Polyetherether-Ketone (PEEK) Kennedy Class III Removable Partial Dentures: A case report
Modified poly-ether-ether-ketone (PEEK) is a new material that can be used for patients allergic to metals, or who dislike the metallic taste, the weight, and for patients with aesthetic concerns related to the visibility of the metallic clasps. This polymer would allow increased biocompatibility, durability, and elasticity, as well as more esthetically pleasing results. It has been used for years in orthopedics and medical field. The clinical use of PEEK removable partial denture prosthesis frameworks is presented as an alternative for the conventional metallic prosthesis.
Introduction
The number of partially edentulous adults is increasing and requires replacement of missing teeth [1]. Among the treatment options, removable partial denture (RPD) with Chrome Cobalt frameworks and clasps is considered to be an inexpensive and predictable treatment for the rehabilitation in elderly patients [2].
However, problems related to Cobalt-Chromium (CoCr) alloys traditionally used for removable partial denture construction have been documented [3, 4].
Advances in polymer-based materials and digital fabrication strategies might allow for incorporation of key design features such as rests and indirect and direct retention components [5]. The increased biocompatibility, durability, and elasticity, as well as the most aesthetics and cost-effective benefits, will expand their applications in RPD- based prosthetics [6].
The involvement of computer-aided design/computer- aided manufacturing (CAD/CAM) into the design and fabrication of dental prostheses is more efficient, because it saves materials, less time-consuming, and effort, and includes the possibility of mass production [7]. Polyetheretherketone (PEEK) as a framework material has been reported to be an alternative to base metal alloys in constructing RPDs [8]. PEEK offer high biocompatibility, good mechanical properties, high temperature resistance, and chemical stability [9].
Clinical Report
A 58-year-old male patient presented to the prosthodontics department, DENTAL CLINIC OF MONASTIR (Tunisia), for the replacement of his missing teeth. He had a cardiologic problem, and was taking Aspirin. His chief complaint was the lack of chewing. Clinical examination revealed a maxillary modified Kennedy Cl III arch extending from the existing Canin to the existing 3rd molars bilaterally and the absence of the first lower molar bilaterally (Figures 1a & b).

The Treatment Plan
The treatment options were discussed with the patient, and the treatment plan was established. A maxillary RPD with PEEK framework using EXOCAD milling technology and two RPD flexible were proposed for the replacement of the lower missing teeth.
Preliminary impressions were performed for both arches using irreversible hydrocolloid impression material (CAVEX CA37) in perforated trays. After that, were poured to obtain study casts on which acrylic custom tray was made using light-cured resin (Figure 2).

Then the definitive impression was recorded with Polysulfure (PERMLASTIC LIGHT BODY - KERR) and a maxillary definitive cast was obtained (Figures 3 & 4).


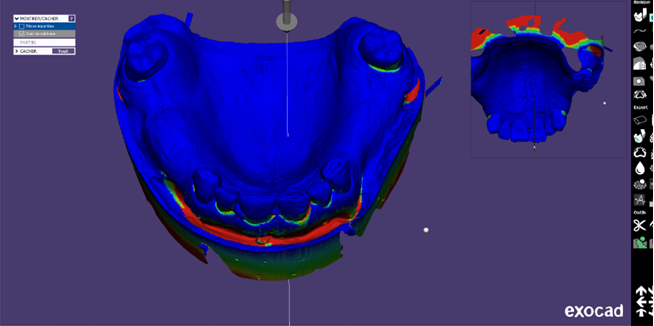
This maxillary cast was then fixed on the scanner table and scanned using a 3D scanner to obtain a virtual model, which was digitally surveyed to determine the most acceptable path of insertion, to draw the survey line on the abutment teeth, and to block out the undesirable undercuts into flattened surfaces (Figure 5).
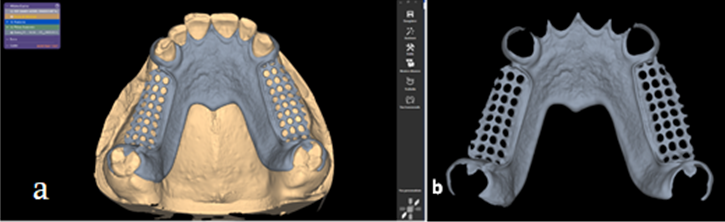
A framework design was planned to include Four Aker clasps on both canines and third molars, “Horse-Shoe” palatal major connector and cingulum rests on the anterior teeth. All components of the framework were selected from a menu and placed in the correct position (Figure 6a) they were a little thickened compared to conventional metallic framework. The complete framework design was checked from all surfaces after finishing and smoothing (Figure 6b).
Then imported into the milling machine to begin milling the medical-grade PEEK dental discs (Figure 7). Once the PEEK dental disk has been milled, the framework was then finished and tried intraorally to check its fit (Figures 8a & b).

Maxilla-mandibular relation was recorded using bite registration wax, stone casts were mounted on a semi- adjustable articulator, and the artificial teeth (Conventional acrylic denture teeth) were arranged respecting the patient occlusion.
The final try-in was made to check the fit, the occlusion and the aesthetic result. The stability and retention were fairly good.
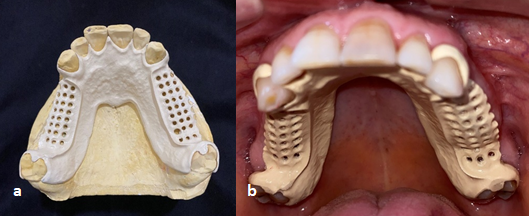
A clinical remount followed by occlusal adjustments was performed to accommodate processing discrepancies and finally, the RPD was delivered to the patient (Figures 9a & b). The latter was pleased and satisfied with restoring his chewing ability.

Discussion
Clinical examination, patient’s demands, and scientific evidence are the main factors to take into consideration when choosing the material for RPDs constructing [5]. In order to avoid unacceptable display of metal clasps, increased prosthesis weight, a potential for metallic taste, and possible allergic reactions, a number of thermoplastic materials were introduced in clinical practice [8].
In this case, the patient rejected treatment with implant- supported prostheses due to cost concerns, fear of additional oral surgery and the more time-consuming needed. The use of a precision attachment also was rejected because of psychological issues related to preparing the natural teeth for crowns.
Correct planning of RPD design according to biomechanical principles is important for maintaining a proper hygiene and less plaque accumulation, and hence would reduce the incidence of carious lesions and periodontal diseases [10].
Due to its cream color and high strength, PEEK permits RPD fabrication with metal-free clasps and occlusal rests providing occlusal stability and enhanced aesthetics [11].
The low weight of PEEK material (It weighed 15 g less than its Cr-Co predecessor) permits the fabrication of lighter prostheses providing high patient satisfaction and comfort during function (Figures 10a & b). However, its fabrication is more expensive than the conventional lost-wax technique and use of metallic RPD frameworks.
This it would be difficult for partially edentulous patients with financial constraints [12]. The retentive force of PEEK clasps could be a matter of concern. According to Hussein T Abed et al, PEEK clasps offer a lower retentive force than metal clasps after 15000 cycles of insertion/removal, which is related to the low modulus of elasticity of the PEEK clasps with increased flexibility compared to Co-Cr clasps, but still sufficient for clinical use at 0.50 and 0.75 mm undercut but not enough at 0.25 mm undercut [13].
However, the authors suggest the use of deeper retentive areas (0.5 mm) or increasing the clasp bulkiness to provide adequate retention for clinical use. PEEK clasps are gentler to the enamel and the porcelain restorative materials than conventional Cr-Co clasps are [14]. Due to its insolubility in water and low reactivity with other materials, PEEK could be a suitable material for patients allergic to Cr-Co, or sensitive to the metallic taste of conventional Cr-Co RPD [15].
Nevertheless a few inconvenient may be encountered with this treatment, including the additional cost of the scanning equipment and CAD software, special training, understanding of digital techniques, and increased waste of the subtractive manufacturing method [16].
As already mentioned, PEEK is a material recently introduced in dentistry. Unfortunately, there is lack of clinical studies evaluating their longevity and resistance to permanent deformation with RPD function as well as their clinical influence on the abutments with long-term use.
Further long-term follow-up studies are needed to consolidate the scientific data.
Conclusion
The use of CAD/CAM technology for the fabrication of an RPD metal-free framework resulted in improving patient satisfaction toward his RPD in terms of function and aesthetics. With adequate patient selection and treatment planning, PEEK can be considered a useful alternative framework material for RPDs restoring partially edentulous patients.
References
-
Jeyapalan V, Krishnan CS (2015) Partial Edentulism and its Correlation to Age, Gender, Socio-economic Status and Incidence of Various Kennedy’s Classes-A Literature Review. J Clin Diagn Res (JCDR) 9(6): 14-17.
-
Behr M, Zeman F, Passauer T, Koller M, Hahnel M, et al. (2012) Clinical performance of cast clasp-retained removable partial dentures: a retrospective study. Int J Prosthodont 25(2): 138-144.
-
Grosgogeat B, Vaicelyte A, Gauthier R, Janssen C, Le Borgne M (2022) Toxicological Risks of the Cobalt– Chromium Alloys in Dentistry: A Systematic Review. Materials 15(17): 5801.
-
Kassapidou M, Stenport VF, Hjalmarsson L, Johansson CB (2017) Cobalt-chromium alloys in fixed prosthodontics in Sweden. Acta Biomater Odontol Scand 3(1): 53-62.
-
Campbell SD, Cooper L, Craddock H, Hyde TP, Nattress B, et al. (2017) Removable partial dentures: The clinical need for innovation. J Prosthet Dent 118(3): 273-280.
-
Harb IE, Abdel Khalek EA, Hegazy SA (2019) CAD/CAM Constructed Poly (etheretherketone) (PEEK) Framework of Kennedy Class I Removable Partial Denture: A Clinical Report. J Prosthodont 28(2): 595-598.
-
Davidowitz G, Kotick PG (2011) The use of CAD/CAM in dentistry. Dent Clin North Am 55(3): 559-570.
-
Zoidis P, Papathanasiou I, Polyzois G (2016) The use of a modifiedpoly-ether-ether-ketone (PEEK) as an alternative framework material for removable dental prostheses. A clinical report. J Prosthodont 25(7): 580- 584.
-
Ortega Martínez J, Farré Lladós M, Cano Batalla J, CabratosaTermes J (2017) Polyetheretherketone (PEEK) as a medical and dental material: A literature review. Medical Research Archives 5(4)
-
Owall B, Budtz Jörgensen E, Davenport J, Mushimoto E, Palmqvist S, et al. (2002) Removable Partial Denture Design: A Need to Focus on Hygienic Principles?. Int J Prosthodont 15(4): 371-378.
-
Hatmode T, Deshmukh K, Pande N, Deshpande S, Radke U, et al. (2021) Metal-free prosthodontics: a overview. JPID 4(3): 126-132.
-
Akl MA, Stendahl C (2022) Removable Partial Denture Frameworks in the Age of Digital Dentistry: A Review of the Literature. Prosthesis 4(2): 184-201.
-
Abed HT, Al Omari AW (2022) Evaluation of Retention Force of Polyetheretherketone (PEEK) and Cast Cobalt- Chromium Circumferential Clasps: A comparative study. Al-Rafidain Dental Journal 22(1): 19-27.
-
Rzanny A, Gobel F, Fachet M (2013) BioHPP summary of results for material tests, Research Report. Jena, Germany, University of Jena, Department of Materials and Technology
-
Qin L, Yao S, Zhao J, Zhou C, Oates TW, et al. (2021) Review on Development and Dental Applications of Polyetheretherketone-Based Biomaterials and Restorations. Materials (Basel) 14(2): 408.
-
Tofail SAM, Koumoulos EP, Bandyopadhyay A, Bose S, O Donoghue L, et al. (2018) Additive manufacturing: scientific and technological challenges, market uptake and opportunities. Materials Today 21(1): 22-37.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells