Applicability of Thermography in Dentistry-Scoping Review
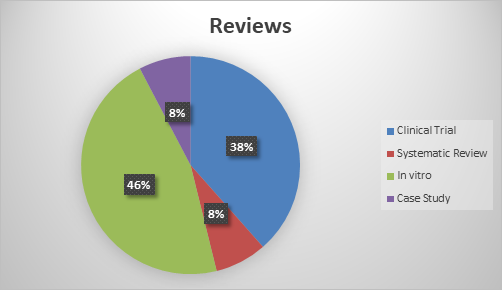
Introduction: Thermography offers a non-invasive radiation-free methodology for diagnostic imaging and temperature measurement, but the extent of the current application is unclear, as is the level of evidence for each use case. Moreover, population-based thermographic reference values for diagnostic purposes are nearly unknown. The present scoping review aims to assess the extent of literature and available evidence regarding the application of infrared thermography in dentistry to establish indications and further scope of its utility. Material and Methods: PubMed, Cochrane Database of Systematic Reviews and CENTRAL and Web of Science searches were done in July 2022 with specific keywords. Wide eligibility criteria were used to capture all relevant studies, published in English, and addressing thermal imaging in dentistry. The literature found was selected regarding the eligibility criteria. Relevant data was extracted from the included references into a collection chart in a synthesized narrative format and classified under the Levels of Evidence and Grades of Recommendation (Oxford Centre for Evidence-based Medicine, March 2009). Results: 13 studies were selected, 6 in vitro, 5 clinical trial and 1 case study and 1 systematic review. Four studies related the temperature variation of dental pieces with pulpal diagnosis. Three evaluated the effectiveness of thermography in the diagnosis of temporomandibular disorders. Five were used in surgery to measure inflammatory responses resulting from surgical procedures and temperatures reached when cutting hard tissues. One study evaluated, from an ergonomic point of view, the impact of bad working positions of oral health professionals. Conclusion: Within the limitations of this review, studies suggest that thermography has the potential to become an important tool in dental medicine, either as an auxiliary means of diagnosis in endodontics and temporomandibular disorders or as a complementary element in cutting procedures capable of producing heat with implications for the viability of the underlying structures. In addition, this scoping review can rouse new research foci regarding thermography
Introduction
Thermography is a non-invasive technique that allows the measurement of the temperature distribution of any object that is superior to the absolute temperature of -2730C, adequate to body surface. Above this value the body emits infrared rays proportionally, due to the vibrations and rotations of the atoms and molecules that constitute the object, being possible to measure its temperature by measuring the infrared output [1, 2, 3].
This technique is important within the scope of evaluating thermographic alterations that indicate pathological situations at a general level and its main advantage is not being harmful for the human body, as it does not use gamma or X -rays. It is easy to use and highly configurable, affordable comparing to other auxiliary means of diagnosis, allows visual perception by the difference of color that change in real-time, as well as the rapid acquisition in stationary targets and the capture of thermal patterns [1, 2, 3]. There are two methods usually used to register thermic images. The semi-quantitative method, which is cheaper and uses liquid crystals, Liquid Crystal Thermography, and a quantitative method of infrared detection characterized as Infrared Thermography [4, 5].
Infrared thermography is a method of non-contact, for measuring temperature, where the detector is placed remotely on a site. This method consists of an infrared detector, amplifier-digitizer, a microcomputer, and a video display. The infrared detector can either have a single element with a linear array or a bi-dimensional array [1, 6].
The thermal images that are obtain are characterized by spatial resolution, that is, by the capacity of differentiation between two points next to each other, and by their thermal resolution or the difference by which the minimum temperature that may be measured between two distinct points in an image. Another related parameter is the temporal resolution, being the delay time between the temperature change and the location/area where it was monitored in the thermal image [4].
Regarding facial thermographic image, heat emissions from the human face have been demonstrated to be physiological indicators delineating health versus disease. The heat emission is directly related to the vascular cutaneous activity, exacerbating the heat on vasodilation, and reducing heat on vasoconstriction. In the facial area, infrared tele thermography may be useful, as a non-invasive diagnostic technique, which may help differentiate specific clinical problems. The radioactivity dissipation pattern on human heat is, usually, symmetrical. Small differences are displayed through a hemi-facial control, choosing 10 points side by side (circa 0.280C) [6, 7].
However, it is necessary to know the existing differences within the human body to identify health from disease. A significant difference between the absolute facial temperature of men and women have also been observed. Men have higher temperatures in about 25 anatomical zones on the face (orbits, upper lip, lower lip, chin, cheek, among others) than women. That is understandable due to men’s higher metabolic rate, so they dissipate more heat by corporal surface area unit. Age and ethnicity may also have a variation in facial temperature [6, 7].
Structurally, teeth have a very poor heat transference. As its thermal conductivity is extremely low (0,6 Wm-1K-1). It is necessary to study the dynamic of the heat transfer through the amelodentinal tissue, to identify and understand possible pathological behaviors [8, 9].
This kind of behavior generates challenges in its measurement, due to a complex functional and biological environment and geometry. It is important also to investigate the behavior of transfer and dissipation of the enamel and dentin portions of the human tooth, as these two materials have different thermophysical properties [6, 7].
According to literature, the thermal diffusion through hard-dental tissues, namely dentin, and enamel, is inferred through the temperature change depending on the origin of the stimulus, time and respective layers involved. The temperature gradient is continuously distributed across the enamel and dentin layers and its junction below a temperature of 42℃, however, if the temperature is higher than this value, a negative thermal resistance is observed [6, 7]. These results suggest that the microstructure of the enamel dentin junction plays a predominant role in the heat transfer and protects the pulp from damage caused by heat transfer across the dentin- enamel junction in human teeth [6, 7].
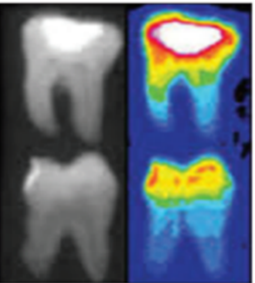
Source: Adapted from Harshavardhan, et al. [6]. Figure 1: Thermographic image of an inflamed pulp.
Studies with thermographic images in human teeth, to evaluate the pulp vitality, are yet few and are an ongoing investigation [10]. A comparison between vital and non-vital, pulp tissue was made, and it was observed that the dental surface from de vital tissue was warmer, in comparison with a tooth without blood irrigation [11, 12]. After a reduction in temperature, non-vital teeth take longer to reheat than vital ones [13]. This procedure implies the teeth to be isolated with a rubber dam as a standard procedure, after an acclimatization period before register the image. It is a complex procedure, demanding one hour of relaxation before the patients can be submitted to the test [6, 8, 10].
Under these considerations, this innovative technique presents many challenges, especially in the measurement of the thermal conductivity of enamel and dentin.
The aim of this scoping review is to go through the available literature and assess the indications and the evidence regarding the applicability of infrared thermography in dentistry and further scope of its utility.
Methodology
Based on the methodology outlined by Levac, et al. [14] Arksey & O’Malley [15] this scoping review consisted of six stages.
Stage 1: Formulating the research question. Following a preliminary exploration of published literature, the following research questions were identified:
- In which way could Thermography be a useful asset to Dentistry?
- Which challenges and advantages will arise with the use of this technique in Dentistry?
Stage 2: Identifying relevant studies
Information Sources and Search Strategy
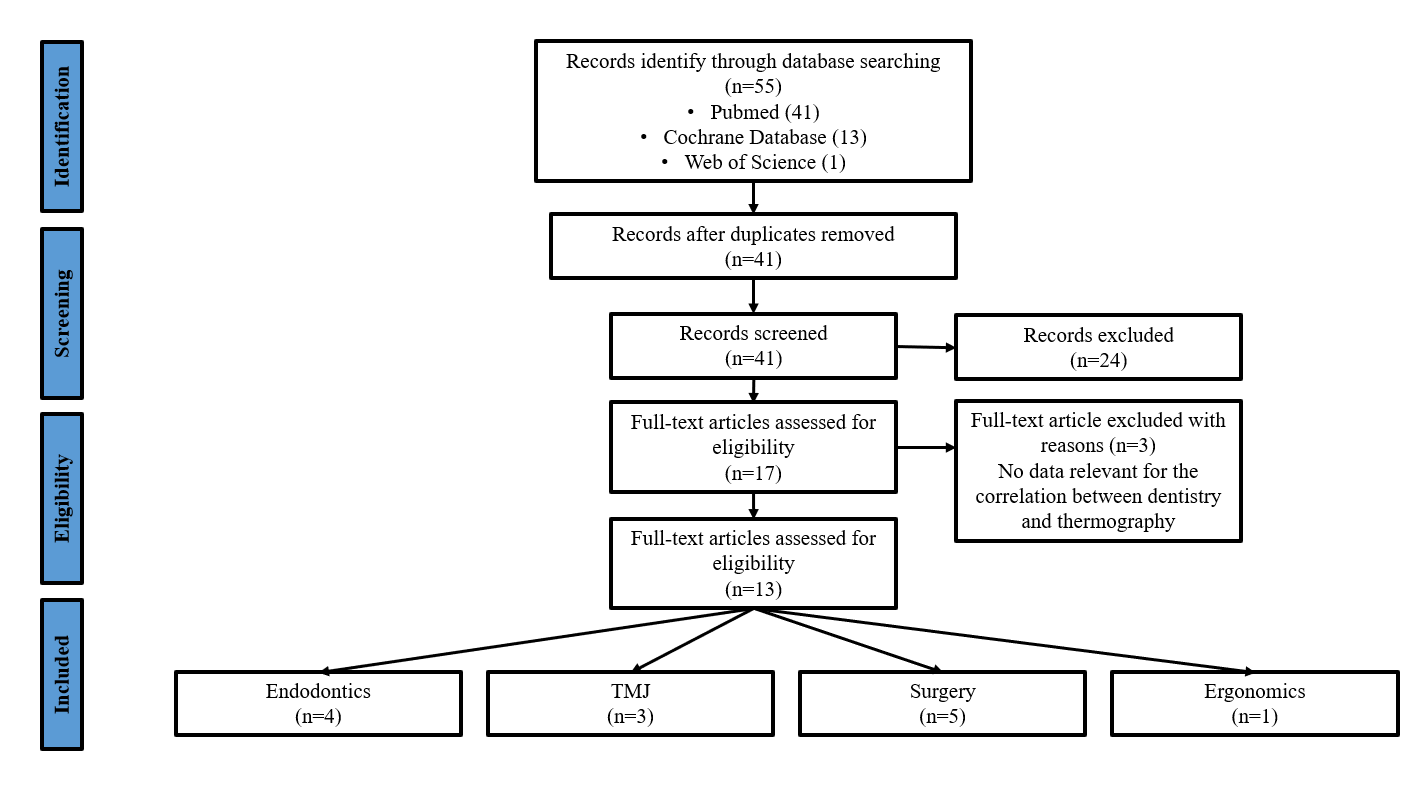
Stage 3: Study selection Two levels of screening were performed: (1) title and abstract review, and (2) full-text review. For level one, a reviewer, checked titles and abstracts for full-text review based on the inclusion criteria. In level two, were included if perspectives on thermography use in dentistry were described. The PRISMA flow diagram tracking progress is shown in Figure 2 [16].
Following several preliminary scoping searches which were intended to gain familiarity with the literature and aid with the identification of keywords, three health bibliographic databases: PubMed, Cochrane Database of Systematic Reviews and CENTRAL and Web of Science, were searched for relevant literature to date. The search strategy was developed to identify studies which have a direct correlation between “Dentistry” and “Thermography”. Electronic search results were exported into a word spreadsheet and duplicated deleted.
Eligibility Criteria
Dentistry and thermography are distinct concepts, both related and they are the focus of this review. Therefore, papers were included if they satisfied all the following eligibility criteria:
- Population: all the patients that need dentistry treatments.
- Language: Articles publish in English.
- Timeline: No restrictions.
- Type of Study; Case Reports; Classical Article; Clinical Conference; Clinical Study; Clinical Trial (all phases and types); Meta-Analysis; Randomized Controlled Trial, Systematic Review.
- Outcome: articles that used thermography as a means of auxiliary diagnosis or studied objectively and compared thermography in dentistry with other auxiliary means of diagnosis
- Exclusion criteria: review and works that did not comply with this search purpose, as well as dissertations, thesis, and course conclusion work.
Stage 4: Charting the data Eligible papers were independently reviewed, and the following data were extracted: author information (title, author, and year of publication), objectives, study type, number of primary studies included in the review, and the results.
Stages 5 and 6: Collection, summary, and consultation. The PRISMA-ScR guided the collection, interpretation, and communication of results [16]. Following the recommendations by Levac, et al. thematic analysis consisted of (1) analyzing the data, (2) reporting results, and (3) applying meaning to the results [14].
Results
Literature Search
Electronic searches identify 55 articles, resulting in 41
to be screen after excluding the duplicates. (Figure 2). The titles and abstracts were assessed to review following the inclusion criteria, resulting in 17 studies being retained. After full text reading and applying the inclusion criteria 3 were excluded as they did not provide relevant data to relate thermography with dentistry.
Characteristics of Reviewed Studies
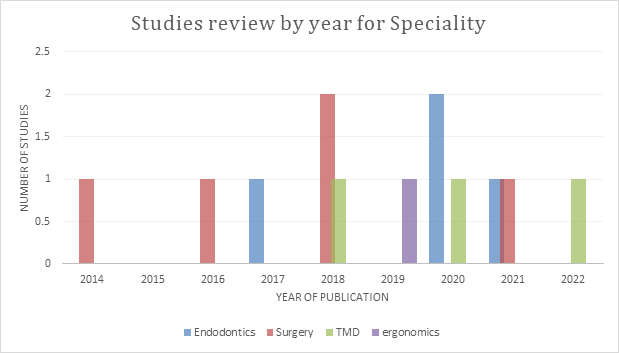
According to the 13 selected studies, in surgery, studies relating this area to thermography have been carried out over the years since 2014. Subsequently, in endodontics, there were more frequent publications of literature in the year 2017, 2020 and 2021. As in temporomandibular disorders studies, thermography studies started in 2018. One ergonomic study was published in 2019. This information is represented in a chart mode in Figure 3.
Type of Reviews
The largest number of studies were in vitro, as observed in Figure 4, followed by clinical trials and fewer systematic reviews and case study.
Evidence Assessment
To assess the evidence of the selected studies the Level of Evidence of Oxford metric was carried out [17] Table 1.
| Study | Level of Evidence | Design | Level of Recommendation |
|---|---|---|---|
| Aboushady, et al. [15] | 3B | Clinical Trial | B |
| Barbosa, et al. [16] | 3B | Clinical Trial | B |
| Lima, et al. [17] | 3B | Clinical Trial | B |
| Melo, et al. [18] | 3A | Sistematic Review | B |
| Harder, et al. [19] | 4 | In Vitro | C |
| Endo, et al. [20] | 4 | Case study | C |
| Cosoroaba, et al. [21] | 3B | Clinical Trial | B |
| Kurt, et al. [22] | 4 | In vitro | C |
| Diegritz, et al. [23] | 4 | In vitro | C |
| Raj, et al. | 4 | In vitro | C |
| Lipski et al | 4 | In vitro | C |
| Mohlhenrich, et al. | 4 | In vitro | C |
| Christensen, et al. | 3B | Clinical Trial | B |
Table 1: Level of evidence of Oxford [17].
| Areas of Dentistry | Year | Author | Type of study | Number of Patients | Objetives | Results |
|---|---|---|---|---|---|---|
| Endodontics | 2021 | Aboushady, et al. | Clinical Trial | n= 80 | To evaluate the effectiveness of thermography for the study of periapical inflammatory lesions and compare them with standard reference radiographs [18]. | Thermography was indicated as effective to be used in the diagnosis of acute pulpitis and apical periodontitis, acute periapical abscess (having a higher temperature than the others), and chronic apical abscess. Thus, it can detect inflammatory reactions during the preclinical phase, leading to early diagnosis [15]. |
| TMD | 2020 | Barbosa, et al. | Clinical Trial | n=86 | Evaluate patients with and without temporomandibular disorders according to differences in thermal radiance in sensitivity and specificity tests and evaluate the thermal asymmetry and the thermal intensity correlating with the intensity of pain on palpation [19]. | The low accuracy of infrared thermography made it difficult to differentiate TMD through thermographic analysis. According to thermal patterns, the intensity of pain on palpation in patients with TMD may be accompanied by a decrease in temperature [16]. |
Table 2: Level of evidence of Oxford [17].
TMD 2022 Lima, et al. Clinical Trial n=78 Review the scientific effectiveness of infrared thermography in the diagnosis of TMDs [20].
TMD 2018 Melo, et al. Sistematic Review n=9 Surgery 2018 Harder, et al. In Vitro Surgery 2018 Endo, et al. Case study n=10 $$ \text{Ergonomics} \mid 2019 \mid \text{Cosoroaba, et al.} \mid \text{Clinical Trial} \mid n=4 $$ Endodontics 2017 Kurt, et al. In vitro n=80 Endodontics 2020 Diegritz, et al. In vitro n=45 The literature still needs an increase in the number of studies on the reliability of Infrared Thermography for the diagnosis of TMDs [17].
The literature still needs an increase in the number of studies on the reliability of Infrared Thermography for the diagnosis of TMDs [18].
Systematically review the scientific effectiveness of infrared thermography in the diagnosis of TMDs [21].
These results suggest that thermography reflects greater acuity of intraosseous temperature change during preparation than thermocouples [19].
To compare the use of thermography and thermocouples to detect changes in intraosseous temperature during implant placement preparation [22].
This study was conducted to assess the usefulness of thermography to quantify facial temperature before and after orthognathic surgery and intermaxillary fixation and the effects of these orthognathic procedures on facial temperature [23].
Thermography was useful for the quantitative assessment of facial temperature in patients undergoing orthognathic surgery. Changes in facial temperature were predominantly due to inflammation after surgery [20].
Stretching exercises can be seen as effective preventive measures to avoid muscle strains caused by wrong working postures, however, more studies with thermography and other methods are needed to reach a definitive conclusion [21].
Evaluate, through thermal imaging, the muscle strain experienced by oral health professionals during work, depending on their position [24].
Appropriate cooling procedures, according to the thermographic data, and fine tungsten carbide burs should be used during the removal of remaining adhesives after debonding the bracket to prevent adverse pulpal reactions [22].
Evaluate changes in pulp area temperature during different cleaning adhesive procedures [25].
The increase in temperature at the root surface during the application of vertical compaction presents considerable variability depending on the filling system, according to the thermographic data [23].
Determine the increase in temperature at the root surface during vertical hot compaction using three different obturation systems [26].
| Surgery | 2021 | Raj,et al. | In vitro | N=72 | Discover a relationship between drilling speed, hand pressure, and coolant temperature to obtain the ideal balance needed, using thermography [27]. | The results indicate that none of the three parameters generated heat above the critical temperature for bone necrosis (47º) [24]. |
|---|---|---|---|---|---|---|
| Endodontics | 2020 | Lipski, et al. | In vitro | N=80 | Measure changes using infrared thermography surface temperature adjacent to the chamber ceiling of premolar teeth extracted from young and old patients [28]. | Dentin had a significant limiting effect on the temperature rise generated during the polymerization of temporary materials, indicating good thermal insulating properties of this tissue [25]. |
| Surgery | 2016 | Mohlhenrich, et al. | In Vitro | N=16 | Determining how bone density affects temperature in artificial bone using a thermographic camera [29]. | Temperature increases with increasing bone density. However, this effect is reduced with increasing drill diameter. This will be important in terms of which tool to use depends on the bone reaction [26]. |
| Surgery | 2014 | Christensen, et al. | Clinical Trial | N=124 | To assess differences in facial temperature after mandibular third molar removal when patients received methylprednisolone and placebo, and to assess the correlation between patient-reported swelling on a visual scale and facial skin temperature measured with thermography [30]. | Thermography does not appear sensitive enough to detect differences in inflammatory responses when patients received methylprednisolone or placebo [27]. |
Table 3: Areas, publication year, author, type of study, number of patients and results of the analyzed studies.
Discussion
The selected studies report that the thermographic examination allows the identification of temperature variations. Some are so subtly that cannot be evidenced by laboratory tests, radiographs among others, thus being a complementary diagnostic method, helping in the identification of several pathologies. It is important to understand that the level of confidence is low, that the literature still needs an increase in the number of studies on the reliability of this technique.
In all cases, it was evidenced that for the performance of thermographic exams it is extremely important to have clinical requirements in thermography in order to obtain standardized images, and with the least interference [18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30]. During the examination, the patient must be positioned relatively equidistant and adequately away from the wall. Before the examination, patients with minor infections around the face should be recorded, such as pimples, among others, as it can interfere with the diagnosis. These structures are called hyperthermic artifacts. Thermography can also be useful to assess temperature changes, monitoring postoperative inflammatory response [23]. It is recommended that, before the examination, the patient´s face should be cleaned to eliminate lotions, creams, powders, deodorants, or antiperspirants in the area to be examined, as they may have a reflexive effect [19].
Thermography can be applied in different medical specialties. Surgery is one of these, explored since 2014. Thermography has been used as an auxiliary diagnostic aid in pre-surgery, during, and after surgery [22, 23, 27, 29, 30]. In pre-surgery and post-surgery Endo et al. (2018), found out that is technique is very useful for evaluating temperature changes in the different stages of post-surgical inflammation [23]. According to Raj, et al. thermography can be used during surgery, to prevent temperature from reaching a value above 47°C, which is the critical temperature for bone necrosis. Also has good accuracy compared to other methods of temperature change, according to Harder, et al. [22, 27].
Regarding endodontics, the interest in this area is more recent and had different approaches. Some studies aimed to confirm the effectiveness of thermography as a pulp diagnosis tool [18, 28]. Other studies have used thermography to monitor temperature changes to maintain the vitality of pulp structures [25, 26]. In temporomandibular disorders, thermography studies started in 2018. For this specialty, this technique has a consensus in the selected studies, both Lima, et al. and Melo, et al. concluded that the literature needs an increase in the number of studies. This could elevate infrared thermography reliability in the diagnose of temporomandibular disorders to another level [20, 21]. Barbosa, et al. demonstrated the low accuracy of this technique, with a decrease in temperature in patients with pain on palpation [19].
One ergonomic study published in 2019 stated that this technique could also be important in the study of ergonomic control of health professionals. Cosoroaba, et al. report that this approach could become a complement to other study methods for muscle strains [24].
Thermography is a promising technique that, after being implemented robustly in the market, will become an asset on dentistry. Being an easy-to-use technique, without ionizing radiation, it could be used in more clinical studies as a complement to other diagnostic methods in different clinical areas. However, great care is needed in the handling of this technique, since any thermal alteration may cause errors in the reading and consequently in the diagnosis, so the professional must be trained to use this method and should only use it as a complementary means of diagnosis [31, 32, 33, 34]. At this stage, as a novel technique, it needs more robustness, and more studies to prove its effectiveness, mostly in temporomandibular disorders.
This technique will contribute to an earlier and more accurate diagnosis in some endodontic treatments. Since many of these studies are in vitro, it would be of great importance to carry out studies at a clinical level in the future, using this method to complement the clinical routine and register the added value in contribution and comparison with other diagnostic methods, such as radiographs and sensitivity tests. This method is also an asset in the diagnosis and prognosis of teeth fractures or vertical cracks, at an early level, so it would also be important to carry out clinical studies in patients with this indication. At a surgical level, this procedure has already demonstrated its effectiveness in controlling temperature to reduce the possibility of bone necrosis and cell apoptosis, keeping temperature below 47ºC, which could be of help in increasing the rate of success on osteotomies and implants placement.
Conclusion
Studies suggest that it may have applicability in dentistry. It is expected that thermography will contribute to the expansion of knowledge as an asset in various pathologies in addition to other diagnostic tools, as in pulpitis diagnose, during hard tissue removal, controlling the temperature in dental procedures, osteotomies and implant placement, as well as in the post-surgical evaluation, apprising post- surgical edema. Being a very novel technique, it is important to increase the number of studies to enhance its reliability.
References
-
Sikdar SD, Khandelwal A, Ghom S, Diwan R, Debta FM (2010) Thermography: a New diagnostic tool in Dentistry. Journal of Indian Academy of Oral Medicine and Radiologu 22(4) 206-210.
-
Berz R, Sauer H (2007) The Medical Use of Infrared- Thermography History and Recent Applications. Thermografie-Kolloquium, pp: 1-12.
-
Lahiri BB, Bagavathiappan S, Jayakymar T, Philip J (2012) Medical applications of infrared thermography: A review. Infrared Physics & Technology 55(4): 221-235.
-
Anbar M (1985) Diagnostic: thermal imaging: A historical techonological perspective. Dynamic: Telethermography in Medical Diagnosis pp: 1-9.
-
Anbar M (1987) Computerized Thermography. The Emergence of a Diagnostic Imaging Modality. Int J Technol Assess Health Care 3(4): 612-621.
-
Harshavardhan T, Vijayalaxmi N, Mudavath M, Meesaka D (2017) Thermography: A Newer Diagnostic Assessment Tool in Dentistry. Journal od Mahatma Gandhi Institute of Medical Sciences, 22(2): 87-91.
-
Lin M, Liu QD, Kim T, Xu F, Bai BF, et al. (2010) A new method for characterization of thermal properties of human enamel and dentine: Influence of microstructure. Infrared Physics & Technology 53(6): 457-463.
-
Linsuwanont P, Palamara JE, Messer HH (2007) An investigation of thermal stimulation in intact teeth. Archives of Oral Biology 52(3): 218-227.
-
Oskui Z, Ashtiani MN, Hashemi A (2013) Thermal analysis of the intact mandibular premolar: a finite element analysis. Int Endod J 46(9): 841-846.
-
Kells BE, Kennedy JG, Biagioni PA (2000) Computerized infrared thermographic imaging and pulpal blood flow: Part 1. A protocol for thermal imaging of human teeth. Int Endod J 33(5): 442-447.
-
Howell RM, Duell RC, Mullaney TP (1970) The determination of pulp vitality by thermographic means using cholesteric liquid crystals: a preliminary study. Oral Surg Oral Med Oral Pathol 29(5): 763-768.
-
Gopikrishna V, Pradeep G, Venkateshbabu N (2009) Assessment of pulp vitality: a review. Int J Paediatr Dent 19(1): 3-15.
-
Pogrel MA, Yen CK, Taylor RC (1989) Studies in tooth crown temperature gradients with the use of infrared thermography. Oral Surg Oral Med Oral Pathol 67(5): 583-587.
-
Levac D, Colquhoun H, Brien KkO (2010) Scoping studies: advancing the methodology. Implement Sci 5: 69.
-
Arksey H, Malley LO (2005) Scoping studies: towards a methodological framework Int J Soc Res Methodol 8: 19- 32.
-
Tricco A, Lillie E, Zarin W, Brien KKO, Colquhoun H (2018) PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 169(7): 467- 473.
-
Howick I, Chalmers P, Glasziou and Greenhalgh (2022) The 2011 Oxford CEBM Level of Evidence. http://www. cebm.net/ index.aspx?o=5653 (accessed on 2 June 2022)..
-
Aboushady MA, Talaat W, Hamdoon Z, Elshazly TM, Ragy N (2021) Thermography as a non-ionizing quantitative tool for diagnosing periapical inflammatory lesions. BMC Oral Health 21(1): 260.
-
Barbosa S, Amorim A, Arruda M, Medeiros GBS, Freitas A, et al. (2020) Infrared thermography assessment of patients with temporomandibular disorders. Dentomaxillofac Radiol 49(4): 20190392.
-
Lima ED, Paulino JAS, Freitas APLF, Ferreira JEV, Amorim A, et al. (2022) Artificial intelligence and infrared thermography as auxiliary tools in the diagnosis of temporomandibular disorder. Dentomaxillofac Radiol 51(2): 20210318.
-
Melo DP, Bento PM, Peixoto LR, Martins SKLD, Martins CC (2019) Is infrared thermography effective in the diagnosis of temporomandibular disorders? A systematic review. Oral Surg Oral Med Oral Pathol Oral Radiol 127(2): 185-192.
-
Harder S, Egert C, Freitag Wolf S, Mehl C, Kern M (2018) Intraosseous Temperature Changes During Implant Site Preparation: _In Vitro_ Comparison of Thermocouples and Infrared Thermography. Int J Oral Maxillofac Implants 33(1): 72-78.
-
Endo T, Komatsuzaki A, Miyagawa Y, Kamoda T, Goto S, et al. (2019) Thermographic assessment of facial temperature in patients undergoing orthognathic surgery. J Oral Sci 61(2): 321-326.
-
Cosoroaba R, Cirin L, Anghel MD, Talpos Niculescu CI, Argesanu V, et al. (2019) The use of thermal imaging in evaluating musculoskeletal disorders in dentists. J Med Life 12(3): 247-252.
-
Kurt G, Gul N, Er O (2017) Thermal imaging of the pulp during residual adhesive removal. J Orofac Orthoped 78(4): 330-337.
-
Diegritz C, Gerlitzki O, Fotiadou C, Folwaczny M (2020) Temperature changes on the root surface during application of warm vertical compaction using three different obturation units. Odontol 108(3): 358-365.
-
Raj R, Manju V, Kumar Gopal V, Eswar M (2021) Analysis of Factors Determining Thermal Changes at Osteotomy Site in Dental Implant Placement-An _In-Vitro_ Study. J Clin Exp Dent 13(2): 2021.
-
Lipski K, Woźniak L, Szyszka Sommerfeld, Borawski M, Droździk A, Nowicka A (2020) _In Vitro_ Infrared Thermographic Assessment of Temperature Change in the Pulp Chamber during Provisionalization: Effect of Remaining Dentin Thickness. Journal of Healthcare Engineering.
-
Möhlhenrich SC, Abouridouane M, Heussen N, Modabber A, Klocke F, et al. (2016) Influence of bone density and implant drill diameter on the resulting axial force and temperature development in implant burs and artificial bone: an _in vitro_ study. Oral Maxillofac Surg 20(2): 135- 142.
-
Christensen J, Matzen LH, Søren S, Væth M, Wenzel A (2014) Is thermography useful for assessment of postoperative inflammation after surgical removal of mandibular third molars when methylprednisolone is administered and how does it correlate with patients’ perception of swelling?. J Oral Maxillofac Surg 72(3): 463-469.
-
Kells BE, Kennedy JG, Biagioni PA, Lamey PJ (2000) Computerized infrared thermographic imaging and pulpal blood flow: Part 2. Rewarming of healthy human teeth following a controlled cold stimulus. Int Endod J 33(5): 448-462.
-
Gratt BM, Anbar M (1998) Thermology and facial telethermography: Part II. Current and future clinical applications in dentistry. Dentomaxillofac Radiol 27(2): 68-74.
-
Gratt BM, Radford SBG, Shetty V, Solberg WK, Sickles EA (1996) A 6-year clinical assessment of electronic facial thermography. Dentomaxillofac Radiol 25(5): 247-255.
-
Cummings M, Biagioni P, Lamey PJ, Burden DJ (1999) Thermal image analysis of electrothermal debonding of ceramic brackets: an _in vitro_ study. Eur J Orthod 21(2): 111-118.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells