Temporomandibular Joint Osteoarthritis Exacerbates with Restored Teeth: A Cadaveric Case Report
The objective of this case report is to begin to investigate the correlations between gross signs and symptoms of osteoarthritis (OA) on cadaveric temporomandibular joints (TMJs) and the restorative care a patient experienced prior to death. Two cadaveric donors (88-years-old male and 93-years-old female) were investigated by classical dissection for gross symptoms of OA on the mandibular condyle and the mandibular fossa using a validated scale for OA disease severity. A Grade 0-4 disease severity score was awarded to the unilateral condyle and mandibular fossa for each patient. An oral exam was performed to assess restorative changes to the dentition. Both patients demonstrated Grade 4 (severe) OA on the mandibular fossa and condyle. This is a finding documented to only affect 23% (7/31) of a previous research cohort of donors; the mandibular fossa typically presents with more severe disease findings compared to the condyle. These specific donors were selected for TMJ disease assessment as a preliminary oral examination revealed substantial restorative findings. Excluding removal of the third molars, the male donor was charted to have 1 missing tooth and 11 restored teeth whereas the female donor was charted to have 17 missing teeth and 11 restored teeth. The 93-years-old female demonstrated a visibly more profound state of disease on the fossa and condyle of the TMJ compared to any other donor assessed by this protocol to date; the fossa demonstrated complete cartilage loss with a substantial concavity on the articular eminence, the condyle was flattened and the articular disc was effectively absent minus a thin fibrocartilaginous ring. It could be concluded that this substantial degree of TMJ OA disease severity, based on this specific validated scale, may relate to a high quantity of restored teeth and may manifest uniformly between the sexes.
Introduction
Osteoarthritis (OA) is the most common degenerative joint disease, affecting over 300 million people worldwide and over 32.5 million adults in the United States [1, 2]. OA presents with chronic degeneration of features of synovial joints including the articular cartilage, ligaments and fibrocartilaginous structures such as menisci or articular discs. The disease was previously understood to be a pathology of “wear and tear” but is now discussed as a multifactorial syndrome produced by dysregulated inflammatory signaling and tissue remodeling [3, 4]. Cadaveric dissection of synovial joints, including the temporomandibular joint (TMJ), demonstrates visible symptoms of OA including fibrillations, linear cracks, erosions and large crater-like degenerations which exposure and allow for damage to the underlying cortical bone [5, 6]. Regardless of the specific synovial joint affected, OA typically presents with pain, joint stiffness and defective functionality that decreases patient quality of life [7, 8].
The TMJ represents a bilateral articulation between the mandibular condyle and the mandibular fossa of the temporal bone; it is a synovial joint divided into an upper and a lower joint compartment with an articular disc separating the two. The integrity of the TMJ is crucial to patient health and has a strong influence on the practice of dentistry [9]. Temporomandibular joint disorders (TMDs) affect between 5-12% of Americans and as many 31% of the elderly population [7, 8]. There are three types of TMDs: muscular disorders, disc disorders and joints disorders. OA presenting in the TMJ is a common joint disorder that may produce decreased range of mandibular motion, audible joint noises, pain, stiffness and other functional abnormalities [8]. Currently, the literature pool related to TMJ OA is limited. Basic information related to morphometric symptom presentation, prevalence of specific gross symptoms and patient demographic, clinical history and lifestyle correlates to symptoms are in the early phases of discovery. The objective of this case report is to begin to investigate the gross signs and symptoms of OA in cadaveric TMJs and compare severe findings to the restorative care a patient experienced prior to death.
Methods
Two donors utilized for educational dissection at the University of Nevada Las Vegas (UNLV) were selected for a case report-style investigation to begin to draw conclusions on TMJ OA gross symptoms and restorative dental procedures performed on the donor prior to death. An abbreviated oral exam was performed by 2nd year dental students and a postgraduate dentist participating in a residency program for orthodontics and dentofacial orthopedics to assess the quantity of missing teeth and the quantity of restored teeth. These two particular donors, a 93-years-old female and an 88-years-old male, were selected for the case report-style assessment based on the severe TMJ OA they demonstrated on dissection.
TMJs were dissected from the cadaveric skulls after the calvaria and brain had been removed. Soft tissue dissection removed the muscles of mastication, muscles of facial expression and the parotid gland from the lateral face to expose the ramus and neck of the mandible; the neck was bisected with an autopsy saw to free the TMJ inferiorly. Parallel saw cuts were made through the greater wing of the sphenoid bone and the squamous part of the temporal bone to the depth of the medial margin of the mandibular fossa. Force was applied to the residual greater wing of the sphenoid bone to break the floor of the middle cranial fossa medial to the TMJ to free to joint superiorly. Fine dissection was performed to remove any residual soft tissue, perforate the joint capsule and expose the upper and lower joint compartments. The articular disc was freed from the mandibular condyle by bisecting the collateral ligaments of the joint with a scalpel. Articular cartilage and the articular disc were then easily visualized.
A validated disease severity scale was utilized to score the symptoms of OA on the mandibular condyle and the mandibular fossa of each donor using a Grade 0-4 classification system [9]. Each grade for disease severity has specific gross symptoms associated with its designation (Table 1). Strong statistical interrater reliability has been demonstrated for the use of this scale in assessing OA disease severity on the femoral condyles [10] and in a pilot cohort of TMJs through the use of the Krippendorff’s alpha (Kα) test (condyle Kα = .9353; fossae Kα = .9816). The two donors selected for this investigation each scored a Grade 4 for the mandibular condyle and the mandibular fossa to indicate their severe state of disease.
| Characterization | Surface Features | |
|---|---|---|
| 0 | Normal Cartilage | No visible changes |
| 1 | Questionable if OA is present | Slight unevenness, granularity of the surface, shallow furrows or streaking |
| 2 | Mild OA | Superficial fraying, superficial splitting, superficial pitting |
| 3 | Moderate OA | Extensive ulceration, cartilage loss |
| 4 | Severe OA | Large areas of complete degeneration, accompanied by exposure and eburnation of bone |
Table 1: Scale modified from Kolver, et al 2004 to be implemented in the knee joint and the TMJ.
Results
The female donor demonstrated the most severe symptoms assessed in a pilot study on cadaveric TMJ OA carried out by this team of authors (N=31). The donor’s mandibular condyle and mandibular fossa were awarded a Grade 4 disease severity based on severe cartilage erosions present and the accompanying damages to the underlying cortical bone. The articular disc was completely worn through; the only dissectible remnant was a thin fibrocartilaginous ring of tissue adhered to the condyle (Figure 1A). Figures 1B-C demonstrate the severe symptoms seen on the condyle.
Figure 1D-E demonstrates the severe symptoms seen on the fossa. Forceps flank the major cartilage and bony erosion on the articular eminence that presents as a large concavity in the middle of the eminence. The represents a tremendously severe example of a bony deformity in the mandibular fossa. This donor demonstrated 17 missing teeth (60.7% of the natural dentition excluding the third molars) and 11 restored teeth (39.3% of the natural dentition excluding the third molars). The donor had predominantly porcelain fused to metal (PFM) crowns.
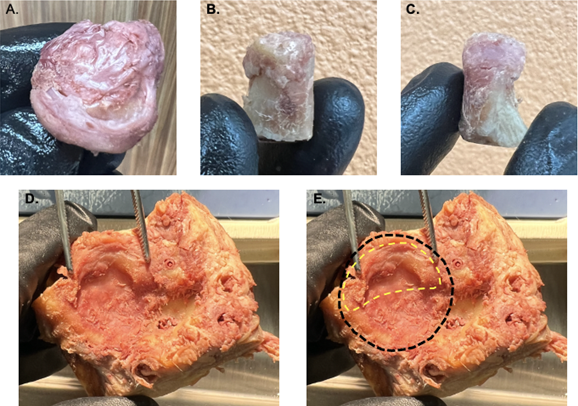
Figure 1: Demonstrates the disease severity of the mandibular condyle, fossa and articular disc on the 93-years-old female donor. (A.) Image represents the donor’s right mandibular condyle with remnants of the remaining, degenerated articular disc. The condyle’s articular cartilage demonstrates severe erosions on the medial (B.) and lateral (C.) aspects. (D.) Image represents the mandibular fossa of the temporal bone with forceps flanking the substantial bony erosion on the articular eminence (E.) Represents the approximate total surface area (black dashed line) of the mandibular fossa with an approximation of the pre- degeneration margin of the articular eminence (yellow dashed line).
TMJ OA symptoms were scored comparably on an 88-years-old male donor compared to the previously discussed female. The donor’s condyle and fossa were awarded a Grade 4 disease severity based on the severe cartilage erosions that were present and the accompanying damages to the underlying cortical bone. The articular disc was completely worn through although, there was more fibrocartilage remaining to help protect the cartilage of the donor’s articular surfaces compared to the female donor (Figures 2A & B). The donors both received Grade 4 scores for condyle and fossa disease severity but the male donor’s symptoms were visually less extreme (Figures 2C-D). This donor demonstrated 1 missing tooth (3.6% of the natural dentition excluding the third molars) and 11 restored teeth (39.3% of the natural dentition excluding the third molars). The donor had predominantly porcelain fused to metal (PFM) crowns.
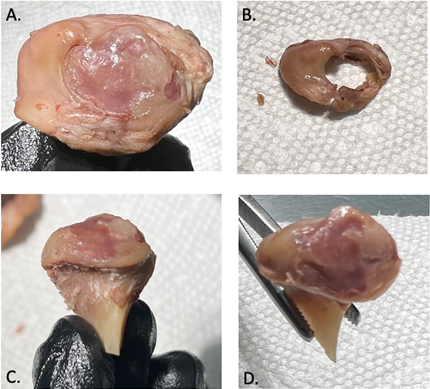
Figure 2: Demonstrates the disease severity of the mandibular condyle, fossa and articular disc on the 88-years-old male donor. (A) Image represents the residual articular disc, represented by a ring of fibrocartilaginous tissue surrounding the circumference of the mandibular condyle. (B) Image represents the articular disc dissected away from the condyle. (C) Image represents an anterior view of the condyle. (D) Image represents a superior view of the substantial cartilage erosions on the condyle.
Discussion
Grade 4 OA was award to the mandibular condyle and the mandibular fossa in only 23% (7/31) of a previously assessed pilot cohort of cadaveric TMJs (16 donors, 31 TMJs). This care report-style investigation aimed to assess the state of these particular donors’ joint anatomy based on their high restoration counts. This case report shows there is potentially a correlation with TMJ OA disease severity and high restoration count and/or missing teeth. These two donors were among the donors with the most severe TMJ OA symptoms in this pilot donor pool; out of 8 donors assessed for restoration changes they also were both in the top half for restoration counts. There may or may not be differences in severity of TMJ OA symptoms between the sexes; further investigation is required. Based on the equivalent disease scoring between these two donors a lack of disparity between male and female TMJ OA severity is plausible. The current literature and the visibly more severe TMJ OA symptoms on the female donor despite receiving the same disease severity scale score may indicate that increasing the number of restorative changes in women may exacerbate symptoms of TMJ OA to a greater extent. Women, especially of childbearing age, are shown to demonstrate OA regularly and associations have been made to mental health [11, 12].
Future directions of this study are related to increasing the donor pool to increase our understanding of morphometric OA lesions and their locations; broadening the donor pool will also ideally extend the age range to help draw patient conclusions. It is unknown as to whether restorative work and/or the loss of dentition encourages the pathogenesis of OA or if OA is driving the loss of dentition and need for restorative work. Based on investigations being carried out on this pilot cohort of donor TMJs and the findings associated with this case report, the authors hypothesize there to be a strong correlation that they aim to establish in future research studies.
References
-
Safiri S, Kolahi AA, Smith E, Hill C, Bettampadi D, et al. (2020) Global, regional and national burden of osteoarthritis 1990-2017: a systematic analysis of the Global Burden of Disease Study 2017. Ann Rheum Dis 79(6): 819-828.
-
Centers for Disease Control and Prevention; Arthiritis Foundation. A national public health agenda for osteoarthritis.
-
Loeser RF, Goldring SR, Scanzello CR, Goldring MB (2012) Osteoarthritis: a disease of the joint as an organ. Arthritis Rheum 64(6): 1697-1707.
-
Xia B, Chen D, Zhang J, Hu S, Jin H, et al. (2014) Osteoarthritis pathogenesis: a review of molecular mechanisms. Calcif Tissue Int 95(6): 495-505.
-
Immonen J, Siefring C, Sanders L (2019) Osteoarthritis of the anterior cruciate ligament and medial tibial plateau: a cadaveric study. Cartilage 10(1): 11-18.
-
Bauer M, Jackson RW (1988) Chondral lesions of the femoral condyles: a system of arthroscopic classification. Arthroscopy 4(2): 97-102.
-
Whittaker JL, Runhaar J, Bierma Zeinstra S, Roos EM (2021) A lifespan approach to osteoarthritis prevention. Osteoarthritis Cartilage 29(12): 1638-1653.
-
Yadav S, Yang Y, Dutra EH, Robinson JL, Wadhwa S (2018) Temporomandibular joint disorders in older adults. Journal of the American Geriatrics Society 66(6): 1213- 1217.
-
Kovler M, Lundon K, McKee N, Agur A (2004) The human first carpometacarpal joint: osteoarthritic degeneration and 3-dimensional modeling. J Hand Ther 17(4): 393- 400.
-
Immonen J, Stevens K, Albin A, Chaus D, Gilmer L, et al. (2021) Assessment of the Degree of Osteoarthritis in Aging Male and Female Femoral Condyles: A Cadaveric Study. Cartilage, 13(1): 1684-1695.
-
Dean L, Churchill B, Ruppanner L (2022) The mental load: building a deeper theoretical understanding of how cognitive and emotional labor over load women and mothers. Community, Work & Family 25(1): 13-29.
-
Garcia Alonso J, Krentz M, Lovich D, Quickenden S (2019) Lightening the mental load that holds women back. Boston Consulting Group pp: 1-6.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells