described. The workflow allowed a simulation of the treatment plan with a better collaboration and acceptance of the patient. Digital system reduced the systematic mistakes during the various phases, decreasing production time. It needs to stress the concept of digital and not hand-made steps in order to have greater precision and less discomfort. The digital system saved space creating a virtual plaster casts collection.
Single Unit Polyetheretherketone Crown Restoration
A pilot study was conducted on twenty patients who required crown placement on vital or non-molars. The teeth preparations were done according the standard operative procedures based on the guidelines given by Shillingburg, et al. [41]. After tooth preparation was completed, isolation was carried out, and then, gingival retraction cord (Ultapak, USA) was placed using a cord packer into the gingival sulcus and impressions of the prepared teeth were made using stock trays loaded with putty (Dentsply Sirona, Germany) and light body elastomeric impression material (Reprosil
light body, Dentsply, USA). The impression of the opposing arch was made as well. Temporary crowns were fabricated, finished and cemented using non-eugenol based temporary luting cement.
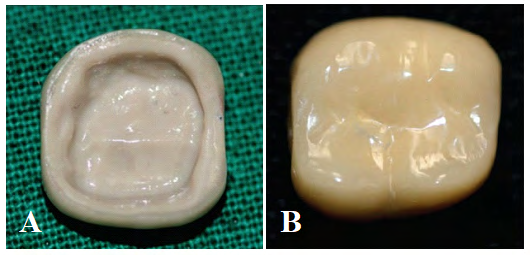
The models were made from the final impression using die stone (Elite rock, Zhermack, Italy) which were then scanned using a scanner. The coping was designed using a CAD program. The PEEK (Auvaro, United Kingdom) coping was milled using CAM. PEEK frameworks were coated with Visiolink (Bredent, Germany) followed by layering with composite (ADORA Composite, Shofu Ceramage) as per design (Figures 9a & b). The final restoration was then checked intraorally for any premature contacts. Once all aspects were evaluated the restorations were cemented using resin cement (RelyX™ U200, Germany) [42].
The patient was recalled at intervals of 3 months and 6 months and 1 year. The survival rate at 1 year was 95%. There was one fracture of framework that had to be replaced during the observation period. This study was concluded that the high level of accuracy of fit (crown retention, marginal quality and marginal accuracy) and esthetic accomplished with PEEK material was deemed very satisfying. During the observation period no marginal discoloration or caries were noticeable. The patients also were extremely satisfied by the feel and comfort of the crown. Even though these crowns could not completely mimic the translucency of natural teeth still were capable enough to give a good esthetic match and provide good patient satisfaction. Considering the mean observation time of a year, PEEK single crowns seem to exhibit promising clinical survival rates with excellent patient satisfaction and not much of mechanical failure and biological reactions as well. Further studies may be carried out to compare the PEEK crowns fabricated using different methods (surface treatment and bonding). A split mouth study can also be done to compare it with another material [42].
The Use of PEEK Material in Fixed and Removable Prostheses
There are several advantages of PEEK material as the substructure in fixed and partial prostheses. These include that it can be more easily produced compared to metal substructure, and those produced with CAD- CAM systems can be more easily applied with abrasion in a short time without damaging the burrs [43]. With the introduction of CAD-CAM techniques in dentistry, it has become possible to fabricate restorations, frameworks and appliances using modern biocompatable materials including alloys, ceramics and high-performance polymers. Many of these materials cannot be processed or can only be processed with great difficulty using conventional methods. One of these newer materials is the thermoplastic composite polymer known as PEEK.
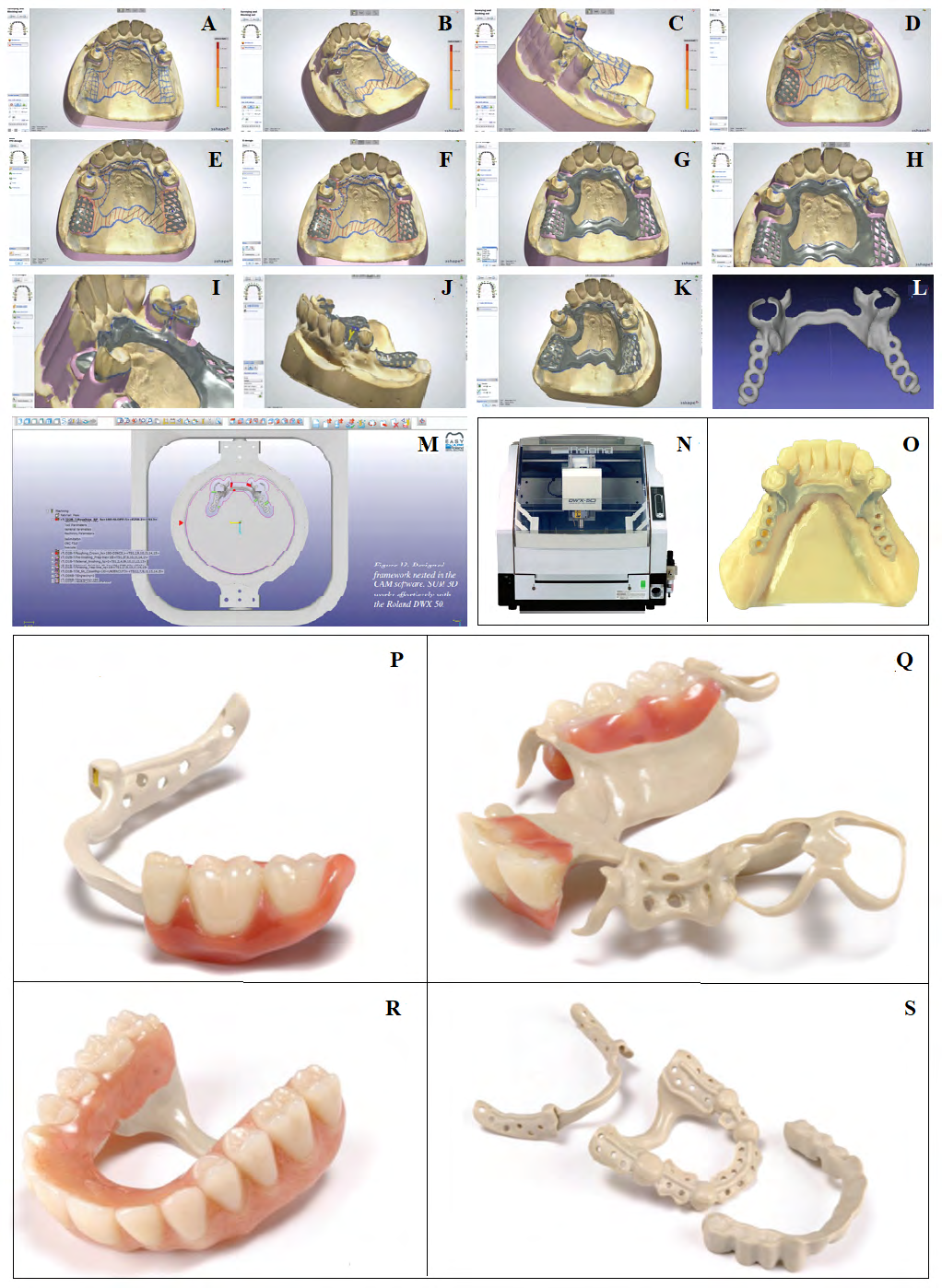
One notable dental brand of PEEK is JUVORA. Their ultra high purity “filler free” type of PEEK is unique in the marketplace and has been used in 4 million medical device implants, Juvora is a true unfilled pure form of PEEK and really does mill effortlessly with the Roland DWX 50 with SUM 3D CAM software already having a preset strategy to suit. Bridge frameworks milled from a high-grade, industrially manufactured block undergo no physical changes during the fabrication process and possess the same material/ technical properties. PEEK exhibits a perfect balance of the properties desirable to frameworks and can be milled very easily, especially with an affordable Roland DWX 50 milling machine. Figures 10 A-O follow the general workflow of a CAD designed and milled partial denture framework using a Roland DWX 50 Milling unit, SUM 3D CAM software and 3Shape CAD software. Figures P-S show what is possible [43].
Workflow procedures for PEEK CAD-CAM using Roland DWX 50 with SUM 3D CAM software are as follows (Figure 10): A) Scan from a 3Shape D900 color scanner. This scanner has the ability to scan and reproduce drawn lines from a stone model, B) Using the 3Shape Partial Denture Designer, the digital model is surveyed, path of insertion is determined and undesirable undercuts are blocked out, C) Blocking out of undercuts. Virtual wax can be shaped to the desired height of contour and undercut for clasps. Undesirable undercuts are blocked, D) Retention grids are designed, E) Various retention grid designs are available, F) Tracing the spline for the major connector. a spline in this situation is a drawn curve on the 3D model, G) Rendering of the major connector framework, H) Rest formation, I) Clasp design, J) Support post design, K) Finished 3D design, L) A 3D Designed framework opened in an inspection program and ready for milling, M) Designed framework nested in the CAM software. SUM 3D works effortlessly with the Roland DWX 50, N) The Roland
DWX 50 is a 5-axis machine more than capable of milling most materials. Perfect to mill PEEK, O) Milled framework from Roland DWX 50. NB: only the milling connectors have been trimmed. Surface finish is amazing, P) An example framework with teeth added to one saddle area, Q) Another example of PEEK framework with some teeth added, R) Full upper denture design over PEEK framework, and S) Various examples of PEEK frameworks.
Conclusion
Several in vitro studies and clinical reports suggested that PEEK could be suitable for CAD-CAM fabricated fixed, removable, orthodontic, and pediatric appliances due to its favorable mechanical, chemical and physical properties. However, further in vitro and clinical studies are needed to evaluate the long-term performance of these prostheses before PEEK can be safely recommended as an alternative to well-established prosthodontic materials [44]. Design improvements and the search for new manufacturing materials require further research [39]. Digital work is in constant evolution in dentistry. For this reason, we hope that more complex devices will be created with this method and also with this material in the future. Other techniques such as 3D printing may be an alternative option that can be studied. Further clinical studies are also necessary to establish their active function once defined the passive role of these devices [2].
References
-
Auconi P, Caldarelli G, Scala A, Ierardo G, Polimeni A (2011) A network approach to orthodontic diagnosis. Orthod Craniofac Res 14(4): 189-197.
-
Ierardo G, Luzzi V, Lesti M, Vozza I , Brugnolett O, et al. (2017) Peek polymer in orthodontics: A pilot study on children. J Clin Exp Dent 9(10): 1271-1275.
-
Li RW, Chow TW, Matinlinna JP (2014) Ceramic dental biomaterials and CAD/CAM technology: state of the art. J Prosthodont Res 58(4): 208-216.
-
Sannino G, Germano F, Arcuri L, Bigelli E, Arcuri C, et al. (2015) CEREC CAD/CAM chairside system. Oral Implantol (Rome) 7(3): 57-70.
-
Schwitalla AD, Spintig T, Kallage I, Müller WD (2015) Flexural behavior of PEEK materials for dental application. Dent Mater 31(11): 1377-1384.
-
Stawarczyk B, Beuer F, Wimmer T, Jahn D, et al. (2013) Polyetheretherketone- A suitable material for fixed dental prostheses?. J Biomed Mater Res B Appl Biomater 101(7): 1209-1216.
-
Rho JY, Ashman RB, Turner CH (1993) Young’s modulus of trabecular and cortical bonematerial: Ultrasonic and microtensile measurements. J Biomech 26(2): 111-119.
-
Alexakou E, Damanaki M, Zoidis P, Bakiri E, Mouzis N, et al. (2019) PEEK High Performance Polymers: A Review of Properties and Clinical Applications in Prosthodontics and Restorative Dentistry. Eur J Prosthodont Restor Dent 27(3): 113-121.
-
Malpo P, Araújo NM, Borges J, Almeida R (2012) Retrievable metal ceramic implant-supported fixed prostheses with milled titanium frameworks and all- ceramic crowns: retrospective clinical study with up to 10 years of follow-up. J Prosthodont 21(4): 256-264.
-
Menini M, Conserva E, Tealdo T, Bevilacqua M, Pera F, et al. (2011) The use of a masticatory robot to analyze the shock absorption capacity of different restorative materials for implant prosthesis. J Biol Res 84: 118-119.
-
Halabi ElF, Rodriguez JF, Rebolledo L, Hurtós E, Doblaré M (2011) Mechanical characterization and numerical simulation of polyether-ether-ketone (PEEK) cranial implants. J Mech Behav Biomed Mater 4(8): 1819-1832.
-
Rosentritt M, Schneider FS, Behr M, Preis V (2017) In vitro shock absorption tests on implant-supported crowns: influence of crown materials and luting agents. Int J Oral Maxillofac Implants 33(1): 116-122.
-
Jenkins MJ (2000) Relaxation behavior in blends of PEEK and PEI. Polymer 41(18): 6803-6812.
-
Yurchenko ME, Huang J, Robisson A, McKinley GH, Hammond PT (2010) Synthesis, mechanical properties and chemical/solvent resistance of crosslinked poly(aryl-ether-ether-ketones) at high temperatures. Polymer 51(9): 1914-1920.
-
Rodriguez F, Cohen C, Ober CK, Archer L (2014) Principles of Polymer Systems, 6th (Edn.). New York: Taylor & Francis US.
-
Korn P, Elschner C, Schulz MC, Range U, Mai R ,et al. (2015) MRI and dental implantology: two which do not exclude each other. Biomaterials 53: 634-645.
-
Wiesli MG, Ozcan M (2015) High-performance polymers and their potential application as medical and oral implant materials: a review. Implant Dent 24(4): 448- 457.
-
Han KH, Lee JY, Shin SW (2016) Implant-and tooth- supported fixed prostheses using a high-performance polymer (Pekkton) framework. Int J Prosthodont 29(5): 451-454.
-
Victrex PEEK-OPTIMA™ Product Guide.
-
Andres TE, Griffiths I (1998) Proceedings of 1998 SPE Annual West Regional Meeting, Anaheim, CA (Soc. Pet. Eng. Richardson, TX, USA) pp: 203-237
-
Schwitalla AD, Abou Emara M, Zimmermann T, Spintig T, Beuer F, et al. (2016) The applicability of PEEK-based abutment screws. J Mech behav biomed mater 63: 244- 251.
-
Wiesli MG, Özcan M (2015) High-performance polymers and their potential application as medical and oral implant materials: a review. Implant dent 24(4): 448- 457.
-
Najeeb S, Zafar MS, Khurshid Z, Siddiqui F (2016) Applications of polyetheretherketone (PEEK) in oral implantology and prosthodontics. J prosthodontic res 60(1): 12-19.
-
Patil R (2015) Zirconia versus titanium dental implants: A systematic review. Journal of Dental Implants 5(1): 39- 42.
-
Schwitalla A, Muller WD (2013) PEEK dental implants: a review of the literature. Journal of Oral Implantology 39(6): 743-749.
-
Araújo NM, Maló P, Gonçalves I (2015) Evaluation of clinical soft tissue parameters for extramaxillary zygomatic implants and conventional implants in all- on-4 hybrid rehabilitations: Short-term outcome and proposal of clinical recommendations for intervention in recall appointments. Implant Dent 24(3): 267-274.
-
Araújo NM, Guedes CM, Ricardo AR, Silva A (2021) Poly- ether-ether-ketone and Implant Dentistry: The future of mimicking natural dentition is now!. Polym Int pp: 1-3.
-
Harb IE, Abdel KEA, Hegazy SA (2019) CAD/CAM constructed poly (etheretherketone) (PEEK) framework of Kennedy class I removable partial denture: a clinical report. J Prosthodont 28(2): 595-598.
-
Zoidis P, Papathanasiou I, Polyzois G (2016) The use of a modified poly-etherether-ketone (PEEK) as an alternative framework material for removable dental prostheses: a clinical report. J Prosthodont 25(7): 580- 584.
-
Costa PS, Torrents NJ, Brufau BM, Cabratosa TJ (2014) Use of polyetheretherketone in the fabrication of a maxillary obturator prosthesis: a clinical report. J Prosthet Dent 112(3): 680-682.
-
Benli M, Eker Gümüş B, Kahraman Y, Gökçen Rohlig B, Evlioğlu G, et al. (2020) Surface roughness and wear behavior of occlusal splint materials made of contemporary and high-performance polymers. Odontology 108(2): 240-250.
-
Papathanasiou I, Kamposiora P, Papavasiliou G, Ferrari M (2020) The use of PEEK in digital prosthodontics: A narrative review. BMC oral health 20(1): 217.
-
Kaleli N, Sarac D, Kulunk S, Oztürk O (2018) Effect of different restorative crown and customized abutment materials on stress distribution in single implants and peripheral bone: a three-dimensional finite element analysis study. J Prosthet Dent 119(3): 437-445.
-
Beretta M, Poli PP, Pieriboni S, Tansella S, Manfredini M, et al. (219) Periimplant soft tissue conditioning by means of customized healing abutment: a randomized controlled clinical trial. Materials (Basel) 12(18): 3041.
-
Abdullah AO, Tsitrou EA, Pollington S (2016) Comparative in vitro evaluation of CAD/ CAM vs conventional provisional crowns. J Appl Oral Sci 24(3): 258-263.
-
Kalia G, Tandon S, Bhupali NR, Rathore A, Mathur R, et al. (2018) Speech evaluation in children with missing anterior teeth and after prosthetic rehabilitation with fixed functional space maintainer. J Indian Soc Pedod Prev Dent 36(4): 391-395.
-
Srivastava N, Grover J, Panthri P (2016) Space maintenance with an innovative “tube and loop” space maintainer (Nikhil appliance). Int J Clin Pediatr Dent 9(1): 86-89.
-
Kawara M, Komiyama O, Kimoto S, Kobayashi N, Kobayashi K, et al. (1998) Distortion behavior of heat- activated acrylic denture-base resin inconventional and long, low-temperature processing methods. J Dent Res 77(6): 1446-1453.
-
Guo H, Wang Y, Zhao Y, Liu H (2020) Computer-aided design of polyetheretherketone for application to removable pediatric space maintainers. BMC Oral Health 20(1): 201.
-
Richard N (2012) The future of dental devices is digital. J Dent mater 28(1): 3-12.
-
Shillingburg HT, Sather DA, Wilson EL, Cain JR, Mitchell DL, et al. (2012) Fundamentals of Fixed Prosthodontics. 4th (Edn.), USA: Quintessence Publication.
-
Sulaya K, Guttal SS (2020) Clinical evaluation of performance of single unit polyetheretherketone crown restoration-a pilot study. J Indian Prosthodont Soc 20(1): 38-44.
-
Whitty T (2018) PEEK A new material for CADCAM dentistry. Juvora Dental Innovations.
-
Papathanasiou I, Kamposiora P, Papavasiliou G, Ferrari M (2020) The use of PEEK in digital prosthodontics: A narrative review. BMC Oral Health 20(1): 217.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells