Conservative Management of Large Trauma-Related Periapical Lesion: Case Report
Dental trauma is a serious health problem affecting the teeth and the general health as well. Sometimes, the traumatized tooth may end up with vitality loss. The possible consequences of pulp necrosis could be osteolytic lesions and radicular cysts. This case study reported a successful conservative non-surgical endodontic management of a massive trauma-related periapical lesion in a child 13-year-old.
Introduction
Dental trauma has a great impact on the person’s health and the quality of life as well [1]. The severe injury may result in fracturing the tooth with possible pulp and bone necrosis Yu H, et al. [2], Sometimes, the secondary infection and periodontal inflammation might induce division and proliferation of epithelial cell rests of Malassez to form radicular cyst Lin LM, et al. [3]; the latter is the most common of all cysts affecting the jaw, and considered an osteolytic and not self-sustaining lesion. Therefore, the radicular cysts with small size can be treated successfully using endodontic therapy and enucleation, while the larger one necessitates decompression or marsupialization; the recurrence is rare because of its inflammatory nature [4, 5, 6, 7, 8]. This case report presented a conservative endodontic approach of a massive periapical lesion correlated to dental trauma.
Case History
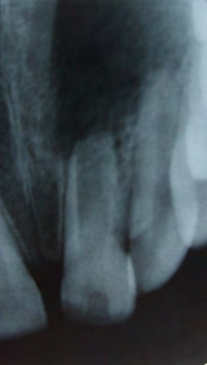
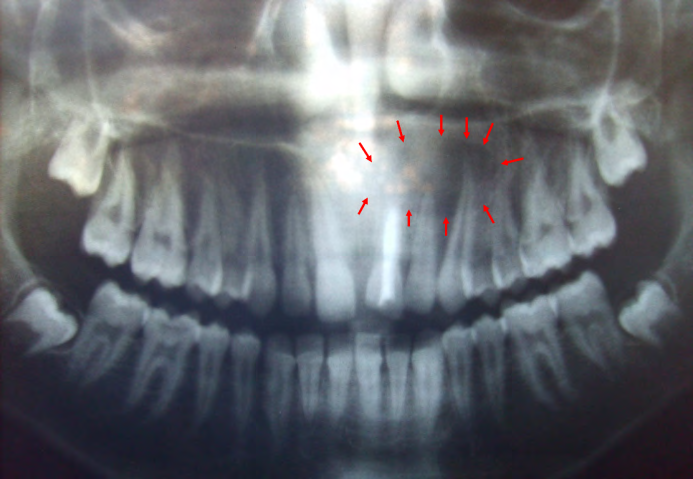
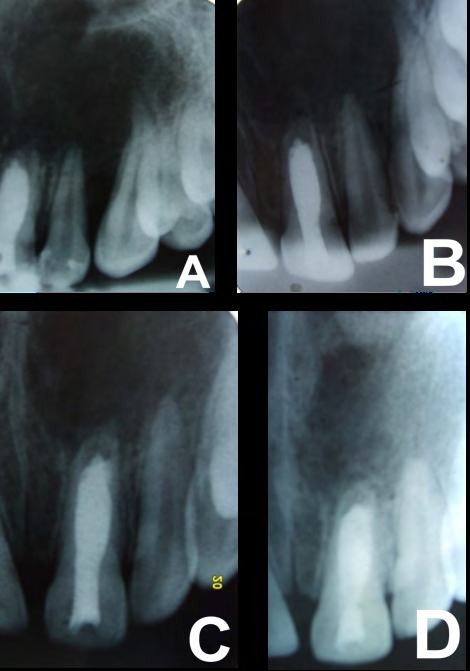
A female healthy child, 13 years old, presented with the parents to paediatric dental clinic to “check swollen gum inside the mouth and repair broken front tooth”. Clinical dental examination revealed an upper left central incisor 21 with enamel-dentin-pulp fracture accompanied with a noticeable mobility; the trauma took place five years ago and they had not sought any dental treatment thereafter because the child was very apprehensive and fearful; recently, there was an increasing swelling in the hard palate discharging yellow secretions through the gingival sulcus of the upper left first premolar 24. The pulp test, using Endo Ice spray (-50°), revealed that the teeth 11, 22, 23, 24, 25 were vital, while the tooth 21 was negative. Radiographic examination using orthopantomography and periapical radiographs showed a complicated crown fracture of the tooth 21 accompanied with arrested root development and open apex, in addition to a huge oval bone radiolucency measuring around 25mm with defined borders which seemed to be a radicular cyst extended from 21 to the area of upper left second premolar 25, (Figures 1 & 2). The parents and the child were advised that the tooth 21 could be saved, and the treatment steps were discussed in detail, then an informed consent had been obtained before treatment. In the first session, the root canal was debrided gently using H-file size 50#, and thoroughly rinsed with saline to allow for freely discharging of the secretions through the pulp chamber; after that, the canal was irrigated using sodium hypochlorite 5%, and then with saline as a final irrigation; once the root canal was almost dry, Calcium Hydroxide (CH) dressing paste with PH=12.5 was inserted using Lentulo Spiral size 30# and condensed inside the canal using wet cotton pellets and paper points, then the orifice was closed with temporary filling, an antibiotic Augmentin 457mg/5ml was prescribed orally for seven days to control the infection. After one week, the same procedure for applying CH intracanal dressing was repeated, and the fractured part of the tooth 21 was restored using composite restoration, only limited palatal access was maintained using temporary filling for subsequent endodontic therapy. After one month, CH dressing was reinserted again, the secretions coming through the gingival sulcus of 24 completely disappeared and the palatal swelling started to diminish. After that, CH intracanal dressing was repeated periodically every two months; a successful apexification along with noticeable bone regeneration could be clearly recognized on periapical radiograph after eight months, (Figure 3).
Discussion
Dental trauma is a serious health problem affecting the person’s life and community as well [9]. This case study reported the consequences of a dental injury left untreated for five years; the resulted massive periapical osteolytic lesion with remarkable radiopaque borders is very compatible with an infected radicular cyst [4]. This estimated diagnosis was not confirmed by a histological examination as the treatment was carried out endodontically without any surgical intervention. The fractured tooth 21 was early restored with composite at the second session, this in turn helped the child regained the smile and accepted the long observation and treatment period with a great cooperation. Subsequent visits were maintained regularly to assess the healing process, and Calcium Hydroxide intracanal dressing was repeated periodically aiming for disinfecting the lesion and repairing [6].
Interestingly, this case report is distinguished by the conservative non-surgical endodontic therapy of a massive periapical lesion, resulted in noticeable bone regeneration along with successful apexification. On the other hand, most studies depended on enucleation, marsupialization or decompression of the radicular cyst accompanied with endodontic therapy of the infected tooth [4, 5, 6, 7, 8]. Indeed, the decompression and drainage in this case report were achieved endodontically through the wide root canal of an immature central incisor with open apex, even without delivering any type of anaesthesia; this in turn motivated the child and eliminated the dental phobia which was the main cause for refraining from any dental intervention within five years after injury. However, there are many limitations in this case report; including the only use of two-dimensional radiographs for diagnosis without going further to cone beam computed tomography CBCT through which a comprehensive radiographic detail can be obtained; Indeed, no clinical photographs were revealed in response to the desire of the parents to publish only radiographs, also no histological examination was carried out due to the non-surgical intervention, which is crucial to outline the differential diagnosis of large periapical lesions; in addition, the goal of endodontic treatment in this case report was apexification while other studies aimed for regenerative endodontics which is far better for the long term results, root length, and strength Abu Zeid ST, et al. [10], Corbella S, et al. [11] finally, the observation period was very limited to assess the healing process of such massive periapical lesion.
Conclusion
In a conclusion, within the limitations of this case report, the conservative endodontic approach might be of great benefit for the treatment of large periapical lesions without the complications, stress, and cost of surgical intervention; this in turn will make the dental procedure easier and more favourable.
References
-
Nowosielska M, Baginska J, Kobus A, Kierklo A (2022) How to Educate the Public about Dental Trauma-A Scoping Review. Int J Environ Res Public Health 19(4): 2479.
-
Yu H, Zhu H (2021) The management of a complicated crown-root fracture incorporating modified crown- lengthening surgery. Br Dent J 230(4): 217-222.
-
Lin LM, Huang GT, Rosenberg PA (2007) Proliferation of epithelial cell rests, formation of apical cysts, and regression of apical cysts after periapical wound healing. J Endod 33(8): 908-916.
-
Lin LM, Ricucci D, Kahler B (2017) Radicular Cysts Review. JSM Dent Surg 2(2): 1017.
-
Penumatsa NV, Nallanchakrava S, Muppa R, Dandempally A, Panthula P (2013) Conservative approach in the management of radicular cyst in a child: case report. Case Rep Dent 2013: 123148.
-
Kadam NS, Ataide I, Raghava P, Fernandes M, Hede R (2014) Management of large radicular cyst by conservative surgical approach: a case report. J Clin Diagn Res 8(2): 239-241.
-
Chybicki D, Lewandowska ML, Gruda MR, Naze AJ (2020) Massive Radicular Cyst in the Maxillary Sinus as a Result of Deciduous Molar Tooth Pulp Necrosis. Case Rep Dent V: 2020.
-
Koju S, Chaurasia NK, Marla V, Niroula D, Poudel P (2019) Radicular cyst of the anterior maxilla: an insight into the most common inflammatory cyst of the jaws. J Dent Res Rev 6(1): 26-29.
-
Lam R (2016) Epidemiology and outcomes of traumatic dental injuries: a review of the literature. Aust Dent J 61: 4-20.
-
Abu Zeid ST, Alamoudi RA, Alothmani OS, Mokeem Saleh AA, Siddiqui AYA (2021) Prospective Study of Long- Term Regenerative Endodontics Outcomes of Necrotic Immature Permanent Teeth: An 8-Year Follow-Up. Healthcare (Basel) 9(12): 1670.
-
Corbella S, Ferrara G, El Kabbaney A, Taschieri S (2014) Apexification, apexogenesis and regenerative endodontic procedures: a review of the literature. Minerva stomatologica 63(11-12): 375-389.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells