Clinical Approach to a Tooth with Irreversible Pulpitis: A Case Report
Introduction: A case report which describes the practical steps and clinical treatment approach for the endodontic treatment of a posterior tooth with irreversible pulpitis utilizing Protaper gold files. Digital imaging was utilized for each clinical stage. Objective: To outline clinical steps taken to manage irreversible pulpitis and, the endodontic treatment thereof. Results: The clinical approach was based on detailed treatment plan, precise and accurate diagnosis which ensured proper classification of disease of the pulp together with various diagnostic aids to determine pulpal status and appropriate root canal therapy. The oral health status and root anatomy were documented together with a detailed step-wise approach for management of irreversible pulpitis by use of basic K-files, digital imaging (DI) and rotary Protaper gold files. An acceptable endodontic result was achieved with patient satisfaction and functionality. Conclusion: The described case report revealed successful endodontic treatment in a premolar tooth which had irreversible pulpitis and it also provides the detailed approach to conservatively manage the tooth that had a good prognosis.
Introduction
Dental pain management is one of the most crucial steps in endodontic treatment. Irreversible pulpitis occurs when inflammation and other symptoms such as pain become severe [1]. The pain can be quite sudden and often followed by thermal and sweet sensitivity that can last for longer duration. Therefore, pain can be intense, linger to temperature changes, spontaneous, diffuse and be referred to other orofacial areas [1].
The dental pulp is a complex arrangement of connective tissue, neurovascular tissue and humoral cells. When exposed to numerous external stimuli, including bacterial invasion through dental caries, tissue inflammation, the effects thereof are the clinical signs and symptoms of ‘reversible and irreversible pulpitis’ [2]. The inflammatory status of the pulp can be reversed if the noxious stimulus is removed, as long as it is not outside the pulp’s capacity to settle, heal and/ or repair [2]. However, if the external stimulus overcomes the pulp’s innate defense and repair mechanisms, then it becomes an excruciating, acutely inflamed and ‘irreversibly’ damaged, resulting in pulp necrosis [2].
It is commonly known that the primary pain for pulpitis is caused by direct dentin destruction due to microbial invasion and alteration in osmotic pressure of dentinal tubules [2]. Aetiologically, which is secondary to microbial effect, is hypersensitivity of the pulp nerve fibers due to inflammatory reactions. It appears that the C nerve fibers are more affected by inflammatory stimulators in the pulp [2]. In all-purpose, the A delta fibers respond to the stimulators related to the dentinal tubules whereas the C fibers mostly respond to inflammatory stimulators which are interpreted as long-standing and vague pain sensation. It is understood that when the pulp nerve fibers are affected by chemical mediators, the action potential procedure would be facilitated or spontaneously started [2]. Some of the inflammatory chemical mediators activate nerve fibers, and some of them toughen the nerve fibers responses. So, when large numbers of chemical mediators exist, the nerve response is more intense. It is indicated that some chemical mediators like nerve growth factor are effective in prolonged pain [2].
As disease progresses, the periapical region becomes involved, the tooth becomes sensitive to percussion and the proprioceptive nerve endings in the periodontal ligament space get stimulated. In literature it is evidenced that the utmost suitable treatment for irreversible pulpitis requirements to be definite diagnosis and identification of pain etiology [1]. The treatment for controlling the pain as per its original sources differs from case to case. It is conceivable that the pain becomes referred or originates from the other teeth [1]. It is thus important to reach a correct diagnosis and recognition of pain reason. Clinical signs and symptoms, vitality tests and precise evaluation of tooth can be helpful in recognition of the source of pain. The most important step is to anesthetize the tooth and be able to successfully manage the cause of pain.
Diagnosis and management of this clinical case was based on the coexistence of two clinical conditions, irreversible pulpitis on the upper right premolar tooth (15) and the longstanding chronic maxillary sinusitis. Uniqueness of this case report was based on the fact that an infected root canal system can exacerbate pain of the upper maxillary sinuses. Therefore, management of the upper right premolar tooth (15) was done by eliminating the infected pulp which was also greatly beneficial to the wellbeing of the patient.
The main aim of this case report is to outline the common techniques and approaches to provide successful pain management of irreversible pulpitis.
Case Report
A 38-year-old female presented with an upper right premolar (15) which was sensitive and painful to cold, hot, sweet and upon biting. The patient stated that the tooth had continuous sharp and shooting pain. The patient also reported that she once experienced pain in April 2019 but it disappeared and that subsequently the pain was more severe. She informed the clinician that the tooth was previously restored.
Upon extra-oral examination (EOE), there was no facial swelling and temporomandibular joint dysfunction was noted due to the presence of a right click and sinuses were tender upon palpation.
Upon intra-oral examination (IOE), revealed a composite resin restoration on tooth 15 with no fracture or cracks and there was a good overall oral hygiene with healthy gingiva, had slight fluorosis on anterior maxillary teeth, had signs of bruxism and attrition with wear facets, crown on tooth 47 and numerous composite restorations (Figure 1).
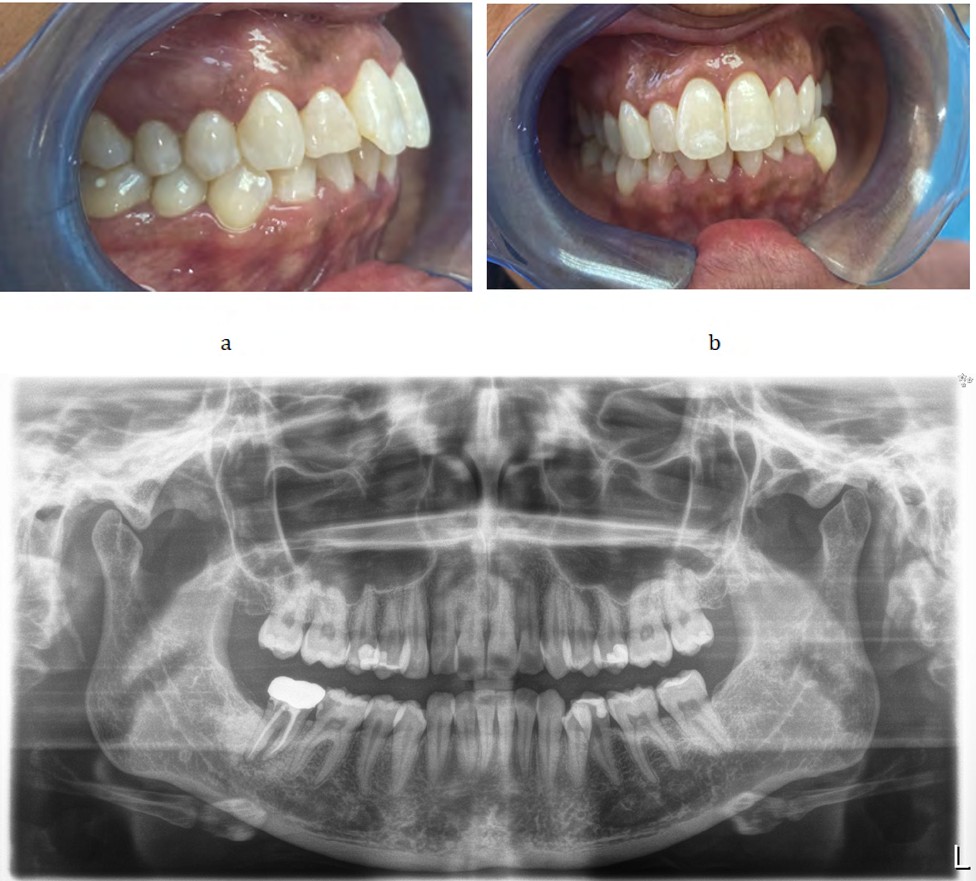
Figures 1a and 1b: Pre-operative clinical view of tooth 15 and slight fluorosis on anterior teeth.
Diagnostic tests were performed and the tooth was sensitive to cold (ethyl chloride was used for cold sensitivity test), to hot (warm gutta percha was used for hot sensitivity), slight tenderness in the periapical was present and there was no tooth mobility (Figure 2).
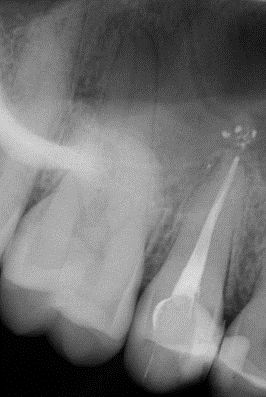
On radiographic examination, (extra-oral panoramic x-ray), the following features were noted: a crown and root treated 47, composite restorations on 17, 16, 15,14, 25, 27, 37 and radiolucency indicating carious defect on disto occlusal of 46 (Figure 2). On intra-oral preapical x-ray, it was noted that there was a large composite resin restoration on tooth 15, which was situated close to the pulp chamber as well as distal radiolucency (possible secondary carious) defect beneath the restoration as per extra oral panoramic x-ray. There was also widening of the periodontal ligament space around the root of tooth 15. A composite restoration was also observed on the distal aspect of tooth 14 with possible recurrent caries as observed radiolucency beneath the restoration (Figure 3).

A pre-treatment diagnosis for tooth 15 in this patient was confirmed to be irreversible pulpitis based on clinical signs and symptoms and radiographic findings. Notably the patient is bruxer and received treatment advice regarding biteplate to alleviate the symptoms.

After an informed and signed consent, the patient was anaesthetised, emergency root canal treatment (ERCT) was performed and 2 canal orifices were found buccal and palatal respectively with a working length (WL) of 21mm (Figure 4). Irrigation and debridement using Milton (1% NaoCl) as well as 17% EDTA solution (Pacdent) was carried out by the clinician. An intra-canal medicament, calcium hydroxide on Teflon tape was applied and coltosol temporary restoration was placed.
An appointment was scheduled for 6 days later for subsequent management of the case. The patient was symptom free and was anaesthetized. A size 10 K-file (Dentsply Sirona was introduced to length of 21mm, connected to NSK Ipex II Apex Locator in order to establish the correct working length to a reading of 0.3 at 21mm and rubber dam placement for isolation was done (Figure 5). 2 canals were shaped and filled using protaper gold system with a speed of 300 rpm and toque of 1.5N using an Endomate (NSK) handpiece.

EDTA chelating agent (Essential Range, Wright Millners) was used and it was found that 2 canals joined into 1 large canal closer to the apex. The following sequence of files were used, SX, S1, S2, F1, F2 and last file used was F2 to working length (WL) of 21 mm. During the filing/debridement technique copious amount of irrigants (17%EDTA initially followed by chlorolex5.25% and finally 1%NaOCL) were flushed into the canal. Endo activator was used to activate irrigation solutions. The final rinse involved a flushing with sodium hypochlorite solution. Cone fit and obturation of the canal was done using F2 gutta percha 0.6 taper plus cold lateral technique. FKG Totalfilll bioceramic sealer was dispensed into the coronal and middle thirds of the canal, thereafter the final restoration was done using 3M Espe Bulkfill flowable composite followed by 3M espe composite. A post-operative radiograph was then taken (Figure 6).

Postoperative follow up visits were 10-days later and intra-oral periapical x-ray was taken (Figure 6), there was still slight tenderness and discomfort and laminate biteplate was also delivered six months later a panoramic radiograph was taken and the patient was asymptomatic (Figure 7). Post-operative follow up intra-oral x-ray was taken one year later and the patient was asymptomatic (Figure 8).
Discussion
Most clinicians are curious, interested and intrigued by the successful outcomes of correct tooth debridement of the root canal and its final obturation. Clinical encounters, different approaches, type of instruments, files and different intra-oral imaging modalities, extra- oral imaging modalities are stated by various authors but all clinical outcomes are unique to individual patients [3, 4]. Other authors specified that the importance of correct diagnosis and treatment planning cannot be underestimated [4]. Notably, there are countless causes of facial pain and the differential diagnosis can be complicated, difficult and demanding. All the important information about the patient must be collected; this includes medical and dental history, the results of both a clinical examination and diagnostic tests. The clinician should be well versed with the prognosis for different endodontic clinical conditions.
Pre-operative diagnosis is vital and an accurate diagnosis of the patient’s condition is crucial before an appropriate treatment plan can be formulated for that individual case. A reasonable and compassionate approach to clinical examination should be adopted.
In addition, 17% EDTA solution combined with small amounts of 1% sodium hypochlorite with the effervescent effect can be useful for the canal debridement. Use of chelating agents such as paste EDTA (Essential range, Wright Millners) are criti the initial stages to provide lubrication to instruments and also help in avoiding file separation. The use of digital radiography can also contribute greatly in successful management [3].
Successful management of the steps lead to increased depth of penetration, cleaning, shaping and obturation with appropriate use of instruments and materials lead to a, acceptable outcome and final restoration (Figures 7 and 8).
There are many encounters in carrying out treatments for teeth with acute pulpitis and such cases with irreversible inflamed pulp may be hyperalgesic which is difficult to anaesthetize [2]. Previous authors emphasized the significance of complete debridement of inflamed and necrotic pulp tissue as the main aim of conventional root canal therapy [2, 4, 5]. Literature reviews also indicate that antibiotics don’t seem to significantly reduce pain caused by irreversible pulpitis [5]. It does not reduce the percussion perception or quantity of pain medication taken. It does however, facilitate antibiotic resistance and should be prescribed only where indicated [6]. The ideal outcome in all clinical situations should include overall healing as well as prevention of disease and infection. The main aim should involve functional retention of the tooth. Understanding the risk factors associated with endodontic failure is a key factor to increase the chances of success [7].
Conclusion
The described case illustrates a typical approach to manage a case of a tooth with irreversible pulpitis by recommended clinical guidelines and techniques. Similar cases may be difficult to approach for other clinicians due to lack of clinical experience, expertise and availability of adequate instruments and equipment.
References
-
Modaresi J, Davoudi A, Badrian H, Sabzian R (2016) Irreversible pulpitis and achieving profound anesthesia: Complexities and managements. Anesth Essays Res 10(1): 3-6.
-
Gemmell A, Stone S, Edwards D (2020) Investigating acute management of irreversible pulpitis: a survey of general dental practitioners in North East England. Br Dent J 228(7): 521-526.
-
Cohenca N, Simon JH, Roges R, Morag Y, Malfaz JM (2007) Clinical indications for digital imaging in dento-alveolar trauma Part 1: traumatic injuries. Dent Traumatol 23(2): 95-104.
-
Carrotte P (2004) Endodontics: Part 2 Diagnosis and treatment planning. Brazilian Dental Journal, 197(5): 231-238.
-
Ahmed H (2014) Elective root canal treatment: A review and clinical update. ENDO-Endodontic Practice Today 8(2): 139-144.
-
Agnihotry A, Fedorowicz Z, van Zuuren EJ, Farman AG, Al Langawi JH (2016) Antibiotic use for irreversible pulpitis. Cochrane Database Syst Rev 2: CD004969.
-
Estrela C, Holland R, Estrela CR, Alencar AH, Sousa Neto MD, et al. (2014) Characterization of successful root canal treatment. Braz Dent J 25(1): 3-11.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells