Systematic Review-Adverse Effects of Silver Diamine Fluoride
Purpose: To conduct a systematic review of the literature regarding the possible adverse systemic and oral effects of silver diamine fluoride (SDF) when used as a therapeutic agent for arresting caries in deciduous and permanent teeth in children and adolescents. Methods: A digital search of the adverse effects of SDF was conducted on November 25,2020 without date of publication restraints. The data was updated in February 2022 with no additional significant findings. The search was conducted using PubMed, Scopus, Cochrane Library via Wiley, EMBASE, LILACS, Biological Science Index, OpenGrey, Grey Literature Report, Dissertations and Theses, ClinicalTrials.gov, and International Clinical Trials Registry Platform. Results: The initial digital and manual systematic literature search found a total of 493 articles; after the removal of duplicates and other publications, a total of 6 publications were included in this systematic review: 3 randomized controlled trials, 2 clinical trials, and 1 ex-vivo study. SDF application was accompanied by black staining of the tooth in all six studies. There were no reports that SDF caused serious systemic illness or oral injury based on this systematic review.
Clinical Significance
Even though systematic reviews have confirmed the efficacy of SDF in arresting and preventing caries, there are no known systematic reviews on related adverse effects, critical information when making clinical decisions. This systematic review affirms the safety of SDF and supports its use for caries arrest on patients under 18 years old. This would effectively reduce the high prevalence of early childhood caries, [1] even more so in disadvantaged communities where the prevalence remains disproportionately high [2, 3].
Introduction
Silver Diamine fluoride (SDF) has been used as a therapeutic agent for arresting caries in deciduous and permanent teeth since the 1970’s [4]. This product was developed in the late 1960s, when ammonia was added to silver nitrate to make it stable for use as an antibacterial agent to prevent and treat dental caries [5]. The U.S. Food and Drug Administration (FDA) approved the use of SDF
as a desensitizing agent in 2014 [6]. In the United States, currently, SDF is used off-label for caries arrest. Although not officially FDA approved for caries arrest in the United States, in 2016 SDF was awarded breakthrough therapy status by the FDA [7]. For decades, SDF has been used around the world for caries management due to its economic benefits and ease of use with children, the elderly, and in disadvantaged communities with difficult access to dental care [8, 9]. Silver diamine fluoride (SDF) at a concentration of 38% (44,800 ppm fluoride) is the highest concentration among fluoride agents used in dental practice and the only concentration available in the US [10, 11]. Due to the high concentrations of fluoride and silver, adverse effects of SDF are of concern regarding its use in young children. It has been thought that silver ions have low cell toxicity, but the oxidation of ionized silver into metallic silver has been the most obvious adverse effect of SDF, causing the black staining effect on carious tissue and limiting its use in aesthetically demanding patients [5, 12, 13]. A range of SDF products exist on the market and some products include a second step application that can reduce staining caused by SDF alone to varying degrees, while others have an aqueous based solution to create a more neutral pH [14].
Although several systematic reviews have been conducted on the beneficial effects of SDF as a caries arresting agent, no systematic review has been conducted describing the possible adverse health effects of SDF. The purpose of this report is to provide a systematic review of the evidence regarding the potential adverse effects of SDF when used to arrest caries on deciduous or permanent teeth in children and adolescents.
Materials and Methods
Search Strategy
This systematic review was performed using the Preferred Reporting Items for Systematic Reviews and Meta- Analysis statement (PRISMA). PRISMA is an evidence-based minimum set of items for reporting in systematic reviews and meta-analyses. PRISMA primarily focuses on the reporting of reviews evaluating the effects of interventions but can also be used as a basis for reporting systematic reviews with objectives other than evaluating interventions (e.g., evaluating etiology, prevalence, diagnosis, or prognosis).
Inclusion Criteria
Published randomized and non-randomized human clinical trials, pilot studies, and ex-vivo studies of adverse systemic or local effects of SDF used as a caries arresting medicament or as part of a restorative or non-restorative option in permanent or primary teeth in children and adolescents under 18 years of age. Studies with adverse effects as the primary or secondary outcome were included.
Exclusion Criteria
Systematic reviews, metanalysis, retrospective studies or case reports; in vitro studies, animal studies, or use of SDF for caries prevention only, or in conjunction with other fluorides, or patients 18 years of age or older. Studies on parental acceptance of SDF without discussion of adverse effects were excluded.
Search
An electronic search was performed on November 25, 2020, using the search terms SDF, children, and adverse effects. Synonyms for each search term were identified using both keywords and indexing terms. The databases searched were PubMed (including MEDLINE), Scopus, Cochrane Library via Wiley (including CENTRAL), EMBASE via Elsevier, LILACS, Biological Science Index via ProQuest, OpenGrey, Grey Literature Report, ProQuest Dissertations & Theses, ClinicalTrials.gov, and International Clinical Trials Registry Platform via WHO (Appendix 1). A manual search of 3 specific journals was also conducted and two experts were consulted for suggestions on additional articles of interest to include. The initial search, conducted on November 25, 2020, had no constraints on date of publication. The collected articles were uploaded to a core database using End note X7 (Thomson Reuters, San Francisco, CA, USA), and duplicates were removed. The data was subsequently updated in February 2022.
Data Collection
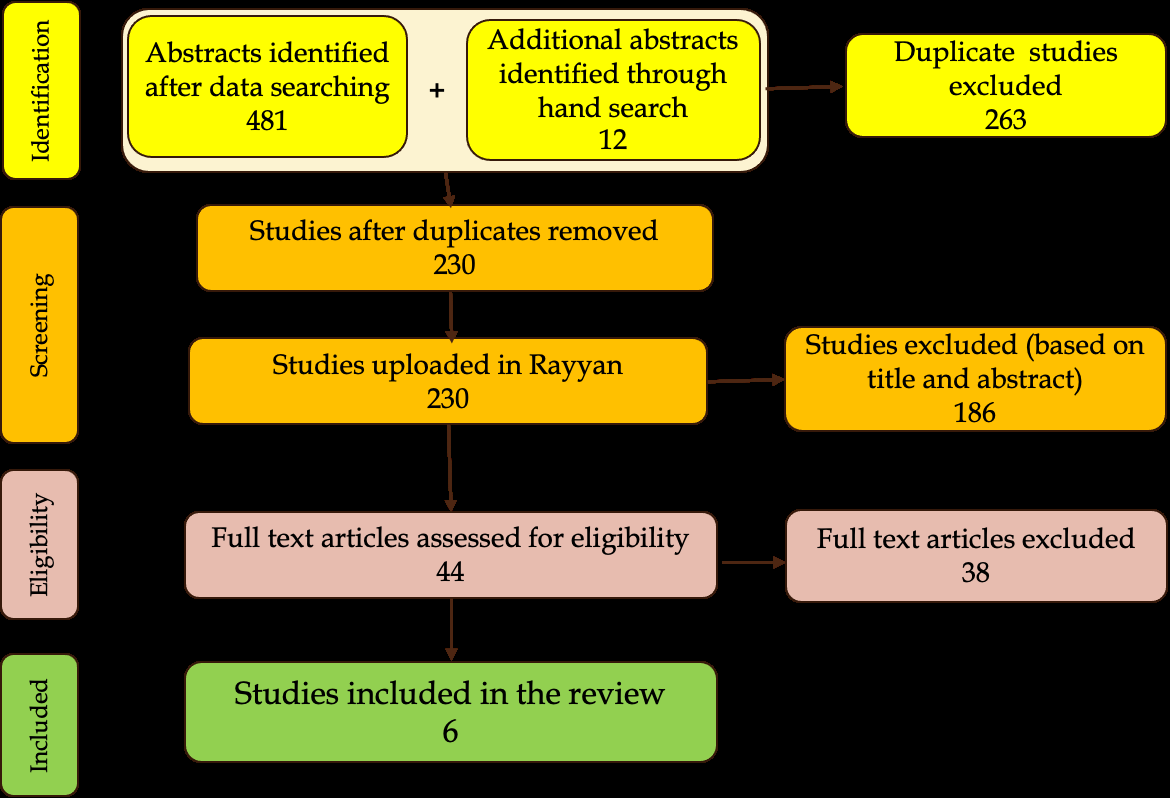
The de-duplicated articles were then uploaded to Rayyan—a web and mobile app for systematic reviews [15]. The titles and abstracts of the de-duplicated articles were then screened by two of the authors who independently sorted them into include, exclude, and maybe categories based on the eligibility criteria. Conflicts in these entries were resolved by a third author, to create the final list of included articles based on titles and abstracts. The full texts of these included articles were screened by two other authors who once again sorted them into include, exclude, and maybe categories. Studies in languages other than English had the data extracted with the help of individuals knowledgeable in those languages. We attempted to contact study authors to obtain missing or unclear information. Studies related to SDF and parental acceptance were included only if they also provided data on adverse effects also. Conflicts in the screening were resolved by an independent author to select the final list of included articles. All included articles in the final list were read by all reviewers and independently assessed for relevance to our original inclusion criteria. All information was tabulated in a flowchart representing the methods used to arrive to conclusions (Figure 1).
Results
The initial electronic literature search found a total of 481 potentially eligible publications. 67 were found in PubMed, 80 were found through Scopus, 39 via Wiley (including Central) in Cochrane Library, 71 in Embase via Elsevier, 28 in LILACS, 99 in Biological Science Index via ProQuest, 8 ProQuest’s Dissertations and Thesis, 38 ClinicalTrials.gov, and 51 in International Clinical Trials Registry. A manual search was also conducted, and 12 publications were added to the search results. Next, 263 duplicated publications were removed. The resulting 230 publications were manually screened for appropriateness, based on title, keywords, and abstract. After screening the titles and abstracts, 186 publications were excluded. The full texts of the remaining 44 publications were then manually reviewed, and 38 publications were excluded based on the inclusion and exclusion criteria [6, 16, 17, 18, 19, 20, 21]. studies were included in this systematic review. A flow chart of the selection criteria is shown in Figure 1.
| for header rows | for data cells | for header rows | for data cells | ||
|---|---|---|---|---|---|
| Authors | Study Type | Study Population | Evaluation Methods/Duration | Control | Study Results |
| Clemens, et al. [16] | Clinical trial | 32 children, 2-5 years old with a total of 118 carious lesions. | 4 -item, 5-level Likert-scale questionnaire to parents 2-3 weeks after 38% SDF application. | N/A | There was no correlation between the children’s behavior during application and parents’ acceptance. High level of agreement in responses. |
| Duangthip, et al. [17] | Stratified-randomized clinical trial | 888 Children, 3-4 years old with a total of 4220 carious surfaces. | Parental questionnaire, 1-week, and then after 6,12,18,24,30 months after placement of 38% SDF. Acute adverse effects were to be self-reported. | 12% SDF/annually or biannually | Self-reported: Tooth or gum pain (3.7-7.0%), gum bleaching (3-5.7%), gum swelling (1.5-2.9%). Common: caries staining. No systemic illness or acute toxicity observed including nausea, vomiting, or generalized discomfort. |
| Hiremath, et al. [18] | Pilot clinical study | 42 children between the ages of 12-16 years | The children were given a children oral health impact profile (COHIP-SF) immediately and 4 months after application of 38% SDF to assess the OHRQol of children. | A baseline children oral health impact profile (COHIP-SF) English version | Emotional well-being scores were significantly different at any of the follow-ups (immediately or 4-months after application of SDF). 85.7% of the children did not want to experience SDF again as they were uncomfortable with the metallic taste of SDF and the blackish discoloration of teeth. |
| Milgrom, et al. [19] | Randomized controlled trial | 66 preschool children with a total of 64 treated teeth. (35 -SDF; 29-placebo) | Silver diamine fluoride (38%) applied topically to the lesion. 1) Within 24-48 hours of treatment, telephone contact was made. 2) At the follow up visit 14-21 days later, the gingival and oral tissues were inspected for inflammation or ulcerative lesions and were characterized as mild or severe; localized or generalized. | Placebo: Non-fluoridated sterile water with a blue tint | 1) Within 48 hours, 8 adverse events were reported—4 in the intervention group and 4 in the placebo group—giving no statistical differences by treatment. The majority of adverse events were mild diarrhea or stomachache which resolved in 2-4 days. No tooth pain was reported in any group, despite deep lesions. One child reported a non-sore, non-irritated spot at the corner of the mouth that resolved before the 14-day visit 2). No gingival or mucosal irritation was observed at follow-up in any patient. |
| Rossi, et al. [20] | Ex-Vivo | 8 primary carious teeth previously treated with 38% SDF. | a) 4 teeth were cut histologically for evaluation by scanning electron microscope (SEM) of which one was examined by an energy dispersive X-ray detector (EDS) to determine qualitative and quantitative composition, and (b) 4 teeth were decalcified s and studied under brightfield optical microscopy (OM) | In each histological analysis of human teeth, (ex vivo) the zone opposite the treated lesion was used as control. | SEM on ex vivo teeth showed areas of hypomineralization in the intertubular dentin and few blocked tubules, while EDS detected silver in the center of the lesion, with concentration declining to the edges. OM showed SDF sealing the tubules only at the site it had been placed, with limited penetration beneath, the tubules appeared normal, and the associated pulp tissue showed chronic inflammatory infiltrate and formation of tertiary dentin and no Ag precipitate. The conclusion being minimal adverse effects. |
Table 1: Summary of included studies.
| Vollu, et al.[21] | Randomized controlled clinical trial | 68 children, , 2–5 years old, with active caries on occlusal surface of primary molars | Following recordings were made: i) time required for treatment/ per tooth ii) anxiety: recorded via a facial image scale iii) any complaints of pain, sensitivity, possible irritations, lesions, spots, tattoos on mucosa, gingiva, and skin registered by operator immediately after treatment iv) caregiver interview 2 days after the treatment. v) Quality of life information was obtained using the B-ECOHIS questionnaire before and 15 days post- treatment. | Atraumatic restorative material- glass ionomer Ketac Molar Easy Mix 3 M | Whitish spot on the gingiva, staining or mildly painful white lesion on the tongue or marginal gum that resolved within 2 days. |
|---|
Table 2: Summary of included studies.
Of the 6 papers included, there were 3 randomized controlled trials, 1 clinical trial, 1 pilot clinical trial, and 1 ex- vivo study.
Five of the 6 studies involved surveys (Appendix 1); 3 of the studies were entirely survey based. Only 1 of the 3 survey-based studies surveyed children; the others surveyed parents or their care givers. Of the 6 studies, adverse effect was the primary outcome studied in only 1 study Duangthip, et al. [17]. In 3 investigations Clemens, et al. [16] Milgrom, et al. [19] and Vollu, et al. [21], the primary outcome studied was caries arrest, and not adverse effects of SDF.
One trial compared SDF to glass ionomer restorations Vollu, et al. [21] and one trial used blue tinted water as a placebo Milgrom, et al. [19]. Three trials compared the use of SDF to no other treatments Clemens, et al. [16] Hiremath, et al. [18] and Rossi, et al. [20].
The adverse effects of SDF application were classified into i) Oral including tooth pain, ii) Staining, and iii) Systemic illness and toxicity.
Intraoral
In one study by Vollu, et al. [16] adverse effects reported by parents and caregivers were no different between the SDF treated group and those treated with atraumatic restorative treatment (ART). During the treatment appointment, the operator registered 24 events, (i.e., 29.4% from the SDF treated group and 33.3% from ART group). In this study, staining or mildly painful white lesions in the tongue or marginal gingiva were the more prevalent adverse events, which usually resolved within 2 days after treatment.
In the study by Duangthip, et al. [17] data was collected on adverse effects of SDF via parental questionnaires and self-reported information. This stratified randomized clinical trial included 888 children and 2260 carious surfaces. Similar number of parents (6.6%) reported tooth pain when SDF was placed or when saline was placed as a placebo. Transient gingival swelling (2.8%), and gingival bleaching (4.7%) were seldom reported, and if reported did not last beyond 2 days. In the study by Milgrom, et al. [19] 1 child in a group of 30 children treated with SDF was described as having a non-sore, non-irritated spot at the corner of the mouth, consistent with a silver burn, which resolved within 2 days. No participant in that group was identified with gingival or soft tissue stomatitis or ulcerative lesions.
Staining
Tooth staining was the most reported side effect of SDF. The level of staining depended on the severity of caries, the concentration of the SDF, and/or the frequency with which the SDF was applied. In their study, Duangthip, et al. [17] reported that lesions in children receiving 38% SDF rather than 12% SDF as well as lesions treated semiannually rather than annually had a higher chance of becoming stained black.
When compared with those treated with 12% SDF, lesions in children receiving 38% SDF had a higher chance of becoming stained black (odds ratio [OR], 3.29; 95%CI, 2.84 to 3.81; P<0.001). Lesions treated semiannually had a higher chance of becoming stained black than those treated annually (OR, 1.69; 95%CI, 1.46 to 1.95; P<0.001).
In the conducted in Hongkong by Duangthip, et al. [17] surveys showed that parents were highly accepting of the results of SDF treatment on their children. Another study by Clemens, et al. [16] reported 86.6% agreement among the parents in terms of parental acceptance of SDF.
In a study by Hiremath, et al. [18] conducted on the effect of tooth staining by SDF on the psychological wellbeing of the HIV+ children pediatric patient and their acceptance of the staining, oral health and functional wellbeing dimensions were not significantly different at any of the follow ups, but emotional wellbeing scores were significantly poorer immediately following SDF application compared to 4 months and baseline (P < 0.05). Most study subjects (85.7%) reported that they did not want to experience SDF again due to the discoloration and metallic taste.
Systemic Illness and Toxicity
A stratified randomized review by Duangthip, et al. [17] including 888 kindergarten children, reported no cases of acute toxicity or systemic illness or related symptoms including vomiting and nausea.
In the study by Milgrom, et al. [19] 2 out of 25 children reported adverse systemic effects: 1 child reported nausea, vomiting, stomachache, and diarrhea and 1 child reported nausea and stomachache. In the same study, 3 out of 26 of the placebo group participants reported similar symptoms and there were no statistically significant differences between the SDF and placebo groups. These symptoms were described as mild in severity, probably not related to the SDF application, and resolved within 48hrs of reporting.
Risk of Bias
The risk of bias was determined to be low in only two of the randomized clinical trials Milgrom, et al. [19] Vollu, et al. [21]. In these studies, the operators and examiners had been calibrated and caregivers were followed up with calls and surveys up to two days post application. The study by Rossi, et al. [20] was an ex-vivo study and the study by Duangthip, et al. [17] was a stratified randomized clinical trial in which the adverse effects were based on self-reporting or surveys Hence the risk of bias was considered moderate in these two studies. Of the remaining two studies with a small sample size, one was a pilot study Hiremath, et al. [18] and the other Clemens, et al. [16] had a single examiner and the authors hypothesized that there may have been perceived pressure on the parents to respond positively. These two were considered at high risk for bias.
Discussion
There have been no systematic reviews to date with the primary aim of studying the adverse effects of SDF. However, several systematic reviews have studied caries prevention and arrest related to SDF, a few including adverse effects.
This review focuses on studies involving the adverse effects of SDF on the oral tissues, systemic health, and overall well-being of children and adolescents less than 18 years of age. The search was conducted on November 25, 2020, with no constraints on date of publication. The data was updated in February 2022, with no added significant findings.
In this review, we found the adverse reactions reported in the 6 trials were mild to moderate with few reactions. Even these were short-term and considered possibly unrelated to the application of SDF. The adverse events reported included tooth, gingiva, or tongue pain, gingival bleaching or swelling, mild diarrhea or stomachache, metallic taste, and discoloration. Tooth staining was the most reported adverse effect with an impact on parental acceptability and emotional quality of life of the child. Except for discoloration, adverse events resolved within a few days or by the time of follow up.
Intraoral and Tooth Pain
Two of the studies included in this review Milgrom, et al. [19] and Vollu, et al. [21] reported that any minor gingival irritation or sores resolved within 2 days. This is consistent with a prospective controlled clinical trial [22] conducted on the efficacy of a 38% SDF solution for caries reduction in 425 six-year-old children in which small, reversible, mildly painful white lesions were found in the oral mucosa in 3 of the children through inadvertent contact with SDF solution. These reversible lesions disappeared within 48 hrs without treatment. In another prospective controlled clinical trial [23] conducted on 375 children, no side effects were noted. In a separate paper [24] highlighting the best evidence from systematic reviews and clinical trials on the use of SDF in children, the authors reported no children exhibited negative reactions to the treatment, nor adverse pulpal responses, and only 0.1 percent of children noted slight gingival irritation.
In another randomized clinical trial [25] 108 permanent first molars with deep occlusal cavitated carious lesions in 49 children, aged 6 through 9 years, were treated with SDF plus Potassium Iodide, SDF, and Resin Modified Glass Ionomer Cement. The study reported no clinically significant differences in postoperative pain, clinical abscess or tooth vitality at 3 months, 6 months and one-year.
In summary, intraoral adverse reactions from SDF application are at most mild too moderate, and some of these were possibly unrelated to the application of SDF. Even these dental, gingival, or mucosal reactions resolved within 48 hours.
Staining
The vast majority (76.3 %) of 38% SDF semiannually treated lesions were arrested and stained black at the 30-month follow-up Duangthip, et al. [17]. This study, conducted in Hong Kong, determined that parents were highly accepting of the results of SDF treatment on their children. In one systematic review [26] conducted in 2018, parental acceptances with children’s dental appearance and dental health after 24 months of follow-up was similar between test and control groups [27]. In another study, [28] 43 parents in the United States were surveyed. They were more concerned about the esthetic impact of SDF, and desired to understand the risks of alternative treatments. These US parents were more accepting of SDF treatment on posterior teeth as opposed to anterior teeth. Even for anterior teeth, if the alternate treatment was advanced behavior techniques such as sedation or general anesthesia, they would prefer SDF application. So, the geographic location, cultural differences, tooth selection, all appear to impact the response to the reported adverse esthetic effects (staining) of SDF.
In one of the survey studies Milgrom, et al. [19] included in this systematic review, HIV + children between the ages of 10 and 12 years reported that they did not want to experience SDF again since they were uncomfortable with the blackish discoloration and the metallic taste, and the authors recommended that SDF should be used with caution among HIV+ children as the black staining of the teeth could cause further emotional trauma. Two other studies Mei ML [29] also reported a temporary metallic taste or burning sensation.
In summary, tooth staining is the most reported adverse effect. This adverse aesthetic effect has an impact on parental acceptability and emotional quality of life of the child.
Systemic Illness and Toxicity
One study Duangthip, et al. [17] reported no systemic illness or acute toxicity including nausea, vomiting, or generalized discomfort, whereas one study Milgrom, et al. [19] reported a few cases of mild diarrhea or stomachache which resolved within 2-4 days. With regards to the toxic dose of fluoride, one study Duangthip, et al. [17] argued that at a minimum there is an eight-fold safety margin when SDF is applied to all teeth in a small child. This is consistent with the findings of an earlier systematic review [23] which dismissed the possibility of fluoride toxicity given that one drop of SDF which is enough to treat 6 teeth, contains approximately half the fluoride level of the smallest unit dose used for a fluoride varnish application. As regards the lethal dose of silver, if the sub-cutaneous route is taken as reference, there is a 380-fold safety margin if SDF is applied to all the teeth.
To summarize, SDF application is safe, and systemically, may at most cause mild illness or discomfort which resolves within 2 days.
Strength of Evidence
In this systematic review, we found only the study by Duangthip, et al. [17] was conducted with the primary aim of studying the adverse effects of SDF, either systemic or topical. Of the papers selected only half were randomized control trials.
In general, the most frequently downgraded domains were performance and detection bias (blinding of participants/personnel, calibration of examiners, or incomplete outcome data). Blinding in some of the studies could not be assured due to the dissimilarities of compared techniques and materials used (e.g., SDF and glass ionomer restoration). Only one of the six studies reported calibration of examiners. The studies conducted were not standardized in terms of assessment of adverse outcomes: some were surveys of parents or caregivers; one was a survey of the child undergoing SDF treatment, some were self-reported. If the symptoms were very mild, they may not have been observed or reported-thus leading to some under-reporting. At times, it was difficult to separate whether the adverse effects noted were due to the SDF or the disease itself.
A metanalysis was not possible due to the non- homogeneity of study designs, methods, and reporting. Since trial reporting is heterogenous, the use of a standardized protocol for reporting SDF clinical trials with the primary aim of studying adverse effects of SDF application is necessary. The Consolidated Standards of Reporting Trials (CONSORT) Statement may be useful to prevent deficiencies during result dissemination [30].
Summary
Although SDF use in dentistry is not new, no systematic reviews have been compiled, analyzing the reported adverse effects of SDF in pediatric populations.
Our review analyzed both systemic and topical adverse effects. In this review, we found the adverse reactions reported in the 6 trials were mild to moderate with few reactions, possibly unrelated to the application of SDF. Even these resolved within 2 days. Tooth staining was the most reported adverse effect with a related impact on emotional quality of life of the child and parental acceptability.
The results of this systematic review are clinically significant and may have a positive impact on the increased usage of SDF by informing dentists of the lack of potential adverse effects. This review may also help reassure patients and patients’ caregivers since the number and degree of adverse effects appear to be low. Finally, the review can help dentists plan the application of SDF to minimize potential adverse effects. This review should also be considered in the context of a comprehensive assessment of the potential public health impact of SDF. SDF application can be carried out as a non-aerosol-generating procedure and is a safe medicament in COVID times [31]. SDF application is fast, painless, and is a simple technique for children and clinicians, without requiring expensive dental equipment. Its use could safely and effectively reduce the high prevalence of early childhood caries [32].
Conclusion
Tooth staining is the most reported side-effect of SDF application. SDF does not cause serious systemic illness or oral trauma. The reports on oral pain and gingival injury are rare and transient, resolving within 48 hours. Based on the results of this systematic review, caries arrest treatment by SDF safe for children under 18 years of age.
Acknowledgement: The authors thank Dr. Sarah Pagni and Ms. Amanda Nevius for their contribution to this publication.
Financial Interest Disclosure
Dr. Andrea Zandona: Consultant for Colgate Palmolive, Greenmark, Calcivis and CareQuest. Dr. Justin Cardarelli: Lecturer for Southern Dental Industries (SDI) for their Riva star product. Others: None Appendix 1: Survey details 1. Clemens, et al. [16 ] Questions related to adverse effects: i. ease of application ii. comfort with discoloration, iii. pain-free application, and iv. acceptability of taste to the child. 2. Duangthip, et al. [17]
Structured questionnaire related to demographics, information on adverse effects of SDF treatment— including tooth or gum pain, gum swelling, gum bleaching (whiter in color), and systemic toxicity (nausea, vomiting, generalized discomfort)—was collected through a parental questionnaire within a week after SDF/placebo application at baseline and 6-, 12-, 18-, 24-, and 30-month follow-ups. Parents’ satisfaction with their children’s dental appearance and dental health was collected through a self-rated questionnaire at baseline and 18- and 30-month follow-ups. 3. Hiremath, et al. [18] Children oral health impact profile (COHIP-SF) English version. 4. Milgrom, et al. [19] Following questions were asked: i. Has the child received medical care (including visit to ER, medical doctor, nurse or health care provider in last 48 hours? ii. Since the treatment, has the child experienced Nausea, vomiting, difficulty in swallowing or breathing, swelling around the lips or skin of the face, itchiness around the lips or skin or face, hives or rash or stomachache or diarrhea? 5. Vollu, et al. [21] Interview was conducted to investigate burning in mouth, allergy, nausea, vomiting, altered taste of food, irritation of gums or mucosa, staining or bruising of the skin or into the mouth, and pain or tenderness in the teeth. Also, the interview ascertained if the child avoided smiling, or parental aesthetic concerns. Quality of life information was obtained using the B-ECOHIS questionnaire before and 15 days post-treatment.
References
-
Bernabe E, Marcenes W, Hernandez CR, Bailey J, Abreu LG, et al. (2020) Global, Regional, and National Levels and Trends in Burden of Oral Conditions from 1990 to 2017: A Systematic Analysis for the Global Burden of Disease 2017 Study. J Dent Res 99(4): 362-373.
-
Duangthip D, Gao SS, Lo EC, Chu CH (2017) Early childhood caries among 5- to 6-year-old children in Southeast Asia. Int Dent J 67(2): 98-106.
-
Gao SS, Zhang S, Mei ML, Lo EC, Chu CH (2016) Caries remineralisation and arresting effect in children by professionally applied fluoride treatment - a systematic review. BMC Oral Health 16: 12.
-
Mei ML, Ito L, Cao Y, Li QL, Lo EC, et al. (2013) Inhibitory effect of silver diamine fluoride on dentine demineralization and collagen degradation. J Dent 41(9): 809-817.
-
Yamaga R, Nishino M, Yoshida S, Yokomizo I (1972) Diamine silver fluoride and its clinical application. J Osaka Univ Dent Sch 12: 1-20.
-
FDA. FDA Product classification. Silver Spring MD. U.S. Department of Health and Human Sevices.
-
Elevate Oral Care (2017) The Silver Bulletin.
-
American Dental Association. CDT 2016: Dental procedures Code, 1st (Edn.), Chicago: American Dental Association 2015.
-
Chu CH, Lo ECM (2008) Promoting caries arrest in children with silver diamine fluoride: A review. Oral Health Prev Dent 6(4): 315-321.
-
Zhao IS, Gao SS, Hiraishi N, Burrow MF, Duangthip D, et al. (2018) Mechanisms of silver diamine fluoride on arresting caries: a literature review. Int Dent J 68(2): 67- 76.
-
Gao SS, Zhao IS, Hiraishi N, Duangthip D, Mei ML, et al. (2016) Clinical Trials of Silver Diamine Fluoride in Arresting Caries among Children: A Systematic Review. JDR Clin Trans Res 1(3): 201-210.
-
Atiyeh BS, Costagliola M, Hayek SN, Dibo SA (2007) Effect of silver on burn wound infection control and healing: review of the literature. Burns 33: 139-48.
-
Craig GG, Powell KR, Cooper MH (1981) Caries progression in primary molars: 24-month results from a minimal treatment program. Community Dentistry and Oral Epidemiology 9(6): 260-265.
-
Detsomboonrat P, Thongmak P, Lertpayab P, Aiemsri W, Sooampon S (2022) Optimal concentration of potassium iodide to reduce the black staining of silver diamine fluoride. J Dent Sci 17(1): 300-307.
-
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A (2016) Rayyan-a web and mobile app for systematic reviews. Systematic Reviews 5(1): 210.
-
Clemens J, Gold J, Chaffin J (2018) Effect and acceptance of silver diamine fluoride treatment on dental caries in primary teeth. J Public Health Dent 78(1): 63-68.
-
Duangthip D, Fung MHT, Wong MCM, Chu CH, Lo ECM (2018) Adverse Effects of Silver Diamine Fluoride Treatment among Preschool Children. J Dent Res 97(4): 395-401.
-
Hiremath AM, Anbu V, Kuduruthullah S, Khalil E, Elsahn NA, et al. (2020) Acceptability of silver diamine fluoride as interim measure towards untreated dental caries and its impact on ohrqol among children with HIV: Pilot study. Indian J Dent Res. 31(4): 502-506.
-
Milgrom P, Horst JA, Ludwig S, Rothen M, Chaffee BW, et al. (2018) Topical silver diamine fluoride for dental caries arrest in preschool children: A randomized controlled trial and microbiological analysis of caries associated microbes and resistance gene expression. J Dent 68: 72-78.
-
Rossi G, Squassi A, Mandalunis P, Kaplan A (2017) Effect of silver diamine fluoride (SDF) on the dentin-pulp complex: ex vivo histological analysis on human primary teeth and rat molars. Acta Odontol Latinoam 30(1): 5-12.
-
Vollu AL, Rodrigues GF, Teixeira RVR, Cruz LR, Massa GDS, et al. (2019) Efficacy of 30% silver diamine fluoride compared to atraumatic restorative treatment on dentine caries arrestment in primary molars of preschool children: A 12-months parallel randomized controlled clinical trial. J Dent 88: 103165.
-
Llodra JC, Rodriguez A, Ferrer B, Menardia V, Ramos T, et al. (2005) Efficacy of silver diamine fluoride for caries reduction in primary teeth and first permanent molars of school children: 36-month clinical trial. J Dent Res 84(8): 721-724.
-
Lo EC, Chu CH, Lin HC (2001) A community- based caries control program for pre-school children using topical fluorides: 18-month results. J Dent Res 80(12): 2017- 2074.
-
Crystal YO, Niederman R (2016) Silver Diamine Fluoride Treatment Considerations in Children’s Caries Management. Pediatr Dent 38(7): 466-471.
-
Baraka M, Tekeya M, Bakry NS, Fontana M (2022) Twelve-month randomized controlled trial of 38% silver diamine fluoride with or without potassium iodide in indirect pulp capping of young permanent molars. J Am Dent Assoc S0002-8177(22)00500-1.
-
Oliveira BH, Rajendra A, Keenan AV, Niederman R (2019) The Effect of Silver Diamine Fluoride in Preventing Caries in the Primary Dentition: A Systematic Review and Meta-Analysis. Caries Res 53(1): 24-32.
-
Chu CH, Lo ECM, Lin HC (2002) Effectiveness of silver diamine fluoride and sodium fluoride varnish in arresting dentin caries in Chinese pre-school children. J Dent Rest 81(11): 767-770.
-
Crystal YO, Kreider B, Raveis VH (2019) Parental Expressed Concerns about Silver Diamine Fluoride (SDF) Treatment. J Clin Pediatr Dent 43(3): 155-160.
-
Mei ML, Lo EC, Chu CH (2016) Clinical Use of Silver Diamine Fluoride in Dental Treatment. Compend Contin Educ Dent 37(2): 93-98.
-
Needleman I, Worthington H, Moher D, Schulz K, Altman DG (2008) Improving the completeness and transparency of reports of randomized trials in oral health: the CONSORT statement. Am J Dent 21(1): 7-12.
-
Singhal R, Singhal P, Namdev R, Negi S (2021) Can silver diamine fluoride be an alternative to aerosol-based dentistry during the COVID scenario? A retrospective analysis. J Indian Soc Pedod Prev Dent 39(3): 316-320.
-
Thomas ML, Magher K, Mugayar L, Dávila M, Tomar SL (2020) Silver Diamine Fluoride Helps Prevent Emergency Visits in Children with Early Childhood Caries. Pediatr Dent 42(3): 217-220.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells