Lateral Ridge Augmentation Using Cross-Linked or Non-Cross-Linked Collagen Membrane: A Pilot Randomized Clinical Trial
Purpose: The aim of this investigation is to test, in a lateral ridge augmentation model without simultaneous implant placement, the effect of using a cross-linked collagen membrane and a non-cross-linked collagen membrane on guided bone regeneration. Material and Methods: Edentulous alveolar ridges of less than 5 mm width were treated with guided bone regeneration using a glutaraldehyde cross-linked collagen membrane (CL) or a non-cross-linked collagen membrane (NonCL). In all treated cases the bone graft used was a combination of autogenous bone scrapings and deproteinized bovine bone mixed in a 1:3 ratio. Ridge measurements were recorded clinically (during augmentation surgery and during implant placement surgery) and radiographically on the CBCT scans (pre-op, 1 week post-op and at implant placement). All ridge measurements were recorded at 1, 3 and 5 mm from the ridge crest. Soft tissue healing was assessed during the follow-up visits at 1, 2, 4, 8, 12, 16, 20 and 24 weeks post-op. A histological analysis was performed on core biopsies retrieved axially from implant or pontic sites. Results: Four patients were recruited and randomly allocated to treatment groups. Ridge width gain (RWgain) was significantly better for the CL group as assessed clinically. At 1, 3 and 5 mm from ridge crest, the clinically assessed gain was respectively 5.50 mm ± 2.121, 5.40 mm ± 2.074, 5.60 mm ± 1.140 for the CL group and -1.33 mm ± 0.577, 1.33 mm ± 2.517 and 2.00 mm ± 1.000 for the NonCL group. Graft volume resorption was significantly higher in the NonCL group (62%) in comparison to the CL group (10.9%). No soft tissue complications occurred during follow-ups in neither group. Histologically, both groups showed signs of bone remodeling and vital bone formation. New bone formation in the NonCL group was 23.64 % ± 0.64 and in the CL group was 15.75% ± 8.73. Conclusion: Despite the limitations of this pilot study, The CL membrane showed better performance than the NonCL membrane in terms of ridge width gain and in terms of graft volume consolidation as assessed clinically and radiographically. Although no statistical comparison was possible, the NonCL group presented a higher percentage of new bone formation than the CL group.
Introduction
Sufficient bone width at the implant site is an important prerequisite for a predictable, long-term prognosis in implant dentistry [1]. Laterally deficient alveolar ridges have been treated using different techniques, such as block grafting [2], ridge splitting [3], distraction osteogenesis [4] and guided bone regeneration (GBR) [5, 6]. GBR is one of the most commonly applied and documented methods. It advocates, by placing a barrier membrane, the mechanical exclusion of undesirable soft tissue cells from growing into the osseous defect, allowing thereby, only osteogenic cell population to repopulate the osseous wound space [7]. Barrier membranes can be non-resorbable or resorbable. While the use of non-resorbable membranes is limited to major ridge defects, resorbable membranes and notably collagen membranes are widely used in a variety of ridge defects. The desirable characteristics of a collagen membrane in GBR include biocompatibility, cell-occlusion properties, integration by the host tissues, clinical manageability and space-making ability [8]. While non-cross-linked collagen membranes are considered to meet most requirements expected from bioabsorbable membranes, their barrier function is described to be relatively short [9, 10]. This is due to a rapid biodegradation of native collagen by the enzymatic activity of host tissues and microbes [9, 11]. The technique of collagen crosslinking by several physical, chemical, and enzymatic processes decreases the degradation rate of the collagen membranes and allows the extension of the barrier function [12]. It was observed that the degradation rate was directly related to the degree of cross-linking, however, when the degree of chemical cross-linking increased, more inflammatory cells seemed to be involved in the process of biodegradation accompanied by a foreign body reaction [9]. A major concern with the use of cross-linked membrane is tissue compatibility due to the presence of the cross-linking agent and the delay in transmembrane vascularization [9] that could possibly be the cause of a perceived higher prevalence of membrane exposure. While the increased incidence of cross-linked membrane exposure was reported Annen, et al. [13] two systematic reviews failed to corroborate this observation Merli, et al. [14] & Wessing, et al. [15]. The risk of soft tissue complications put aside; the efficacy of the two collagen membrane types was only tested in dehiscence defect models. Comparative animal [14, 15, 16, 17, 18], and clinical studies showed comparable bone formation results for both membrane types [19, 20].
Despite this available documentation, definitive conclusions on the comparative performance of the native and the cross-linked collagen membranes are difficult to draw due to the heterogeneity of the comparative trials, the reduced sample sizes, and the small defect sizes used for comparison (implant dehiscence type defect). No clinical study has yet been conducted comparing these 2 categories of collagen membrane in a lateral ridge augmentation model without simultaneous implant placement where the desired augmentation volume is usually greater compared to the dehiscence defect model. Hence, two fundamental questions are yet to be answered: 1-Will the gain in barrier function longevity, with the cross-linked membranes, enhances bone formation? 2-Different types and degrees of collagen cross-linking are associated with different degrees of inflammatory reaction and foreign body reaction during membrane degradation. To what extent this tissue reaction may impact bone formation? While the answer to those two questions is beyond the reach of this investigation, its objective is to test in a lateral alveolar ridge augmentation model (without simultaneous implant placement) the effect of using a glutaraldehyde cross-linked collagen membrane (CL) and a non-cross-linked collagen membrane (NonCL) on guided bone regeneration outcomes.
Material and Methods
Trial Design
This study is a pilot randomized clinical trial with parallel groups, with an observation period of 11 months. It was conducted in accordance with the CONSORT statement [21]. It is also registered in the ClinicalTrial.gov under the number NCT04402671.
Ethical Considerations
The study was conducted following the ethical principles founded in the Declaration of Helsinki and gained the approval of the ethical committee of the Saint-Joseph University (USJ – 2019 - 98). Prior to enrollment, all eligible patients signed the written informed consent and patients had the option to terminate their participation in the study at any time.
Participants
Patients Requiring Dental Implants with Horizontal Bone Crest Deficiency
- Inclusion criteria: Healthy patients, non-smokers, or smokers<10 cigarettes/day, age between 20 and 75, full mouth bleeding score <20 %, full mouth plaque score <15%, presence of a residual alveolar ridge with residual bone width < 5 mm and adequate bone height in the maxilla and the mandible, tooth extraction performed at least 6 weeks prior to surgery, presence of enough teeth to support an occlusal stent/radiographic guide.
- Exclusion criteria: Systematic diseases, history of radiotherapy in the head and neck region in the last 5 years, active periodontitis on the remaining teeth, pregnancy, allergy to collagen, intake of medications that may have an effect on bone turnover and mucosal healing (i.e., tetracycline within the last month, steroids within the last 6 months, bisphosphonates or fluorides at bone therapeutic levels, vitamin D and metabolites at therapeutic levels within the last 6 months).
Study Settings
Patients Treated at the Periodontology Department of the Saint-Joseph University Dental Faculty
- Sampling Blinding and randomization: A total number of 4 patients were recruited. Each group had 2 patients. The original protocol was designed to include 10 patients per group, but due to the covid-19 pandemic and the ensuing halt of activity at the treatment center only this limited number was recruited. Random allocation was done by the sequentially sealed envelope method. At the time of membrane placement during the surgery, the envelope corresponding to the case sequence number was opened specifying the group allocation. The patients were blind to the allocation. The practitioner was blind to the choice of membrane until the time of membrane placement during the surgery. The examiner of the data is also blind to the measurement of the primary and secondary outcomes. The NonCL group was allocated to the non-cross-linked collagen membrane (Bioguide®, Geistlisch Pharma AG, Wolhusen, Switzerland) and the CL group was allocated to glutaraldehyde cross-linked collagen membrane (RTM Collagen®, Osteogenics Biomedical, Lubbock, TX, USA). The bone graft used was a combination of autogenous bone scraped from the adjacent bony region and a demineralized bovine bone mineral (DBBM) (OCS-B Xenomatrix®, Nibec, Chungcheongbuk-do, Korea) mixed in a 1:3 ratio.
- Interventions: Before surgery, each patient received scaling, root planning and proper hygiene instructions. Then, an occlusal stent/radiographic guide (Stent) was prepared. At each implant site, a gutta-percha marker was incorporated to serve as a reference during the surgery and during the CBCT measurements. After that, a pre-operative CBCT with the Stent in the mouth was taken. Then, patients were put on an antibiotic regimen consisting of 1g co-amoxiclav taken twice daily (Augmentin, GlaxoSmithKline, Brentford, United Kingdom), starting the evening prior to surgery and continued for 10 days. For patients allergic to penicillin, Clindamycin 300mg, taken every 6 hours (Dalacin C, Pfeizer, New York City, NY, and USA) was prescribed. After rinsing with 0.12% CHX solution for one minute, local anesthesia was delivered. Mid-crestal and vertical releasing incisions were made, and full thickness flaps were raised. The recipient bone was curetted to remove any soft tissue. Using a ridge mapping caliper, Ridge Width (RW) was recorded at 1, 3 and 5mm from the crest at the level of the gutta-percha markers of the Stent. Using a periodontal probe, another measure was recorded from the Ridge Crest to the apical Border of the Stent (RC-BS) at each marker Figure 1. This measure was used during implant placement surgery to locate the vertical position of the pre-operative ridge measurements in case of changes in ridge height. After advancement of the buccal and lingual flaps, the buccal aspect of the crest was decorticated. Using a 0.5 cc spoon, the particulate bone graft consisting of a composite autograft-xenograft was then prepared in a 1:3 ratio mixed in sterile saline. The autograft was obtained by scraping the adjacent bony region with a bone scraper (SafeScraper TWIST, META, Reggio Emilia, and Italy). The xenograft used was a DBBM with a 250-1000 microns particle size (OCS-B Xenomatrix®, Nibec, Chungcheongbuk-do, Korea). After opening the sequentially sealed envelope, the patient was allocated to either CL or NonCL group. The membrane was fixed first on the buccal side with titanium pins (Masetrpin®, Meisinger, Neuss, Germany) in a way to create a pouch like space [22]. Second, the composite graft was applied between the membrane and the crest with a slight over fill. Then the membrane was slightly stretched, wrapped over the ridge, and tightly stabilized palatally/lingually with the titanium pins. Using (4/0) PTFE monofilament sutures (Osteogenics Biomedical, Lubbock, TX, USA), a tight wound closure was achieved by placing a first line of horizontal mattress sutures followed by a second line of combined Laurell-Gottlow sutures and interrupted sutures along the horizontal incision [22]. The vertical releasing incisions were closed with a combination of Laurel-Gottlow sutures and interrupted sutures [22]. All patients were prescribed 0.12% CHX mouthwash (twice daily for 2 weeks), NSAIDs drugs (Bruffen 400 mg every 6 hours, Abbott Laboratories, Illinois, CHI, USA) and/ or paracetamol-opioid analgesics (Solpadeine, Omega Pharma Nazareth, Belgium). An extraoral cold pressure dressing was applied. Sutures were removed 3 weeks after surgery. During the first week after surgery, a CBCT of the operated region was performed, with the Stent in place. Follow-up visits were performed at 1, 2, 4, 8, 12, 16, 20 and 24 weeks post-surgery.
![Figure 1: This measure was used during implant placement surgery to locate the vertical position of the pre-operative ridge measurements in case of changes in ridge height. After advancement of the buccal and lingual flaps, the buccal aspect of the crest was decorticated. Using a 0.5 cc spoon, the particulate bone graft consisting of a composite autograft-xenograft was then prepared in a 1:3 ratio mixed in sterile saline. The autograft was obtained by scraping the adjacent bony region with a bone scraper (SafeScraper TWIST, META, Reggio Emilia, and Italy). The xenograft used was a DBBM with a 250-1000 microns particle size (OCS-B Xenomatrix®, Nibec, Chungcheongbuk-do, Korea). After opening the sequentially sealed envelope, the patient was allocated to either CL or NonCL group. The membrane was fixed first on the buccal side with titanium pins (Masetrpin®, Meisinger, Neuss, Germany) in a way to create a pouch like space [22]. Second, the composite graft was applied between the membrane and the crest with a slight over fill. Then the membrane was slightly stretched, wrapped over the ridge, and tightly stabilized palatally/lingually with the titanium pins. Using (4/0) PTFE monofilament sutures (Osteogenics Biomedical, Lubbock, TX, USA), a tight wound closure was achieved by placing a first line of horizontal mattress sutures followed by a second line of combined Laurell-Gottlow sutures and interrupted sutures along the horizontal incision [22]. The vertical releasing incisions were closed with a combination of Laurel-Gottlow sutures and interrupted sutures [22]. All patients were prescribed 0.12% CHX mouthwash (twice daily for 2 weeks), NSAIDs drugs (Bruffen 400 mg every 6 hours, Abbott Laboratories, Illinois, CHI, USA) and/ or paracetamol-opioid analgesics (Solpadeine, Omega Pharma Nazareth, Belgium). An extraoral cold pressure dressing was applied. Sutures were removed 3 weeks after surgery. During the first week after surgery, a CBCT of the operated region was performed, with the Stent in place. Follow-up visits were performed at 1, 2, 4, 8, 12, 16, 20 and 24 weeks post-surgery.](/fulltextimages/9592/fig_1.jpeg)
1A
1B Figure 1: A: RW at 5 mm recorded at initial situation and during implant placement surgery. B: RC-BS recorded at initial situation and at implant placement surgery [23].
At the time of the implant placement surgery, another CBCT with the same Stent in place was taken. Mid-crestal and vertical releasing incisions were made, and full thickness flaps were raised: Any non-integrated bone graft material were gently scraped and washed out with saline. The Stent was put in place and using the previously recorded RC- BS measurement to correctly locate the level of previous measurements, RW was recorded with the ridge mapping caliper at the same locations. At implant or pontic sites, a 2 mm diameter trephine bone biopsy was collected for histological analysis. Inserted implants were left to heal in a submerged protocol Figures 2 & 3.
2A
![Figure 2: NonCL group. A: Pre-operative ridge. B: Membrane fixation and bone graft addition. C: Membrane fixation. D: Ridge at implant placement surgery. E: Implant placement [24].](/fulltextimages/9592/fig_2.jpeg)
2B
2C
2D
2E Figure 2: NonCL group. A: Pre-operative ridge. B: Membrane fixation and bone graft addition. C: Membrane fixation. D: Ridge at implant placement surgery. E: Implant placement [24].
![Figure 3: CL group. A: Pre-operative ridge. B: Membrane fixation and bone graft addition. C: Membrane fixation. D: Ridge at implant placement surgery. E: Implant placement [25].](/fulltextimages/9592/fig_3.jpeg)
3A
3B
3C
3D
![Figure 4: ** The CBCTs and the volumetric reconstructions of the DICOM files at pre-op. **A:** post op, **B:** implant placement surgery, **C:** for the CL group. The red volume represented the volume of the recipient bed before surgery. The green volume represented the volume of the graft at re-entry. The blue volume represented the volume of graft resorption between bone regeneration surgery and re-entry. The yellow volume represented the volume of the resorbed pristine bone after surgery [27].](/fulltextimages/9592/fig_4.png)
3E Figure 3: CL group. A: Pre-operative ridge. B: Membrane fixation and bone graft addition. C: Membrane fixation. D: Ridge at implant placement surgery. E: Implant placement [25].
CBCT Data Processing
For each patient the DICOM files from the 3 CBCT scans were imported into the ITK-snap software version 3.8.0 [26] and were superimposed with the registration tool using the maxillary anatomy and the gutta-percha markers of the Stent as references. The Region of Interest (ROI) corresponding to the grafted region was delineated in the 3 CBCT datasets. A semi-automatic density based active contour segmentation
![Figure 5: ** The CBCTs and the volumetric reconstructions of the DICOM files at pre-op. **A:** post op **B:** and implant placement surgery **C:** for the NonCL group. The red volume represented the volume of the recipient bed before surgery. The green volume represented the volume of the graft at re-entry. The blue volume represented the volume of graft resorption between bone regeneration surgery and re-entry. The yellow volume represented the volume of the resorbed pristine bone after surgery [27].](/fulltextimages/9592/fig_5.png)
![Figure 6: ** Volumetric measurements per implant site. **A:** implant placed at the gutta percha markers in a prosthetically driven position. **B:** Pivots indicating the two vertical and the apical cut, 1.5 mm from the implant surface. **C:** PreopV at the ROI of the implant site (white arrow). **D:** FinalV (black arrow) measured at implant level. **E:** PostopV at implant site [28].](/fulltextimages/9592/fig_6.png)
4A 4B 4C Figure 4: The CBCTs and the volumetric reconstructions of the DICOM files at pre-op. A: post op, B: implant placement surgery, C: for the CL group. The red volume represented the volume of the recipient bed before surgery. The green volume represented the volume of the graft at re-entry. The blue volume represented the volume of graft resorption between bone regeneration surgery and re-entry. The yellow volume represented the volume of the resorbed pristine bone after surgery [27].
technique was used in order to create a 3D model of the pristine bone and bone grafts. The following volumes were delineated: the pre-operative volume of the crest (PreopV), the post-operative volume of the crest (PostopV), the volume of the crest at implant placement surgery (FinalV), volume of the created graft without the recipient bed (graftV), the volume of recipient bed resorption (RecibR) and volume of graft resorption (GR) Figures 4 & 5.
![Figure 7: RW measurements at 1, 3 and 5mm from the RC in the CL group. Red outline: recipient bed outline before surgery. Green outline: The graft outline at re-entry. Blue outline: outline of the resorbed graft during healing. The combined outline of the blue and green outline represents the surface of the created graft immediately after the regeneration surgery [28].](/fulltextimages/9592/fig_7.png)
![Figure 8: RW measurements at 1, 3 and 5mm from RC in the NonCL group. Red outline: recipient bed outline before surgery. Green outline: The graft outline at re-entry. Blue outline: outline of the resorbed graft during healing. The combined outline of the blue and green outline represents the surface of the created graft immediately after the regeneration surgery [29].](/fulltextimages/9592/fig_8.jpeg)
5A 5B 5C Figure 5: The CBCTs and the volumetric reconstructions of the DICOM files at pre-op. A: post op B: and implant placement surgery C: for the NonCL group. The red volume represented the volume of the recipient bed before surgery. The green volume represented the volume of the graft at re-entry. The blue volume represented the volume of graft resorption between bone regeneration surgery and re-entry. The yellow volume represented the volume of the resorbed pristine bone after surgery [27].
Volumetric Measurements per Implant Site (mm3)
The designated volumes on the previous software were exported as Surface Mesh (STL) and imported into the BlueSky Plan software. For each patient, implants of the same height
and diameter (Straumann, Bone Level, 3.3 mm diameter and 10 mm length) were added and positioned at the level of the gutta-percha markers of the Stent in a prosthetically driven position. Then, the STL files of the implants, the 3D bone models were transferred to the Autodesk® MeshMixer software version 3.5.474 (2017, Autodesk, Inc.).
6A 6B
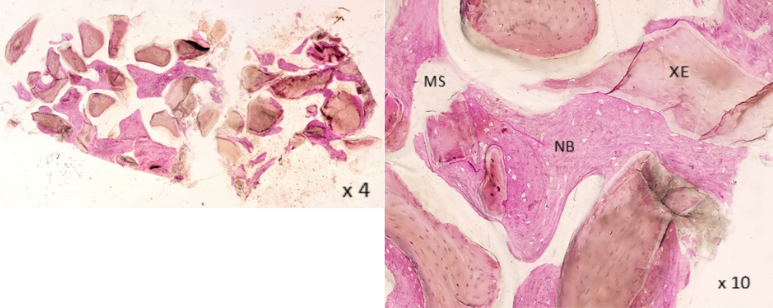
![Figure 9: CL group: Sections seen under an optical microscope (Olympus BX 60, Olympus Corporation, Tokyo, Japan), with x4, x10 magnifications. NB: New Bone Formation. XE: DBBM particles. MS: Marrow Space [29].](/fulltextimages/9592/fig_9.jpeg)
6C 6D
6E Figure 6: Volumetric measurements per implant site. A: implant placed at the gutta percha markers in a prosthetically driven position. B: Pivots indicating the two vertical and the apical cut, 1.5 mm from the implant surface. C: PreopV at the ROI of the implant site (white arrow). D: FinalV (black arrow) measured at implant level. E: PostopV at implant site [28].
For each implant site, a ROI was designated using two vertical plane cuts parallel to the long axis of the implant, distant 1.5 mm from the mesial and distal surface of each implant, and one horizontal plane cut perpendicular to the implant axis distant 1.5 mm from the apex of the implant. At each implant site, the PreopV, PostopV, FinalV, GraftV, RecibR and GR were therefore measured in cubic millimeters (mm3). These volumes allowed the calculation of the percentage of graft resorption (% GR) Figure 6.
Radiographic Linear Measurements per Implant Site (Mm)
In the BlueSky plan software, the placed implants were used as reference axis for the measurements of RW. At each site, RW was measured at 1, 3, and 5 mm from RC for the pre-operative ridge, post-operative ridge, and the ridge after remodeling, while being parallel to the implant axis Figures 7 and 8. The changes in linear ridge width between post- operative situation and implant placement situation allowed the calculation of the linear graft resorption at 1, 3 and 5mm from the ridge crest (LinearGR) Figures 7 & 8.
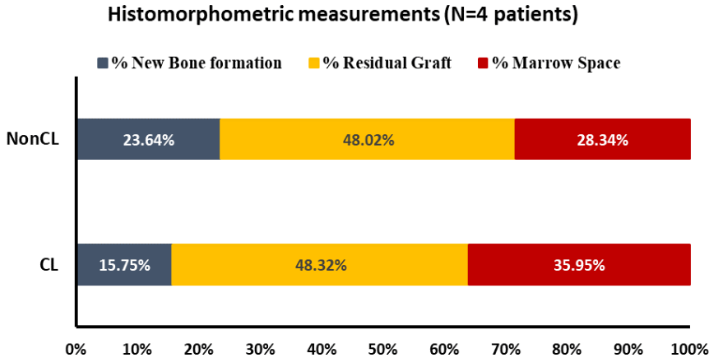
![Figure 10: Histomorphometry measurements in each group. CL: glutaraldehyde cross-linked collagen membrane. NonCL: Non-cross-linked collagen membrane [30].](/fulltextimages/9592/fig_10.png)
Figure 7: RW measurements at 1, 3 and 5mm from the RC in the CL group. Red outline: recipient bed outline before surgery. Green outline: The graft outline at re-entry. Blue outline: outline of the resorbed graft during healing. The combined outline of the blue and green outline represents the surface of the created graft immediately after the regeneration surgery [28].
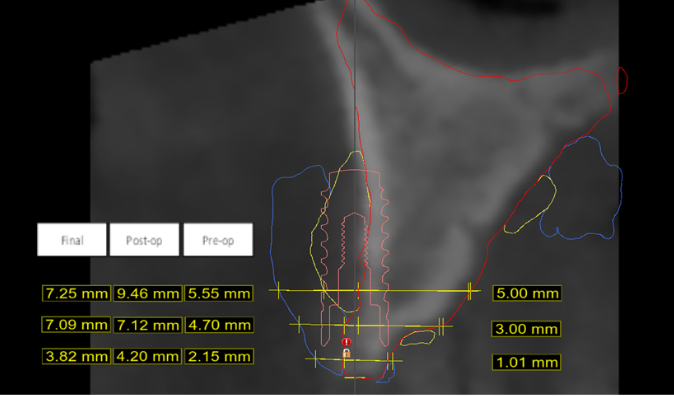
Figure 8: RW measurements at 1, 3 and 5mm from RC in the NonCL group. Red outline: recipient bed outline before surgery. Green outline: The graft outline at re-entry. Blue outline: outline of the resorbed graft during healing. The combined outline of the blue and green outline represents the surface of the created graft immediately after the regeneration surgery [29].
Histological Processing
Collected samples were treated with non-demineralized histology with Methyl Methacrylate resin inclusion. At the time of sampling, the samples were fixed in LILLIE neutral formalin, diluted to 10% in buffered sodium phosphate pH 7.4. The samples were then rinsed under running water for 48 hours. The dehydration of the samples was carried out in alcohol baths of increasing concentration, for 48 hours in each bath, then the clarification, allowing the penetration of methacrylate, in 2 successive xylene baths. The blocks were cut under irrigation and at slow speed with an Exact saw (Cutting machine EXACT-APPARATEBAU Nordersted, Germany), so as to take cuts of at least 80 μm. These cuts were subsequently reduced in thickness with the exact abrasion system. The sections were stained with Giemsa-Paragon and basic fushin. Giemsa gave cells and nuclei the color blue, and Paragon stained bone in red Figure 9.
The histomorphometry was performed at the Oral Biology Division (Craniofacial Research Laboratory, Faculty of Dental Medicine, and Saint-Joseph University of Beirut). The sections were qualitatively assessed under an optical microscope (Olympus BX 60, Olympus Corporation, and Tokyo, Japan). Using Image J software, a semi-automatic segmentation of the total ROI, woven bone, residual bone graft and marrow space was realized using the color thresholding tool and the manual selection tool. For each biopsy, the percentage of woven bone, the percentage of residual bone graft and the percentage of marrow space were calculated Figure 10.
Outcome Measurements
Primary Outcomes
- Ridge Width gain (RWgain) (mm): Calculated as the difference in clinical measurements of the ridge width, at each gutta-percha site, between the initial situation of the ridge and the situation at implant placement, taken at 1, 3 and 5 mm from the initial ridge crest. Negative values indicate a loss of bone horizontally.
- Radiographic Percentage of Graft resorption (%GR): For each group, the mean percentage of graft resorption (in volume) was calculated at each site as:
• Radiographic Linear Graft resorption (LinearGR): Calculated as the difference in radiographic measurements of the RW, at each gutta-percha site, between the situation directly after augmentation (post- op) and the situation at implant placement (final), taken at 1, 3 and 5 mm from the initial RC.
Secondary Outcomes
- Ridge Height gain (RHgain) (mm): Even though the augmentation is intended in the horizontal direction, changes in the ridge height can occur. These changes were documented by calculating the difference in the position of the ridge crest in relation to the Stent between the initial situation and the situation at implant placement. Negative values indicate a loss of bone vertically.
- Soft Tissue Healing: Soft tissue healing was assessed during the follow-up visits at 1, 2, 4, 8, 12, 16, 20 and 24 weeks post-surgery for the following occurrences: Redness and swelling, wound dehiscence and membrane exposure. Suppuration or any other unaccounted complications are also recorded.
- Histological Analysis: A descriptive histological analysis assessing remodeling and vital bone formation was performed. The sample size did not allow a statistical comparison of histomorphometry between the groups.
Statistical Analysis
The level of significance was set at -p-value≤0.05. The normality distribution of continuous variables was assessed using Kolmogorov-Smirnov tests and Shapiro-Wilk tests. Initial comparability between CL and NonCL groups were tested using Student-t tests and Mann-Whitney tests. Repeated-measure analysis of variance was used to compare RWgain between groups and within levels from the crest (1 mm, 3mm and 5mm). It was followed by univariates analyses and the multiple comparisons tests LSD. Mann-Whitney test was used to compare the RHgain between CL and NonCL groups. Paired Student t tests were also used to compare the volumetric measurements in mm3 between groups. The mean percentage and standard deviation were used to describe the histomorphometry measurements in each group.
Results
The implant placement surgery was done between 7-8 months after the GBR surgery except for one patient belonging to the NonCL group where we had to unintentionally wait for 11 months due to the covid-19 pandemic and the ensuing halt of activity at the treatment center. All patients presented sufficient amount of bone for implant placement. The number of placed implants varied between the two groups: 5 for the CL group and 3 for the NonCL group. During implant placement surgery, remnants of the collagen membrane were visible in the CL group but were totally absent in the NonCL group Table 1.
| CL | NonCL | -p-value | |||
|---|---|---|---|---|---|
| Patient | 1 | 2 | 3 | 4 | |
| Age | 54 | 45 | 49 | 63 | |
| Sex | Female | Female | Male | Female | |
| Regeneration site | Maxilla left | Maxilla right | Maxilla anterior | Mandible left | |
| Mean RW at 1mm | 1.900 ± 0.742 | 1.333 ± 0.577 | 0.305 | ||
| Mean RW at 3mm | 3.400 ± 0.894 | 3.333 ± 1.527 | 0.939 | ||
| Mean RW at 5mm | 4.800 ± 0.447 | 4.500 ± 1.500 | 0.677 | ||
| FmBS (%) | 15 | 17 | 15 | 16 | |
| FmPS (%) | 23 | 30 | 25 | 25 | |
| Smoking (cig/day) | 10 | 0 | 0 | 0 | |
| Health Status | Controlled thyroid dysfunction | Healthy | Allergic to penicillin. Controlled Hypertension | Healthy | |
| CBCT preop | Yes | Yes | Yes | Yes | |
| CBCT post op | Yes | Yes | Yes | Yes | |
| CBCT re-entry | Yes | Yes | Yes | Yes | |
| Implant placement date | 30 weeks | 30 weeks | 44 weeks | 30 weeks | |
| Placed implants | 2 | 3 | 2 | 1 |
Table 1: Patient’s characteristics.
CL: glutaraldehyde cross-linked collagen membrane; NonCL: Non-cross-linked collagen membrane; RW: Ridge width; FMBS: Full mouth bleeding score; FMPS: Full mouth plaque score. Table 1: Patient’s characteristics.
Primary Outcomes
At 1, 3 and 5 mm from ridge crest, the clinically assessed gain was respectively 5.50 mm ± 2.121, 5.40 mm ± 2.074, 5.60 mm ± 1.140 for the CL group and -1.33 mm ± 0.577, 1.33 RW gain (mm) Mean ± Std. Dev. CL (n=5) NonCL (n=3) -p-value 1 mm 5.50 ± 2.121 -1.33 ± 0.577a 0.002 3 mm 5.40 ± 2.074 5.40 ± 2.074 0.047 5 mm 5.60 ± 1.140 2.00 ± 1.000b 0.004 -p-value 0.964 0.047 mm ± 2.517 and 2.00 mm ± 1.000 for the NonCL group Table 2. The mean RWgain was significantly higher in the CL group in comparison to NonCL at at 1 mm (-p-value = 0.002), 3 mm (-p-value =0.047) and 5 mm (-p-value=0.004).
- a, b: different letters indicate the presence of significant difference within levels using multiple comparisons tests.
Table 2: Mean Ridge Width gain between initial situation and the situation at implant placement in different groups.
Within levels, the mean RWgain was not significantly different between 1mm, 3mm and 5mm for the CL group (-p-value=0.964). While for the NonCL group, within levels, the RWgain was lower at 1mm and greater at 3mm and 5mm (-p-value=0.047). The difference was not significant between 3mm and 5mm (-p-value=0.499) Table 3.
| Groups | Number of sites | Mean | Std. Deviation | -p-value | |
|---|---|---|---|---|---|
| PreopOV | CL | 5 | 401.44 | 93.237 | 0.444 |
| NonCL | 3 | 448.267 | 32.056 | ||
| PostopV | CL | 5 | 764.012 | 91.798 | 0.355 |
| NonCL | 3 | 820.96 | 36.465 | ||
| FinalV | CL | 5 | 696.16 | 109.751 | 0.13 |
| NonCL | 3 | 575 | 52.483 | ||
| GraftV | CL | 5 | 362.572 | 100.429 | 0.882 |
| NonCL | 3 | 372.693 | 62.406 | ||
| RecibR | CL | 5 | 27.82 | 14.701 | 0.34 |
| NonCL | 3 | 18.427 | 5.458 | ||
| GR | CL | 5 | 40.032 | 33.9 | 0 |
| NonCL | 3 | 227.533 | 14.306 |
Table 3: Mean volume measurements in each group. As for the %GR, the NonCL group presented higher percentage of graft resorpti
PreopV: the pre-operative volume of the crest; PostopV the post-operative volume of the crest; FinalV: volume of the crest at implant placement surgery; GraftV: the volume of the created graft during augmentation surgery; RecibR: volume of recipient bed resorption; GR: Volume of graft resorption. Table 3: Mean volume measurements in each group. As for the %GR, the NonCL group presented higher percentage of graft resorption (62.5%) in comparison to the CL group (10.9%) (-p-value<0.001) Table 4.
| Groups | Number of sites | Mean | Std. Deviation | -p-value | |
|---|---|---|---|---|---|
| %GR | CL | 5 | 10.91 | 10.326 | 0.001 |
| NonCL | 3 | 62.522 | 13.328 |
Table 4: Percentages of graft resorption between the groups.
The mean LinearGR between post-operative situation and situation at implant placement at 1, 3 and 5 mm from ridge crest was -1.572 ± 0.729, -0.116 ± 0.271, -0.510 ± 0.694 respectively for the CL group and -6.450 ± 3.423, -2.637 ± 0.528, -1.673 ± 1.459 respectively for the NonCL group. The mean LinearGR was significantly lesser on CL group compared to NonCL group at 1 mm (-p-value =0.018) and 3 mm (-p-value<0.001); however, the difference was not significant at 5 mm (-p-value=0.393) Table 5.
Within levels, the mean LinearGR was significantly different within 1mm, 3mm and 5mm levels for CL group (-p-value=0.008); and for the NonCL group (-p-value=0.050); the resorption was greater at 1mm, but the difference was not significant between 3mm and 5 mm (-p-value>0.05) Table 5.
- Linear GR (mm) Mean ± Std. Dev.
- CL (n=5)
- NonCL (n=3)
- -p-value
- 1 mm
- -1.572 ± 0.729a
- -6.450 ± 3.423a
- 0.018
- 3 mm
- -0.116 ± 0.271b
- -2.637 ± 0.528b
- <0.001
- 5 mm
- -0.510 ± 0.694b
- -1.673 ± 1.459b
- 0.393
- -p-value
- 0.008
- 0.05
- Secondary Outcomes
- The mean RH gain between initial situation and the situation at implant placement was significantly different between CL and NonCL (-p-value=0.046); While the NonCL group showed a vertical bone loss (-1.667 ± 0.577 mm), the
- CL group performed better (0.100 ± 1.245 mm) Table 6.
- RH gain (mm) Mean ± Std. Dev.
- CL (n=5)
- NonCL (n=3)
- -p-value
- 0.100 ± 1.245
- -1.667 ± 0.577
- 0.046
Table 5: Mean Ridge height gain between the initial situation
- a, b: Different letters indicate the presence of significant difference within levels using multiple comparisons tests.
Table 6: Radiographic linear Graft width Resorption at 1, 3 and 5 mm from Ridge Crest.
- Linear GR (mm) Mean ± Std. Dev.
- CL (n=5)
- NonCL (n=3)
- -p-value
- 1 mm
- -1.572 ± 0.729a
- -6.450 ± 3.423a
- 0.018
- 3 mm
- -0.116 ± 0.271b
- -2.637 ± 0.528b
- <0.001
- 5 mm
- -0.510 ± 0.694b
- -1.673 ± 1.459b
- 0.393
- -p-value
- 0.008
- 0.05
- Secondary Outcomes
- The mean RH gain between initial situation and the situation at implant placement was significantly different between CL and NonCL (-p-value=0.046); While the NonCL group showed a vertical bone loss (-1.667 ± 0.577 mm), the
- CL group performed better (0.100 ± 1.245 mm) Table 6.
- RH gain (mm) Mean ± Std. Dev.
- CL (n=5)
- NonCL (n=3)
- -p-value
- 0.100 ± 1.245
- -1.667 ± 0.577
- 0.046
Table 5: Mean Ridge height gain between the initial situation
The four patients manifested redness and swelling at week 1 after the regeneration surgery. It resolved at week 2 in all patients except one patient from the NonCL group who presented an extended inflammation. No suppuration, wound dehiscence, neither membrane exposure was detected during the follow ups.
Bone biopsies were successfully retrieved from all patients. Histological analysis revealed new bone formation in all histological sections.
At high magnification (x10), woven bone appeared in direct contact with DBBM particles in both groups. The trabecula of the woven bone appeared in divided cementum lines, indicating the ongoing remodeling process. The orientation of the trabeculae was circumferential around the DBBM material, demonstrating the parallel fiber bone structure. The DBBM particles were of variable shapes and were more present in the CL group. Some were not embedded in the bone. No sign of resorption of the xenograft was visible. No remnants of the collagen membranes were visible histologically, and no sign of inflammatory cells Figure 9.
The mean percentage of new bone formation in the CL group (15.75 % ± 8.73) was lower than the NonCL group (23.64 % ± 0.64). As for the percentage of residual graft, the CL and the NonCL presented similar mean percentages (48.32 % ± 5.08 and 48.02 % ± 6.43 respectively). The percentage of Marrow Space in the NonCL group (28.34 % ± 7.08) was lower than the CL group (35.95 % ± 3.66) Figure 10.
Discussion
This study is a pilot randomized clinical trial; it aims to test the effect of using a cross-linked collagen membrane and a non-cross-linked collagen membrane on guided bone regeneration.
The RW gain between initial situation and the situation at implant placement reflected the real variation of bone width after surgery. At 1 mm from the crest, the CL group presented 5.50 mm ± 2.121 of bone width augmentation, while the NonCL group presented a loss of bone width (-1.33 mm ± 0.577). At 3 and 5 mm from the ridge crest, the CL showed significantly better bone width augmentation in comparison to the NonCL group (5.40 mm ± 2.074 vs 1.33 mm ± 2.517 at 3mm, and 5.60 mm ± 1.140 vs 2.00 mm ± 1.000 at 5 mm, respectively). The primary results of this study were difficult to compare with other studies since no paper compared the two membranes in a clinical Cawood-Howell Class IV ridge defect. The clinical and animal studies comparing the effect of the two collagen membranes on bone formation were applied in implant dehiscence type defect and only dehiscence defect resolution was evaluated [19, 20, 24, 25, 26, 27, 28].
The NonCL group showed a loss of bone width at top of the crest and a gain of bone width of 1.33 mm ± 2.517 at 3 from RC. These results are not in accordance with the studies testing the same non-cross-linked collagen membrane in a similar clinical set-up: One paper found 3.6 mm of crestal bone gain [29], and other papers found an average of 5.6 mm of crestal bone gain [30, 31]. This contradiction in the results could be explained by the measuring method: Both authors in their studies measured the crestal bone width variation at crest without taking in consideration the vertical bone loss that could have occurred after remodeling. The measurements in those studies were not taken at the same level of the RC between regeneration surgery and implant placement surgery.
In the CL group, 5.50 mm ± 2.121 of bone width augmentation was recorded at 1 mm from RC and 5.40 mm ± 2.074 at 3 mm from RC. These results are in accordance with the horizontal clinical mean gain (5.27 mm) obtained in one study testing a ribose cross-linked collagen membrane in combination with an allograft [32]. However, the measurement method in this study was different from oursand lacked standardization. To our knowledge, no study tested a glutaraldehyde cross-linked collagen membrane in a similar horizontal bone defect type.
Beside bone gain, our study investigated the amount of graft resorption in relation to the use of a non-cross-linked or a cross-linked collagen membrane.
Assessed in a linear fashion, at 1 and 3 mm from crest, graft width was statistically better preserved in the CL group, while at 5mm; no difference was detected between the two groups. In both groups, bone remodeling/resorption were more pronounced at top of the crest. This pattern is generally seen after horizontal bone augmentations with GBR, yet, few studies have described and discussed this finding [33]. At crest, less bone augmentation is generally seen. This could be linked to primary wound closure and graft displacement [34, 35], to the stability of the membrane [36, 37], the mastication forces and the muscle pull [38] and possibly other factors. In this randomized clinical study, more bone was lost at 1 mm from ridge, in both groups, however, the loss was statistically less pronounced in the CL group.
Assessed in a volumetric fashion per implant site, the NonCL group showed a statistically higher percentage of graft resorption, reaching 62 % versus a loss of only 10.9% in the CL group. The volumetric changes of the NonCL group are comparable to the results of one study using also a non- cross-linked collagen membrane to cover a graft mixture of DBBM and autogenous bone in two different ratios (90:10 vs 60:40). They reported 55.3% and 53.8% of graft volume reduction respectively [39].
The better preservation of the graft volume in the CL group could be explained by the higher resistance to degradation of the CL membrane allowing a more durable barrier effect against soft tissue inclusion and offering more time for graft consolidation. Another explanation could be the higher rigidity of the cross-linked membrane that may have allowed better resistance against membrane collapse.
Despite frequent clinical observation, changes in ridge heights are always overlooked in lateral ridge augmentation studies. In our study, the NonCL group presented a pronounced vertical bone loss of -1.667 ± 0.577 mm, while the CL group barely changed (0.100 ± 1.245 mm). while it is difficult to draw conclusion from such a reduced sample, it is interesting to note that changes in ridge height needs to be accounted for in future studies.
Cross-linking with glutaraldehyde has been controversial, as many studies reported decreased membrane biocompatibility [40, 41, 42], other studies have reported positive impact on fibroblasts and osteoblasts [43, 44] and enhancement of bone regeneration [14]. One animal study testing Glutaraldehyde cross-linked collagen membrane, detected a clear histological separation between the flap and the tested membrane, but no inflammatory cells were detected [16]. In this randomized clinical trial, no patient manifested early or delayed membrane exposure. However, studies comparing non-cross-linked to cross-linked collagen membranes reported variable membrane exposure rates: In one study, significantly more soft tissue dehiscence and infections were reported for an experimental chemically cross-linked membrane compared with a non-cross-linked one [26]. Another randomized clinical trial using the same experimental membrane but with a larger sample, showed that the frequency of soft tissue dehiscence were similar in both membranes [25]. One study comparing ribose cross- linked membrane, a non-cross-linked collagen membrane and a non-resorbable membrane reported similar incidence of spontaneous membrane exposure between groups [19].
A systematic review on the treatment of dehiscence peri-implant defects with collagen membranes, found more frequent soft tissue complication using cross-linked membranes but the odds ratio was not significant [45]. A more recent systematic review found no statistical difference in membrane exposure between the two membranes among included studies [13].
The bone biopsies in all four patients were collected from implant site in 3 cases and from a pontic site in one case. It could have been better if the biopsies were harvested in a horizontal direction, this would have allowed the comparison of the composition of the bone at variable horizontal depths [39]. The NonCL group presented a higher percentage of woven bone and a smaller percentage of marrow space in comparison to the CL group. The two groups presented similar percentages of residual graft. One study using the same non-cross-linked collagen membrane and a similar bone composition found 25.6% of woven bone, 7.5 months after lateral bone augmentation [39]. An animal study comparing the same non-cross-linked collagen membrane to an experimental chemically cross-linked collagen membrane in dogs, found similar percentages of woven bone between the cross-linked and the non-cross- linked collagen membrane groups, at 8 and 16 weeks post GBR [15]. When tested in pigs, the two membranes showed no statistical difference in the percentage of bone formation at 16 weeks [18]. In this study, the higher percentage of new bone formation in the NonCL group could be the result of the longer healing period in 50% of this group’s cases (11 months vs 7.5 months). This interpretation can be supported by one study where significantly greater new vital bone formation occurred when sites healed for 18 to 20 weeks compared with 8 to 10 weeks prior to dental implant placement in an alveolar ridge preservation model [46].
Conclusion and Perspectives
Despite our reduced sample size and the ensuing caution in result interpretation, the present study is a novel one. It is the first to compare the effect of non-cross-linked collagen membrane to cross-linked collagen ones in a defect bigger than the dehiscence type defect, supposing that a bigger defect could show a possible difference in performance where a smaller one failed to show it so far. The protocol of this study can be considered for future clinical trials with larger population.
Acknowledgement
This work was carried out at the unit of Oral Biology and cranio- facial imaging at the Cranio-Facial Research Laboratory at the Faculty of Dental Medicine at Saint Joseph University of Beirut, Lebanon.
References
-
Elgali I, Omar O, Dahlin C, Thomsen P (2017) Guided bone regeneration: materials and biological mechanisms revisited. Eur J Oral Sci 125(5): 315-337.
-
Nkenke E, Neukam FW (2014) Autogenous bone harvesting and grafting in advanced jaw resorption: morbidity, resorption and implant survival. Eur J Oral Implantol 7(2): 203-217.
-
Scipioni A, Bruschi GB, Calesini G (1994) The edentulous ridge expansion technique: a five-year study. Int J Periodontics Restorative Dent 14(5): 451-459.
-
McCarthy JG, Schreiber J, Karp N, Thorne CH, Grayson BH (1992) Lengthening the human mandible by gradual distraction. Plast Reconstr Surg 89(1): 1-8.
-
Buser D, Brägger U, Lang NP, Nyman S (1990) Regeneration and enlargement of jaw bone using guided tissue regeneration. Clin Oral Implants Res 1(1): 22-32.
-
Nyman S, Lang NP, Buser D, Bragger U (1990) Bone regeneration adjacent to titanium dental implants using guided tissue regeneration: a report of two cases. Int J Oral Maxillofac Implants 5(1): 9-14.
-
Dahlin C, Linde A, Gottlow J, Nyman S (1998) Healing of bone defects by guided tissue regeneration. Plast Reconstr Surg 81(5): 672-676.
-
Hardwick R, Hayes BK, Flynn C (1995) Devices for dentoalveolar regeneration: an up-to-date literature review. J Periodontol 66(6): 495-505.
-
Rothamel D, Schwarz F, Sager M, Herten M, Sculean A, et al. (2005) Biodegradation of differently cross-linked collagen membranes: an experimental study in the rat. Clin Oral Implants Res 16(3): 369-378.
-
Benic GI, Hämmerle CHF (2014) Horizontal bone augmentation by means of guided bone regeneration. Periodontol 2000 66(1): 13-40.
-
Kozlovsky A, Aboodi G, Moses O, Tal H, Artzi Z, et al. (2009) Bio-degradation of a resorbable collagen membrane (Bio-Gide) applied in a double-layer technique in rats. Clin Oral Implants Res 20(10): 1116-1123.
-
Elgali I, Omar O, Dahlin C, Thomsen P (2017) Guided bone regeneration: materials and biological mechanisms revisited. Eur J Oral Sci 125(5): 315-337.
-
Annen BM, Ramel CF, Hämmerle CH, Jung RE (2011) Use of a new cross-linked collagen membrane for the treatment of peri-implant dehiscence defects: a randomised controlled double-blinded clinical trial. Eur J Oral Implantol 4(2): 87-100.
-
Merli M, Merli I, Raffaelli E, Pagliaro U, Nastri L, et al. (2016) Bone augmentation at implant dehiscences and fenestrations. A systematic review of randomised controlled trials. Eur J Oral Implantol 9(1): 11-32.
-
Wessing B, Lettner S, Zechner W (2018) Guided Bone Regeneration with Collagen Membranes and Particulate Graft Materials: A Systematic Review and Meta-Analysis. Int J Oral Maxillofac Implants 33(1): 87-100.
-
Oh TJ, Meraw SJ, Lee EJ, Giannobile WV, Wang HL (2003) Comparative analysis of collagen membranes for the treatment of implant dehiscence defects. Clin Oral Implants Res 14(1): 80-90.
-
Bornstein MM, Bosshardt D, Buser D (2007) Effect of two different bioabsorbable collagen membranes on guided bone regeneration: a comparative histomorphometric study in the dog mandible. J Periodontol 78(10): 1943- 1953.
-
Schwarz F, Rothamel D, Herten M, Wüstefeld M, Sager M, et al. (2008) Immunohistochemical characterization of guided bone regeneration at a dehiscence-type defect using different barrier membranes: an experimental study in dogs. Clin Oral Implants Res 19(4): 402-415.
-
Zubery Y, Goldlust A, Alves A, Nir E (2007) Ossification of a novel cross-linked porcine collagen barrier in guided bone regeneration in dogs. J Periodontol 78(1): 112-121.
-
Bornstein MM, Heynen G, Bosshardt DD, Buser D (2009) Effect of two bioabsorbable barrier membranes on bone regeneration of standardized defects in calvarial bone: a comparative histomorphometric study in pigs. J Periodontol 80(8): 1289-1299.
-
Moses O, Pitaru S, Artzi Z, Nemcovsky CE (2005) Healing of dehiscence-type defects in implants placed together with different barrier membranes: a comparative clinical study. Clin Oral Implants Res 16(2): 210-219.
-
Friedmann A, Gissel K, Soudan M, Kleber BM, Pitaru S, et al. (2011) Randomized controlled trial on lateral augmentation using two collagen membranes: morphometric results on mineralized tissue compound. J Clin Periodontol 38(7): 677-685.
-
Moher D, Hopewell S, Schulz KF, Montori V, Gøtzsche PC, et al. (2010) CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. J Clin Epidemiol 63(8): 1-37.
-
Samarani R (2018) Revisiting Guided Bone Regeneration in the Esthetic Zone. In: Advances in Esthetic Implant Dentistry 197-246.
-
Yushkevich PA, Piven J, Hazlett HC, Smith RG, Ho S, et al. (2006) User-guided 3D active contour segmentation of anatomical structures: significantly improved efficiency and reliability. NeuroImage 31(3): 1116-1128.
-
Park SH, Lee K, Oh TJ, Misch CE, Shotwell J, et al. (2008) Effect of absorbable membranes on sandwich bone augmentation. Clin Oral Implants Res 19(1): 32-41.
-
Becker J, Al Nawas B, Klein MO, Schliephake H, Terheyden H, et al. (2009) Use of a new cross-linked collagen membrane for the treatment of dehiscence-type defects at titanium implants: a prospective, randomized- controlled double-blinded clinical multicenter study. Clin Oral Implants Res 20(7): 742-749.
-
Lee DW, Kim KT, Joo YS, Yoo MK, Yu JA, et al. (2015) The Role of Two Different Collagen Membranes for Dehiscence Defect Around Implants in Humans. J Oral Implantol 41(4): 445-458.
-
Lee JH, Lee JS, Baek WS, Lim HC, Cha JK, et al. (2015) Assessment of dehydrothermally cross-linked collagen membrane for guided bone regeneration around peri- implant dehiscence defects: a randomized single-blinded clinical trial. J Periodontal Implant Sci 45(6): 229-237.
-
Hämmerle CHF, Jung RE, Yaman D, Lang NP (2008) Ridge augmentation by applying bioresorbable membranes and deproteinized bovine bone mineral: a report of twelve consecutive cases. Clin Oral Implants Res 19(1): 19-25.
-
Urban IA, Nagursky H, Lozada JL (2011) Horizontal ridge augmentation with a resorbable membrane and particulated autogenous bone with or without anorganic bovine bone-derived mineral: a prospective case series in 22 patients. Int J Oral Maxillofac Implants 26(2): 404- 414.
-
Urban IA, Nagursky H, Lozada JL, Nagy K (2013) Horizontal ridge augmentation with a collagen membrane and a combination of particulated autogenous bone and anorganic bovine bone-derived mineral: a prospective case series in 25 patients. Int J Periodontics Restorative Dent (3): 299-307.
-
Beitlitum I, Artzi Z, Nemcovsky CE (2010) Clinical evaluation of particulate allogeneic with and without autogenous bone grafts and resorbable collagen membranes for bone augmentation of atrophic alveolar ridges. Clin Oral Implants Res 21(11): 1242-1250.
-
Beitlitum I, Sebaoun A, Nemcovsky CE, Slutzkey S (2018) Lateral bone augmentation in narrow posterior mandibles, description of a novel approach, and analysis of results. Clin Implant Dent Relat Res 20(2): 96-101.
-
Mir Mari J, Wui H, Jung RE, Hämmerle CHF, Benic GI (2016) Influence of blinded wound closure on the volume stability of different GBR materials: an in vitro cone-beam computed tomographic examination. Clin Oral Implants Res 27(2): 258-265.
-
Mir Mari J, Benic GI, Castellón EV, Hämmerle CHF, Jung RE (2017) Influence of wound closure on the volume stability of particulate and non-particulate GBR materials: an in vitro cone-beam computed tomographic examination Part II. Clin Oral Implants Res 28(6): 631- 639.
-
Ronda M, Rebaudi A, Torelli L, Stacchi C (2014) Expanded vs. dense polytetrafluoroethylene membranes in vertical ridge augmentation around dental implants: a prospective randomized controlled clinical trial. Clin Oral Implants Res 25(7): 859-866.
-
César Neto JB, Cavalcanti MC, Sapata VM, Pannuti CM, Hämmerle CHF, et al. (2020) The positive effect of tenting screws for primary horizontal guided bone regeneration: A retrospective study based on cone-beam computed tomography data. Clin Oral Implants Res 31(9): 846-855.
-
Azpur GM, Jaime FS, Angeles R, Danesh Sani SA, Delgadillo GM, et al. (2019) Biomechanical Effect of Masticatory Forces in Tenting Screws Used for Vertical Ridge Augmentation. J Oral Implantol 45(2): 165-170.
-
Mordenfeld A, Johansson CB, Albrektsson T, Hallman M (2014) A randomized and controlled clinical trial of two different compositions of deproteinized bovine bone and autogenous bone used for lateral ridge augmentation. Clin Oral Implants Res 25(3): 310-320.
-
Speer DP, Chvapil M, Eskelson CD, Ulreich J (1980) Biological effects of residual glutaraldehyde in glutaraldehyde-tanned collagen biomaterials. J Biomed Mater Res 14(6): 753-764.
-
Wiebe D, Megerman J, L’Italien GJ, Abbott WM (1998) Glutaraldehyde release from vascular prostheses of biologic origin. Surgery 104(1): 26-33.
-
Rothamel D, Schwarz F, Sculean A, Herten M, Scherbaum W, et al. (2004) Biocompatibility of various collagen membranes in cultures of human PDL fibroblasts and human osteoblast-like cells. Clin Oral Implants Res 15(4): 443-449.
-
Chen G, Sato T, Ohgushi H, Ushida T, Tateishi T, et al. (2005) Culturing of skin fibroblasts in a thin PLGA- collagen hybrid mesh. Biomaterials 26(15): 2559-2566.
-
Veríssimo DM, Leitão RFC, Figueiró SD, Góes JC, Lima V, et al. (2015) Guided bone regeneration produced by new mineralized and reticulated collagen membranes in critical-sized rat calvarial defects. Exp Biol Med Maywood 240(2): 175-184.
-
Whetman J, Mealey BL (2016) Effect of Healing Time on New Bone Formation after Tooth Extraction and Ridge Preservation with Demineralized Freeze-Dried Bone Allograft: A Randomized Controlled Clinical Trial. J Periodontol 87(9): 1022-1029.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells