Efficacy of Biofilm Removal in Root Canals Using a Polyamide Tip Oscillating with a Frequency in kHz
Background: This study aimed to verify the effectiveness of polyamide tips oscillating with a frequency in the kHz range in removing intraradicular biofilms formed in vivo. Materials and Methods: An intracanal biofilm model was established using the mandibular first molar of 10-week-old male Wistar rats to compare the efficacy of a polyamide tip oscillating with a frequency in kHz (EDDY) in removing biofilms from the root canal. Biofilm removal efficacy was compared between the following groups: EDDY, conventional needle irrigation (CNI), without irrigation (positive control), and no root canal treatment (negative control). The biofilm removal efficacy was investigated using scanning electron microscopy (SEM) of the root canal wall and quantitative polymerase chain reaction for the statistical evaluation of the number of bacteria in each group. Results: SEM of the root canal wall in the CNI and positive control groups showed multi-layered biofilms, whereas the EDDY group showed less or no biofilms at the opening of the dentinal tubules in the root canal wall. Quantitative analysis showed the EDDY group had statistically significantly lower bacterial counts than the positive control group, with no difference when compared to the negative control group. Although the EDDY group had fewer bacteria remaining than the CNI group, the difference was not statistically significant. Conclusion: A polyamide tip oscillating with a frequency in the kHz range, such as EDDY, is an effective strategy for biofilm removal from the root canal, not only by agitating the irrigant but also by mechanical action on the root canal wall.
Introduction
Apical periodontitis is caused by a bacterial infection, and its by-products induce an inflammatory response resulting in bone destruction [1]. In recurrent apical periodontitis, microorganisms form a biofilm on the root canal wall [2], which is resistant to antimicrobial agents such as NaOCl [3], antibiotics, and chlorhexidine [4]. Thus, once a biofilm is formed, its removal and inactivation requires more effort than the removal of planktonic bacteria. Most biofilm studies have been conducted in vitro or ex vivo, and most of the studies have used mono-bacterial species in artificial biofilms, which do not reflect the actual human environment [5]. Therefore, in this study, a root canal biofilm was introduced into rat mandibular, and a biofilm removal model was established with an apical diameter instrumentation up to #30–35, which reflects the clinical situation in humans.
Mechanical debridement employs cutting instruments to remove the infected dentinal material from the root canals [6]; however, because of the anatomical complexity of the root canal system [7], sources of residual infection persist on non-negotiable surfaces [8]. The conventional needle irrigation (CNI) method uses a syringe and a fine needle to deliver irrigants into the root canal. Although CNI is widely utilized, its limitations are also evident [9, 10, 11, 12]. The organic dissolving action of NaOCl, which is used for chemical cleaning, would be expected to act on the extracellular polysaccharides that comprise the biofilm [13]. However, the deliverability of chemicals by CNI has limitations [9, 10] and the required chemical effect cannot be obtained.
Ultrasonic and sonic vibrations have been used to agitate the irrigant in the root canals to reach a wider area. In ultrasonic-activated irrigation (UAI), a metal tip operates at a frequency in the range of 25–30 kHz, which causes acoustic streaming around the tip to agitate the irrigant [14]. However, inserting the metal tip near the root apex is difficult in curved root canals [15], and there is a risk of unnecessary removal of the dentine [16]. Sonic-activated irrigation (SAI) is based on acoustic streaming agitation using a frequency of 1–6 kHz, which is lower than that used in UAI [17]. Recently, SAI using polyamide tips (EDDY, VDW, Munich, Germany) for root canal agitation has been introduced to the market, and a high root canal irrigation effect has been reported [18]. The polyamide tip is characterised by a low elastic modulus that can follow the curved root canal without preparing the canal wall [19]. SAI also involves a larger tip amplitude than that employed in UAI18. Hence, oscillation of polyamide tips with a frequency in the kHz range may achieve effective biofilm removal, through not only agitation of the irrigant but also direct contact with a wider area of the root canal wall for the propagation of vibratory force.
With the current instrumentation and irrigation methods, a reliable method for removing biofilms (which cause refractoriness to treatment), is required [20]. This study aimed to verify whether polyamide tips with an oscillatory frequency in the kHz range are effective as a novel root canal treatment technique for biofilm removal by developing a rat intraradicular biofilm model and evaluating the efficacy of biofilm removal.
Materials and Methods
Ethics Statement
This study was approved by [details removed] (approval no. [details removed]), and all animal experiments were conducted in compliance with the Declaration of Helsinki and the Regulations for Animal Experiments and Related Activities of [details removed]. All interventions were performed after sedation and anaesthesia induced using medetomidine hydrochloride (0.15 mg/kg), midazolam (2.0 mg/kg), and butorphanol tartrate (2.5 mg/kg) to minimise pain. In this study, a total of 48 roots (including mesial and distal roots of the mandibular left and right first molars) from twelve 10-week-old male Wistar rats were examined, and the effectiveness of biofilm removal was verified using an intraradicular biofilm model.
Developing a Rat Intraradicular Biofilm Model
The experimental protocol is illustrated in Figure 1. All procedures were performed using surgical loupes with an LED (Microloupe, MicroTech. Corp, Tokyo, Japan). The root canal procedure was conducted under rubber dam isolation using a customised rat clamp (YDM, Saitama, Japan) and rubber dam sheet (Premium Rubber Dam, KULZER, South Bend, USA). The access cavity was prepared using a bur (Jet Carbide Bar, Shofu, Kyoto, Japan) and an electric motor (VIVAMATE G5, NSK, Tochigi). The pulp was removed using K files and enlarged using nickel-titanium instruments (ProGlider, Dentsply Sirona, Charlotte, NC, USA, and Profile, Dentsply Sirona). Root canal instrumentation was conducted using Tri Auto ZX2 (Morita Corporation, Kyoto, Japan) at 300 rpm and 1.0 Ncm torque limit, while monitoring the tip location of the instruments. The mesial and distal roots were enlarged up to #30 and .04 taper and #35 and .04 taper, respectively. During the procedure, debris and pulp tissue were rinsed with distilled water using a syringe (Nipro syringe, NIPRO, Osaka, Japan) and a needle (Navitip Sideport 31G, 21 mm, ULTRADENT, South Jordan, USA). After root canal instrumentation, the canals were kept exposed to the oral environment for two weeks to inoculate oral bacteria. The root canals were then sealed with a hydraulic sealing material (Caviton, G.C., Tokyo, Japan) and maintained in an anaerobic environment for four weeks to allow biofilm maturation.
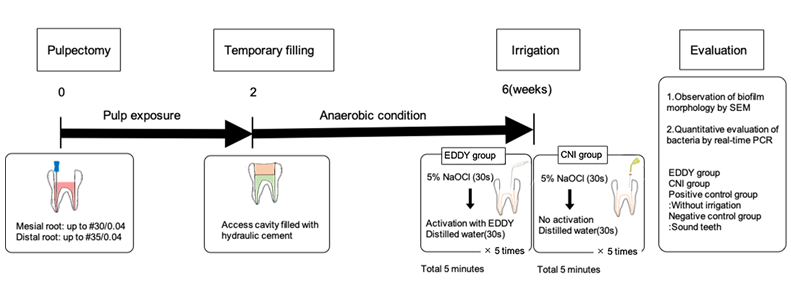
Figure 1: Outline of the experiment. Biofilm models were established on the mesial and distal roots of the left and right mandibular first molars of 12-week-old male Wistar rats. After pulpectomy, the canal was exposed to the oral environment for two weeks and to an anaerobic intracanal environment for four weeks to allow bacterial biofilm maturation. Six weeks after pulpectomy, the root canals were irrigated using a polyamide tip oscillating in a kHz frequency (EDDY) and CNI. After root canal irrigation, the morphology of the intracanal biofilm was observed using SEM, and the residual bacteria in the root canal were quantitatively evaluated using qPCR. CNI, Conventional needle irrigation; SEM, scanning electron microscopy; qPCR, quantitative polymerase chain reaction.
Irrigation Protocol
Six weeks after root canal instrumentation, the rats were euthanised. We dissected the left and right jawbones and removed the temporary sealing material using an ultrasonic scaler (Varios 970, NSK, Tochigi). One tooth exhibited root fracture; therefore, the two root canals were excluded from subsequent experiments. Subsequently, the following procedures were performed: As each root canal in the mesial and distal roots was considered an independent experimental subject, when one was treated, the other was temporarily sealed with a hydraulic temporary sealing material. In the EDDY group, syringe irrigation with 5% NaOCl and agitation using EDDY with distilled water were performed repeatedly. EDDY was inserted up to the working length. While EDDY was being used, distilled water was continuously supplied using a syringe. Five cycles of NaOCl syringe rinsing and agitation using EDDY were performed for a total of 5 min. Finally, the canal was rinsed with distilled water. In the CNI group, rinsing with 5% NaOCl for 30 s was followed by a similar 30 s rinse with distilled water for 5 cycles for a total of 5 min. The canals were then rinsed with distilled water. Each group included seven mesial and seven distal canals. When one root canal was cleaned, the other was temporarily sealed to prevent contamination. The positive control group (mesial root canal, n = 5; distal root canal, n = 5) underwent only canal instrumentation and biofilm maturation. The negative control group (mesial root canal, n = 4; distal root canal, n = 4) included sound teeth. Animals in this group did not undergo access cavity preparation or irrigation. After irrigation, the first molars were extracted from the jawbone and the mesial and distal roots were collected individually. Subsequently, scanning electron microscopy (SEM) and quantitative polymerase chain reaction (qPCR) were performed for morphological observation of the root canal wall and bacterial quantification, respectively.
Morphological Evaluation of the Biofilm using SEM
The biofilm morphology of root canals in the EDDY (mesial root canal, n = 1; distal root canal, n = 1), CNI (mesial root canal, n = 1; distal root canal, n = 1), and positive control groups (mesial root canal n = 1, distal root canal n = 1) was assessed using SEM. One canal from each group was treated. The roots were divided into halves buccolingually and soaked in 2.5% glutaraldehyde to fix the intracanal biofilm. Next, they were washed with phosphate buffered saline, treated with 1-ethyl-3-methyl-imidazoliumtetrafluoroborate, dried in a vacuum desiccator for 1 day, and sputter-coated with platinum. The centre of the root was magnified to observe biofilm formation and the dentinal tubules using a 10 kV SEM (VE-8800, Keyence Inc., Osaka, Japan) at 30×, 500×, 1000×, and 3000× magnifications.
Bacterial quantification using qPCR
All the remaining samples were used for the quantification of bacteria. The roots surface were cleaned with 0.5% NaOCl to prevent contamination, then roots were frozen at -20 °C and ground in an SK mill (Tokken, Chiba, Japan) to obtain powder samples. The total DNA was extracted from each powdered root sample using the Cica Geneus DNA extraction kit (KANTO Chemical Co., Tokyo, Japan), according to the manufacturer’s instructions. The presence of bacteria in the roots was verified by qPCR using the bacterial primers 357F
and 908R22. These assays were performed using a real-time PCR kit (CFX Connect; Bio-Rad Laboratories, Hercules, CA, USA). Amplifications were conducted for 40 cycles at 95 °C for 15 s, followed by 65 °C for 1 min, and fluorescence signals were measured at the end of each cycle. A standard curve was obtained by subjecting 10-fold dilutions of a known concentration of E. faecalis DNA to the same qPCR protocol. Bacterial counts for all experimental groups were calculated using threshold cycle values plotted against a standard curve.
Statistical Analysis
For statistical analysis of the bacterial counts in each experimental group, multiple comparisons were performed using the Tukey test after confirming the normal distribution of the data using the Shapiro–Wilk test. Prism9 (GraphPad Software, San Diego, CA, USA) was used for statistical analysis, with a significance level of α = 0.05.
Results
Morphological observation of the biofilm using SEM
Figure 2 shows the cross-sectional view of the specimens and SEM images of the biofilm remnants. Images of both the mesial and distal roots are shown. In the positive control group, the typical accumulated biofilm is shown for mesial (c-1 to 5) and distal (f-1 to 5) roots.

Figure 2: Morphology of the biofilm in the root canal and observation of dentinal wall after irrigation using scanning electron microscopy. Root canals in the positive control groups (c) and (f) were found to have layered biofilm formation on the walls. Those in the EDDY group (a) had a layer of biofilm (consisting mainly of cocci aggregates) on the walls that obliterated the opening of the dentinal tubules. After using EDDY (d), the biofilm was removed, and the patency of the dentinal tubules was re-established. As seen in (d-2), the curved morphology of the canals was maintained from the cervical to apical parts, and no perforations or fractures were observed. As seen in (d-5), the morphology of the dentinal tubule opening was maintained, and no evidence of unnecessary cutting in the form of waves was observed. In the CNI group (b), the biofilm, an aggregate of cocci and rods, persisted in layers on the root canal walls and obliterated the opening of the dentinal tubules. CNI, conventional needle irrigation High-magnification images showed that regardless of the enlarged canal size, the biofilm structure was layered, consisting mainly of spherical bacteria with some aggregating rod-shaped bacteria (c-3 to 5 and f-3 to 5). Although no biofilm-like deposits were visible in a mesial root canal of the EDDY group (a-1), thin biofilm structures covering the root canal were seen in SEM (a-2 to 5). On the other hand, distal roots showed the removal of biofilm structures throughout the root canal visually (d-1 to 4), no wave-like cutting marks were evident with opening of the dentinal tubules (d-5). The biofilm structure was also similar to the specimens in the positive control group, regardless of the size of root canal enlargement (b-1 to 5 and e-1 to 5).
Bacterial Quantification using qPCR
Figure 3 shows the number of bacteria remaining in the mesial (Figure 3a) and distal (Figure3b) root canals of each group. The EDDY group (mesial root canal, 2.3× 10-2 ng; distal root canal, 4.6×10-3ng) had statistically significantly lower bacterial counts than the positive control group (mesial root canal, 2.9× 10-1; distal root canal, 5.1× 10-1ng) for both mesial and distal root canals (p < 0.05), with no significant difference when compared to the negative control groups (mesial root canal, 3.3× 10-4ng; distal root canal, 1.4× 10-4ng). Although the EDDY group had fewer bacteria remaining in both the mesial and distal root canals compared to the CNI group (mesial root canal, 1.6× 10-1ng; distal root canal, 1.8× 10-1ng), the difference was not statistically significant.
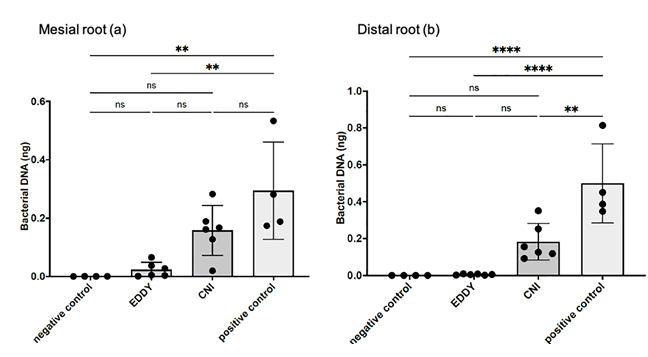
Figure 3: Quantitative evaluation of bacteria by qPCR. Bacterial counts were significantly higher in the positive control group than in the negative control group, indicating biofilm formation in the positive control group, because the negative control group was not infected with bacteria. Bacterial counts were significantly lower in the EDDY group in both the mesial and distal roots than in the positive control group. There was no significant difference in the number of remaining bacteria in both the mesial and distal roots between the EDDY and negative control groups.
Discussion
Biofilms are strongly associated with persistent apical periodontitis; thus, a reliable treatment method for removing them is essential to improve outcomes in recurrent cases. Further, 77% of recurrent cases showed the presence of a residual biofilm in the root canal [2]. This shows that conventional treatment methods are ineffective for biofilm removal. The results of this study using the established rat intraradicular biofilm model showed that the polyamide tip oscillating in the kHz range could remove the biofilm without altering the root canal morphology, indicating that it is a compelling new biofilm removal technique.
Once the biofilm is set as the treatment target, an optimised treatment technique is necessary. The lack of reliable in vitro and ex vivo experimental biofilm models is an issue; however, some inconsistent results have been obtained [21, 22]. Concerns such as bacterial species, biofilm morphology, and introduction duration exist while using in vitro and ex vivo models. In vivo models can be implemented in an environment that mimics the maturation process of human biofilms such as infection from the oral cavity, attachment and growth in the root canal, anaerobic environment, and maturation. Therefore, an in vivo model was considered appropriate for treatment evaluation.
The rat intraradicular biofilm model established in this study was a successful in vivo model. The protocol for biofilm introduction was based on a previous study [23]. Although
bacteriological characterisation was not conducted, the root canal biofilm had a typical biofilm morphology, with cocci and bacilli aggregating with a layered structure. In addition, instruments used in human clinical practice, such as rubber dam isolation and nickel-titanium files were used in this model, allowing for similar root canal preparation as is done in human patients. Therefore, this model was used to explain the optimisation of new treatment techniques intended for biofilm removal.
Applying a polyamide tip oscillating with a frequency in the kHz range in the root canal was effective for biofilm removal. The apical diameters of the #30 and #35 instrumented root canals were 0.30 mm and 0.35 mm, respectively, allowing sufficient space for the polyamide tip with a diameter of 0.2 mm to oscillate inside the root canal. The primary mechanism of root canal cleaning with polyamide tips is agitation of the irrigant caused by acoustic streaming around the tip [18, 24]. However, complete biofilm removal is difficult and achieved only by increasing the flow velocity which increases the water pressure on the root canal wall [25]. Sonic oscillation with polyamide tips generally has a larger amplitude than ultrasonic oscillation [26], and can directly reach a wider root canal area. In contrast to conventional UAI and SAI tips, which mainly oscillate in one direction [27], the EDDY tip has an oval oscillation trajectory [28], suggesting that tip oscillation is distributed over the entire circumference, reaching a wider area of the root canal wall. SEM showed that the biofilm remained and accumulated over the dentin tubules in the mesial root with instruments up to #30, while an opening of the dentin tubules was observed distally with #35 instrumentation following biofilm removal. Although qPCR showed that the bacterial counts decreased in both instrumentation groups, the morphological observations showed that enlargement to #35 was effective for EDDY to successfully remove the biofilm. Therefore, a new technology that enables effective biofilm removal by optimising amplitude and frequency using a polyamide tip oscillating in the kHz range can be developed.
A polyamide tip oscillating with a frequency in the kHz range is an effective strategy for biofilm removal, which was achieved not only by agitating the irrigant but also by mechanical action on the root canal wall. Optimising the frequency, amplitude, and tip material would be a practical approach to developing a new root canal treatment technique capable of removing biofilm. Conflicts of Interest: The authors have no conflicts of interest relevant to this article. Acknowledgements: This work was supported by a Grant- in-Aid for Scientific Research (C) from the Japan Society for Promotion of Science (Grant Number 20K09970). The funding source had no role in any part of the research process.
References
-
Fabricius L, Dahlén G, Sundqvist G, Happonen RP, Möller AJ (2006) Influence of residual bacteria on periapical tissue healing after chemomechanical treatment and root filling of experimentally infected monkey teeth. Eur J Oral Sci 114(4): 278-285.
-
Ricucci D, Siqueira JF Jr (2010) Biofilms and apical periodontitis: study of prevalence and association with clinical and histopathologic findings. J Endod 36(8): 1277-1288.
-
Metzger Z, Solomonov M, Kfir A (2013) The role of mechanical instrumentation in the cleaning of root canals. Endod Topic 29(1): 87-109.
-
de Paz LEC (2007) Redefining the persistent infection in root canals: possible role of biofilm communities. J Endod 33(6): 652-662.
-
Swimberghe RCD, Coenye T, De Moor RJG, Meire MA (2019) Biofilm model systems for root canal disinfection: a literature review. Int Endod J 52(5): 604-628.
-
Wu MK, van der Sluis LW, Wesselink PK (2003) The capability of two hand instrumentation techniques to remove the inner layer of dentine in oval canals. Int Endod J 36(3): 218-224.
-
Peters OA (2004) Current challenges and concepts in the preparation of root canal systems: a review. J Endod 30(8): 559-567.
-
Peters OA, Schönenberger K, Laib A (2001) Effects of four Ni-Ti preparation techniques on root canal geometry assessed by micro computed tomography. Int Endod J 34(3): 221-230.
-
Khademi A, Yazdizadeh M, Feizianfard M (2006) Determination of the minimum instrumentation size for penetration of irrigants to the apical third of root canal systems. J Endod 32(5): 417-420.
-
De Deus G, Barino B, Marins J, Magalhães K, Thuanne E, et al. (2012) Self-adjusting file cleaning-shaping-irrigation system optimizes the filling of oval-shaped canals with thermoplasticized gutta-percha. J Endod 38(6): 846-849.
-
Peeters HH, Gutknecht N (2014) Efficacy of laser-driven irrigation versus ultrasonic in removing an airlock from the apical third of a narrow root canal. Aust Endod J 40(2): 47-53.
-
Tay FR, Gu LS, Schoeffel GJ, Wimmer C, Susin L, et al. (2010) Effect of vapor lock on root canal debridement by using a side-vented needle for positive-pressure irrigant delivery. J Endod 36(4): 745-750.
-
Ye WH, Fan B, Purcell W, Meghil MM, Cutler CW, et al. (2018) Anti-biofilm efficacy of root canal irrigants against in-situ Enterococcus faecalis biofilms in root canals, isthmuses and dentinal tubules. J Dent 79: 68-76.
-
van der Sluis LWM, Versluis M, Wu MK, Wesselink PR (2007) Passive ultrasonic irrigation of the root canal: a review of the literature. Int Endod J 40(6): 415-426.
-
Walmsley AD, Williams AR (1989) Effects of constraint on the oscillatory pattern of endosonic files. J Endod 15(5): 189-194.
-
Plotino G, Pameijer CH, Grande NM, Somma F (2007) Ultrasonics in endodontics: a review of the literature. J Endod 33(2): 81-95.
-
Gu LS, Kim JR, Ling J, Choi KK, Pashley DH, et al. (2009) Review of contemporary irrigant agitation techniques and devices. J Endod 35(6): 791-804.
-
Neuhaus KW, Liebi M, Stauffacher S, Eick S, Lussi A (2016) Antibacterial efficacy of a new sonic irrigation device for root canal disinfection. J Endod 42(12): 1799- 1803.
-
Kucher M, Dannemann M, Modler N, Hannig C, Weber MT (2019) Effects of endodontic irrigants on material and surface properties of biocompatible thermoplastics. Dent J 7(1): 26.
-
Retsas A, Dijkstra RJB, van der Sluis L, Boutsioukis C (2022) The effect of the ultrasonic irrigant activation protocol on the removal of a dual-species biofilm from artificial lateral canals. J Endod 48(6): 775-780.
-
Bryce G, MacBeth N, Gulabivala K, Ng YL (2018) The efficacy of supplementary sonic irrigation using the EndoActivator system determined by removal of a collagen film from an ex vivo model. Int Endod J 51(4): 489-497.
-
Ordinola Zapata R, Bramante CM, Aprecio RM, Handysides R, Jaramillo DE (2014) Biofilm removal by 6% sodium hypochlorite activated by different irrigation techniques. Int Endod J 47(7): 659-666.
-
Tanaka T, Yahata Y, Handa K, Venkataiah SV, Njuguna MM, et al. (2021) An experimental intraradicular biofilm model in the pig for evaluating irrigation techniques. BMC Oral Health 21(1): 177.
-
Park SY, Kang MK, Choi HW, Shon WJ (2020) Comparative analysis of root canal filling debris and smear layer removal efficacy using various root canal activation systems during endodontic retreatment. Medicina 56(11): 615.
-
Yamada J, Takiguchi T, Saito A, Odanaka H, Soyama H, et al. (2017) Removal of Oral Biofilm on an implant fixture by a cavitating jet. Implant Dent 26(6): 904-910.
-
Swimberghe RCD, De Clercq A, De Moor RJG, Meire MA (2019) Efficacy of sonically, ultrasonically and laser- activated irrigation in removing a biofilm-mimicking hydrogel from an isthmus model. Int Endod J 52: 515- 523.
-
Jiang LM, Verhaagen B, Versluis M, van der Sluis LW (2010) Evaluation of a sonic device designed to activate irrigant in the root canal. J Endod 36(1): 143-146.
-
Gankerseer EJ, Walmsley AD (1987) Preliminary investigation into the performance of a sonic scaler. J Periodontol 58(11): 780-784.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells