Assessment of Prevalence and Associated Factors of Oral Lesions among HIV/Aids Patients Attending in Jimma University Medical Center, ART Clinic, Jimma, Oromia, South Western of Ethiopia
Background: HIV/AIDS constitutes a main health problem in worldwide. Oral lesions are among the earliest and most important indicators of infection with human immunodeficiency virus (HIV). The presence of oral lesions has a significant impact on the physical and mental health of the HIV/AIDS patients. Oral lesions in HIV/AIDS are associated with adverse effect on the quality of such as pain, difficulty during eating bad breath, and altered taste. Objective: To assess the prevalence of oral lesions and its associated factors among HIV/ AIDS patients attending in JUMC, ART Clinic 2023. Methods: Institutional based cross- sectional study was conducted with convenient sampling technique in JUMC, ART clinic from June 15- July 15GC, Data was collected by means of Observations, clinical examination, completing questionnaire and also reviewing patient’s medical records to find oral lesions. Results and Discussion: A total of 96 HIV/AIDS patients were examined, the overall prevalence of oral lesions was found to be 46.9% (95% confidence interval). The result indicates that most prevalent oral lesions were pseudomembranous candidiasis 11(11.5%) followed by Oral hairy leukoplakia 8(8.3%) and necrotizing ulcerative periodontitis 6(6.2%). Poor oral hygiene status, mouth rinse practices, smoking cigarette, alcohol usage and chat chewing habits were significantly associated with the prevalence of oral lesions. Conclusion and Recommendation: The study revealed that nearly half of the study participants had oral lesions, with respect to the resulted prevalence in this study (46.9 %), early detection of oral lesions must be emphasized on the diagnosis and early management of HIV/ AIDS patient’s
Introduction
Human immunodeficiency virus (HIV), the lentivirus that causes acquired immunodeficiency syndrome (AIDS), has become one of the most important health and social problem. HIV infection is a major global health problem affecting developing and developed countries alike. More than 1.5 million People globally became newly infected with HIV in 2020 [1]. The WHO African region is the most affected region, accounting for more than two-thirds of people living with HIV worldwide [2].
Our country Ethiopia is the second most popular country in sub- Saharan Africa suffering from the burden of HIV/AIDS. The burden of HIV/AIDS remains high in Ethiopia despite a considerable scale up of comprehensive HIV/AIDS interventions during the (Millennium Development Goals) MDG period. In 2016, there were about 718,500 people living with HIV/AIDS [3]. The 2017 UNAID global AIDS report revealed that the number of new HIV infections in Ethiopia were higher in 2016 than in 2010. The reemergence of HIV/ AIDS in Ethiopia could be due to the low coverage of high impact interventions [4]. Oral lesions are common in patients infected with HIV/AIDS and are often the presenting feature. The fact that HIV is not a notifiable disease emphasizes the clinical importance of oral HIV lesions to both physician &the patients [5]. Oral lesions that are associated with this disease are important, because they affect the quality of life of the patient and are useful markers of disease progression and immunosuppression. Oral lesions in HIV infection have been well documented in developed countries, but there are fewer reports on oral lesions from developing countries [6]. Oral lesion is an integral part of overall health and it is strongly associated with systemic conditions [7]. The prevalence of oral lesion is higher among HIV-positive people (HIV+) than among the general population [8].
The oral cavity is the mirror of the overall health of an individual. Among HIV‑associated infections, oral lesion manifestations have been documented as one of the most prevalent morbidities since the beginning of the epidemic. Oral lesions are the earliest clinical manifestations among people living with human immunodeficiency virus (PLHIV) predicting the progression of HIV to AIDS [9]. Oral lesions can not only indicate infection with human immunodeficiency virus (HIV), but they are also among the early clinical features of the infection and can predict progression of HIV disease to acquired immune deficiency syndrome (AIDS). Seven types of oral lesions manifestation are strongly associated with HIV infection and also most commonly found globally, i.e., oral candidiasis, hairy leukoplakia, “acute necrotizing ulcerative gingivitis” (ANUG), “acute necrotizing ulcerative periodontitis” (ANUP), Kaposi sarcoma, linear gingival erythema, and nonHodgkin lymphoma [10]. These oral lesions may be present in up to 50% of the PLHIV and up to 80% of those with a diagnosis of AIDS. The severity of lesions depends on a low CD4+ cell count [11].
The oral lesions of HIV infection can be categorized into infections, neoplasms, immune mediated, other diseases (parotid disease, nutritional, xerostomia), and oral manifestations as adverse effects of anti-retroviral therapy. Oral or pharyngeal candidiasis are the commonest fungal infections observed as the initial manifestation of symptomatic HIV infection. Oral hairy leukoplakia has been shown to be associated with Epstein–Barr virus (EBV) infection. Oral candidiasis and oral hairy leukoplakia are associated very frequently and are considered AIDS defining disease and have also been included in the clinical classification of HIV by Centers for Disease Control and Prevention CDC [12].
Other infectious diseases commonly occurring in HIV patients are herpes simplex and varicella zoster virus infection, Cytomegalovirus-related ulcerations, oral warts associated with human papilloma virus, linear erythematous gingivitis, necrotizing ulcerative gingivitis, necrotizing ulcerative periodontitis, and syphilis. Kaposi’s sarcoma and non-Hodgkin’s lymphoma are the most common neoplasms occur in HIV patients. The disorders of the immune system also led to various oral manifestations, such as aphthous ulcers, xerostomia and necrotizing stomatitis [12, 13].
Oral manifestations such as adverse effect of anti- retroviral therapy can also be found they are oral hyperpigmentation, erythema multiform, xerostomia, paresthesia, lip edema, cheilitis, and taste disturbances [13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32]. Significance of the Study The study contributes on the usefulness of oral cavity lesions finding as markers of disease progression and screening those populations at risk. It will u t i l i z e to make recommendation to the responsible body for the advancement of better care for HIV positive patient with oral lesions. It is believed that the result of this study will be used as a base line data and information for further study or intervention.
Objectives
General Objectives
To assess prevalence of oral lesion and its associated risk factor in HIV positive patient in order to reduce the possible risk factors with a collaboration of dentist with another department.
Specific Objectives
a) To assess the prevalence of oral lesion in HIV/AIDS patient’s b) To investigate the outcome of ART on oral lesions c) To determine the association of oral lesions with level of CD4 cell count d) To determine the most common oral lesions, present in HIV/AIDS patients e) To assess the association of oral lesion and oral hygiene practice in HIV positive person. f) To assess the association of oral lesion and habits in HIV +ve patient.
Methodology
Study Area
Study was conducted in JUMC ART clinic, Oromia Region, South West Ethiopia, Jima. JUMC is one of the oldest public hospitals in the country, it was established in 1930 EC by Italian invaders for the service of their soldiers, it is located in Jimma city which is 352 Km from Addis Ababa, currently it became the only teaching and referral hospital in south western part of the country. JUMC provides services for approximately 20millin peoples with 1600 staff members and 800 beds, The ART clinic was established in 1999 EC.
Study Period
Study was conducted from June 15 to July15/ 2023 in JUMC, ART clinic.
Study Design
A cross sectional study was conducted on prevalence and associated factors of oral lesions among HIV/AIDS patients attending Jimma university medical center, ART Clinic.
Population
Source population: All HIV/AIDS patient’s attending in JUMC, ART clinic. Study population: All HIV/AIDS patients attending in Jimma University medical center, ART clinic during data collection period were target population for this study.
Inclusive Criteria
All HIV/AIDS patients who came to JUMC, ART clinic during data collection time and all volunteer patients included in the study.
Exclusion Criteria
In volunteer patients and acute sick looking patients those unable to respond for questionnaire were not included.
Sample Size and Sampling Technique
Sample size determination: The total sample size planned to select for the study was 97. All samples were drawn from HIV patients attended in Jimma University medical center (JUMC) ART clinic, it is determined by using Yemane taro formula of sample size determination, it is computed as:
N n = 1+N(e2)
N is total population e- is the level of maximum error required (the level of precision) For this study the researcher used precision level 10%. From this the sample size of the study that was used is computed as:
N n = 1+N(e2) 3209 1 3209(0.1)2 96.98 97
n $$ \begin{array}{l} i = \frac {3 2 0}{1 + 3 2 0 9} \\ i = 9 6. 9 8 \approx 9 \\ \end{array} $$ n Sampling techniques: Convenience type of sampling method was used that all HIV infected patients with new incidence and follow up in Jimma University Medical Center, ART Clinic, and 96 patients used as sample size in the study.
Study Variables
Independent variables: Socio demographic status (Age, sex, marital status, occupational status, educational level, religion, CD4cell count, oral hygiene Practice, Patients’ habits (smoking, drinking alcohol, chat chewing). Dependent variables Oral lesions • Fungal infection: Erythematous candidiasis, pseudo membranous candidiasis, Hyperplastic candidiasis, Angular cheilitis. • Viral infection: Oral hairy leukoplakia, Herpes simplex virus (HSV) Human papilloma virus, Herpes zoserter virus. • Bacterial infection: Necrotizing ulcerative gingivitis, necrotizing ulcerative periodontitis, necrotizing ulcerative stomatitis. • Neoplasm: Kaposis sarcoma, non-Hodgkin lymphoma • Nonspecific etiology: Xerostomia, salivary gland diseases, aphthous ulcer, pain syndrome
Data Collection Technique and Materials
Data collection materials: The materials that were used; computer questionnaire stationary materials like; paper, pens, pencils, ruler, eraser, sharper, etc. and materials used for intra oral examination like gauze, spatula, glove and flash light.
Data Collection technique: The examination was done when patient was seat on the chair under flash light and natural light, the extra oral examination and intra oral examination was done by a dental interns according to their clinical presentation without knowing the HIV clinical stage and CD4 cell count level of the patient or whether the patient was on HAART or not, then further medical information was obtained by reviewing the patient medical record and filling self-administered questionnaire because to reduce the bias activity during examining the patient to get correct diagnosis.
Data Quality Control
For obtaining adequate information, first questionnaires were prepared and then the advisor evaluated them and data was collected.
Data Analysis and Interpretation
Before analyzing data, the information was arranged according to their contents and purpose of study and data was summarized for cleanness, checked for completeness and analyzed by computer statistical program, SPSS using window 16 version and the result was presented by using, tables, figures and statements. Ethical Consideration A formal letter was written by Jimma University, medical center, school of dentistry to concerned bodies particularly to leaders to have permission and support while data collection and appropriate subjects was informed about the objectives, purposes and benefits of the study and the consent of the patient was asked and informed verbally before any procedure under taken .
Dissemination of Result
The result of the study was disseminated to student research program office and Jimma university school of dentistry.
Operational Definition
- Oral lesions: Lesions which are presents in oral cavity due to fungal, bacteria, viral, neoplastic condition and others.
- Fungal infection: A localized fungal infection is the most common opportunistic oral manifestation found in patients with HIV disease caused pain, burning sensation and difficulty in chewing in patient.
- Oral candidiasis: Is fungal infection most commonly associated with HIV/AIDS, caused by Candida barbican, it broadly known as oral thrush, it is a relatively frequent problem for people who are HIV Positive, people with candidiasis often notice changes in the oral cavity taste perception, which may make food undesirable.
- Pseudomembranous candidiasis is type of oral candidiasis with clinical presentation of creamy white adherent plaques, resembling cheese or curdled milk, located anywhere in the mouth.
- Erythematosus candidiasis: Erythematosus (atrophic) macular patches on mucosal surfaces, areas such as dorsum of tongue, which normally have Papillae, are often depopulated, palatial mucosa is usually affected, color ranges from light pink to scarlet.
- Hyperplastic candidiasis is oral candidiasis with clinical features: White plaques that are not removable by scraping, it is usually seen in middle-aged commonly in anterior buccal mucosa.
- Angular cheilitis: Fissures or linear ulcers at corner of mouth, varying degrees of inflammatory erythema; hyperkeratosis may be present peripheral to the fissure.
- Bacterial infections: Bacteria are the causative agent in a substantial proportion of infections in oral mucosa can originate anywhere in the oral cavity and are usually the first sign of the condition. In the initial phase, some diseases could present symptomless, making the diagnosis challenging.
- Necrotizing ulcerative gingivitis; is ulcerative or necrotic destruction of the gingival tissues, often with blunting or catering of the interdental Padilla.
- Necrotizing ulcerative periodontitis: Advanced necrotic destruction of the periodontium with rapid loss of periodontal attachment and alveolar bone.
- Viral infection: Viral infections of the oral cavity usually manifest as either ulceration or blistering presentation of oral tissues and may either occur due to cellular destruction or consequence of immune reaction following viral proteins.
- AIDS: A condition in human in which progressive failure of the immune system allows life- threatening opportunistic infection and cancer to thrive.
- HIV: Human immunodeficiency virus- is a lent virus (a member of the retrovirus family) HIV infects vital cells in the human immune system such as T cells (specifically CD+ T cells), macrophages, and dendritic cells.
- Herpes simplex virus: Is a virus which causes both primary and secondary or recurrent disease in the oral cavity. It is characterized by the eruption of serum filled vesicle, or blisters (sometimes referred to as’ ’cold sore’’ or’’ fever blister’’) on the face, lips, or mouth.
- Herpes zoster virus: Disease occur in the elderly and immune compromised individuals with clinical features of pain, multiple vesicles on the facial skin, lips and oral mucosa.
- Human papilloma virus: Lesions caused by HPV are common on the skin and mucus membranes of persons with HIV disease. Lesions in the oral cavity may appear as solitary or multiple modules.
- Non-Hodgkin’s lymphoma: Lymphoma can occur anywhere in the oral cavity and there may be soft tissue involvement with or without involvement of the underlying bone.
- Oral Hairy Leukoplakia: A non-scrap able corrugated or ‘’hairy’’ white lesion on the lateral margins of the tongue, occurs in all risk groups for HIV infection, although less commonly in children than in adults.
- Periodontal diseases: A fairly common problem in both asymptomatic and symptomatic HIV – infected patients with clinical presentation of redness of the gingiva, ulceration of interdental papillae, spontaneous bleeding, edematous gum bone destruction, gingival recession halitosis and pain.
- Salivary gland disease and Xerostomia: Salivary gland disease is abnormal condition /disease/ which affect saliva producing exocrine glands which is known by causing xerostomia or dryness of mouth due to decrease in production of saliva.
Result
In this study, out of the 96 HIV/AIDS patients examined, 43 (44.8%) were males and 53 (55.2%) were females. Most of them (33 (34.4%)) were in the age group of 20-29 followed by age group of 30-39 which is 23 (24%). Regarding marital status, most of them were Divorced (32.3%), followed by single (30.2%). According to Religion most of them were Muslim 35 (36.5%) followed by Orthodox 33 (34.4%) and the least were wakefata 3 (3.1%). Regarding occupation 34 (35.4%) of them were Private worker followed by merchant 23 (24%) and the least were NGO employer 2(2.1%). Regarding the educational levels 23 (24%) were attended elementary school, followed by 22 (23%) high school while 15.6% were can read and write only. The demographics characteristics of patients are summarized in Table 1.
| Frequency | Percentage % | |||
|---|---|---|---|---|
| Age | < 20 | 5 | 5.2 | |
| Age | 20-29 | 33 | 34.4 | |
| Age | 30-39 | 23 | 24 | |
| Age | 40-49 | 20 | 20.8 | |
| Age | 50-59 | 9 | 9.4 | |
| Age | >60 | 6 | 6.3 | |
| Sex | Male | 43 | 44.8 | |
| Sex | Female | 53 | 55.2 | |
| Religion | Muslim | 35 | 36.5 | |
| Religion | Orthodox | 33 | 34.4 | |
| Religion | Others | 5 | 5.2 | |
| Religion | Protestant | 20 | 20.8 | |
| Religion | Wakefata | 3 | 3.1 | |
| Marital status | Divorced | 31 | 32.3 | |
| Marital status | Engaged | 2 | 2.1 | |
| Marital status | Married | 25 | 26 | |
| Characteristics | Frequency | Percentage % | ||
| Occupation | Single | 29 | 30.2 | |
| Occupation | Widowed | 9 | 9.4 | |
| Occupation | Farmer | 5 | 5.2 | |
| Occupation | Government worker | 6 | 6.3 | |
| Occupation | House wife | 17 | 17.7 | |
| Occupation | Merchant | 23 | 24 | |
| Occupation | NGO employer | 2 | 2.1 | |
| Occupation | Others | 9 | 9.4 | |
| Occupation | Private worker | 34 | 35.4 | |
| Occupation | Level of education | Degree | 10 | 10.4 |
| Diploma | Level of education | 7 | 7.3 | |
| Elementary | Level of education | 23 | 24 | |
| Not educated | Level of education | 19 | 19.80% | |
| read and write only | Level of education | 15 | 15.60% | |
| secondary school | Level of education | 22 | 23.90% | |
| Total | 96 | 100% |
Table 1: Socio-demographics characteristics of patients (n =96).
From a total of 96 studied population, 45(46.9.%) has HIV/AIDS associated oral lesions, according to the oral lesions identified in this study, fungal lesions constituted the highest and the pseudo membranous candidiasis was the most common type 11(11.5%), followed by Erythematous candidiasis and Hyperplastic candidiasis 2(2.1%), and the least was Angular cheilitis 1(1%) The second most common oral lesion was viral lesions from that Oral hairy leukoplakia
8(8.3%), accounts highest followed Herpes simplex virus 2(2.1%), and Human papilloma virus (2.1%). The third most common oral lesions were bacterial lesions accounts 6(6.2%) Necrotizing ulcerative periodontitis and necrotizing ulcerative gingivitis 5 (5.2%). The fourth most common oral lesions were neoplasm, from this Kaposis sarcoma 3 (3.1%) other nonspecific etiology were aphthous ulcers 3(3.1%) was found in this study (Table 2).
| Oral lesions variables | Frequency | Total | ||
|---|---|---|---|---|
| Male | Female | |||
| Oral candidiasis | Pseudo membranous candidiasis | 7 (7.3%) | 4 (4.2%) | 11(11.5%) |
| Erythematous candidiasis | 2(2.1%) | 0 (0.0%) | 2 (2.1%) | |
| Hyperplastic candidiasis | 2 (2.1%) | 0 (0.0%) | 2 (2.1%) | |
| Angular cheilitis | 1(1%) | 0 (0.0%) | 1(1%) | |
| Viral infection | Oral hairy leukoplakia | 2 (2.1%) | 6 (6.2%) | 8 (8.3%) |
| Herpes simplex virus | 1 (1.0%) | 1 (1.0%) | 2 (2.1%) | |
| Human papilloma virus | 1 (1.0%) | 1(1.0%) | 2 (2.1%) | |
| Bacterial infection | Necrotizing ulcerative periodontitis | 1(1%) | 5(5.2%) | 6(6.2% ) |
| Necrotizing ulcerative gingivitis | 1(1%) | 4 (4.2%) | 5 (5.2%) | |
| Non-specific etiology | Aphthous ulcers | 1(1.0% | 2(2.1% ) | 3(3.1% ) |
| Neoplasm | Non- Hodgkin lymphoma | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Kaposis sarcoma | 2 (2.1%) | 1(1.0%) | 3 (3.1%) | |
| Total | 21(21.9%) | 24(25%) | 45(46.9%) |
Table 2: Frequency distribution and association between chat chewer and oral lesions among HIV/AIDS patients (n = 96).
- Regarding to smoking cigarette habits, oral lesions were more observed in cigarette smokers 27 (60%) as compared with non-smokers 18 (40%). Chi -square result indicates that there is statistically significant association between smoking
- Cigarette and oral lesions at 1% (P=0.00) significance level
- (Table 3).
- Association of oral lesions with chewing chat in HIV/
- ADIS patients were observed high in chat chewer 31
- (65.96%) than in non-chewer 14(28.57%). The chi-square result shows that there is statistically significant association between chat chewing and oral lesions at 1% (P=0.00)
- Significance level (Table 4).
- No oral lesion
- Has oral lesions
- Total χ2-test
- P Value
- Chat chewing
- No
- 35 (71.43%)
- 14(28.57%)
- 49 (100%)
- 13.4648
- 0
- Yes
- 16 (34.04)
- 31(65.96%)
- 47(100%)
- Total
- 51(53.13)
- 45(46.88)
- 96(100%)
Table 3: Frequency distribution and association between chat chewer and oral lesions among HIV/AIDS patients (n = 96).
| No Oral lesions | Has oral lesions | Total | χ2-test | P-value | |
|---|---|---|---|---|---|
| No | 44 (86.27%) | 18 (40%) | 62 (64.58%) | 22.3804 | 0 |
| Yes | 7 (13.73%) | 27 (60%) | 34 (35.42) | 22.3804 | 0 |
| Total | 51 (100) | 45 (100%) | 96 (100%) | 22.3804 | 0 |
Table 4: Frequency distribution and association between chat chewer and oral lesions among HIV/AIDS patients (n = 96).
- The association of oral lesions were observed to be high in HIV/AIDS patients, using alcohol drink 36 (80%) than in non-alcohol users 9 (20%). The chi – square result indicates that there is statistically significant association between alcohol drinking and oral lesions at 1% (P =0.002) significance level (Table 5).
- Table 5: Frequency distribution and association between alcohol drinking and oral lesion among HIV/AIDS patient (n = 96).
- Oral lesions were highly observed in HIV/AIDS patients with CD4 cell count<200 cells/µL 28 (62.22%), followed by
- 200-499 cells /µL 14(31.11%) and >500 cells /µL 3 (6.67%
- ) from total patents with oral lesions, the chi-square result shows that there is significant association between CD4cell count and oral lesions at 1% (P=0.003 ) significance level,
- (Table 6 ).
- CD4 cell count
- No oral lesion
- Has oral lesion
- Total χ2 test
- P-value
- <200 cells /µL
- 14(27.45%)
- 28(62.22%)
- 42(43.75)
- 11.7558
- 0.003
- 200-499 cells /µ
- 30(58.82%)
- 14(31.11)
- 44(45.83)
- >500 cells /µL
- 7(13.73%)
- 3(6.67%)
- 10(10.42%)
- Total
- 51(100%)
- 45(100%)
- 96(100%)
Table 5: Frequency distribution and association between CD4 cell count and oral lesion among HIV/AIDS patients (n = 96).
| No oral lesion | Has oral lesion | Total | χ2 test | P-value | |
|---|---|---|---|---|---|
| No | 26(50.98%) | 9(20%) | 35(36.46%) | 9.9044 | 0 |
| Yes | 25(49.02) | 36(80%) | 61(63.54%) | 9.9044 | 0 |
| Total | 51(100%) | 45(100%) | 96(100%) | 9.9044 | 0 |
Table 6: Frequency distribution and association between ART and oral lesion among HIV/AIDS patient (n = 96).
- Prevalence of oral lesions were highly observed in HIV/
- AIDS patients with HAART in27 (60%) while without HAART
- 18 (40%) Test statistics chi-square result shows that there is statistically significant association between ART and oral lesions at 1 % (P=0.007) significance level, (Table 7).
- ART
- No oral lesion
- With oral lesion
- Total χ2 test
- P-value
- With HAART
- 43(84.31%)
- 27(60%)
- 70(72.92%)
- 7.1563
- 0.007
- Without HAART
- 8(15.69%)
- 18(40%)
- 26(27.08)
- Total
- 51(100%)
- 45(100%)
- 96(100)
Table 7: Frequency distribution and association between ART and oral lesion among HIV/AIDS patient (n = 96).
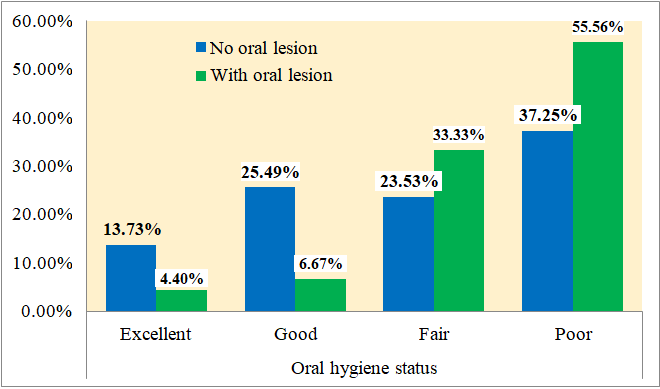
Regarding to frequency distribution and Association of oral lesions with oral hygiene status, most of the Patients with poor oral hygiene status has oral lesions 25 (55.60%), followed by fair oral hygiene status 15 (33.3%), Good oral hygiene status 3 (6.67%) and excellent oral hygiene status 2(4.4%). The result of Chi-square showed that there is statistically significant association between oral hygiene status and oral lesion at 5% (p=0.020) significance level (Figure 1).
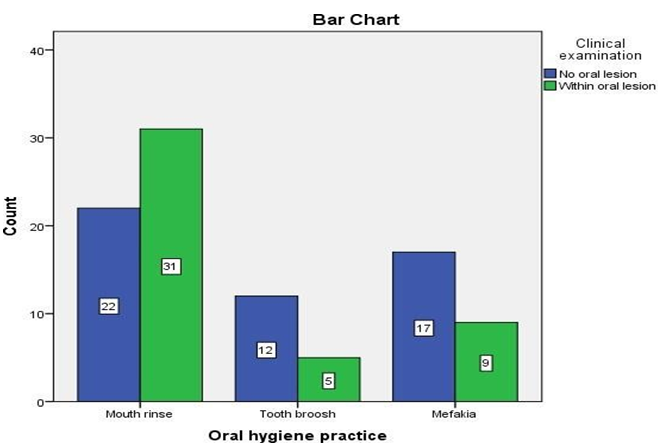
Regarding to frequency distribution and association of oral lesions with oral hygiene practice in HIV/AIDS patients, most of patients using mouth rinse technique 31 (32.3%) has oral lesions followed by those using Mefakia 9 (9.4% ) and, tooth brush 5 (5.2% ) with high statistically significant association p-value (0.02) (Figure 2).
Discussion
This study describes the prevalence and associated factors of oral lesions in HIV/AIDS patients attending in Jimma university medical center at ART Clinic, Jimma, Oromia, South-western Ethiopia. The overall prevalence of oral lesions in this study was found to be in 45(46.9%), Which was highly in agreement with the research findings that were conducted in Arero Health Center at ART clinic, Arero town, Borena Zone, Oromia Regional State, South Ethiopia with prevalence of 48.8%. Prevalence of oral lesion in the other studies show that their occurrence was approximately 35.7% to 73.1 % The high prevalence could be because the HIV patients visited the health institution at later stages of the infection when the appearance of oral lesions is common [33].
The distribution of the studied population by gender demonstrated that 43(44.8%) of the individuals HIV/ AIDS corresponding to male and 53(55.2%) females, with Male to female ratio in this study is 1:1.5 which is roughly representative of the HIV disease burden in Ethiopia. The great prevalence in female suggests that due to being reinforced further by the fact that older men date or marry younger women. The most affected age group was young and active age groups,2029 2nd decades 33 (34.4%) and majority are within the 3rd decades of life 30-39(24%) and 4th decades of life40-49(20.8%) as confirmed by these findings of study. This marked prevalence of HIV/AIDS infection in 2nd decade’s age group may be due to early starting of sexual contact and having more than one partners.
The most common HIV/AIDS associated oral lesion in this study was pseudomembranous candidiasis 11(11.5%) followed by Oral hairy leukoplakia 8(8.3%) necrotizing ulcerative periodontitis 6(6.2%). Candida is commensal, but in immune compromised conditions, it can become pathogenic. Oral candidiasis (pseudomembranous 11(11.5%), erythematous and Hyperplastic candidiasis 2(2.1%) and angular cheilitis 1(1%) were found. Prevalence of Candidiasis was the most common oral manifestation as these studies. Other studies show similar result, the occurrence of pseudomembranous candidiasis was found to be 23% in Nigeria [33] and 20.1% in Ethiopia [31] erythematous candidiasis 10% % and angular cheilitis 7.5% % in Ethiopia [32].
Viral infection was second common oral lesion Oral hairy leukoplakia 8(8.3%), Herpes simplex virus 2(2.1%) were seen in this study. Also, prevalence bacterial lesions accounts
6(6.2%) necrotizing ulcerative periodontitis, necrotizing ulcerative gingivitis 5(5.2%), Other oral lesions like, neoplasm were Kaposis sarcoma 3 (3.1%) and nonspecific etiology were aphthous ulcers 3(3.1%) was found in this study although; the results of this investigation are disagreed with other previous investigations.
According to this study associated factors with the occurrence of oral lesions was highly observed in patients with alcohol drinking around 36(80%) followed by smoking and patient with chat chewer in 31(65.96%) was oral lesion was seen in patient with not use any substance, with statistically significant association at 1% significant level. Oral lesion was highly observed in CD4 count category <200 cells /µL (62.22%) which is followed by 200-499 cell/NL (31.11%) and only (6.67%) of lesions is in patient with > 500 cell/NL each category, was statistically significant association with oral lesions. Prevalence of oral lesion was highly observed in patients with HAART in 27(60%) while without HAART 18(40%) were observed, with statistically significant association with oral lesions. Moreover, the smaller sample size and most of the patients admitted in Jimma university medical center ART clinic were CD4 cell count <200 cells /µL (62.22%) with highest participant due to this reason study might have missed to pick up any significant association of prevalence of oral lesion with the CD4 count and HAART patients.
Among 45(46.9%) oral lesion prevalence, most of the patients uses month rinse technique 31 (32.3%) followed by mefakia 9(9.4%) and tooth brush 5(5.2%) has high statistically significant association with oral lesions, In associations of oral lesions with oral hygiene practice most of the patients with poor oral hygiene status has oral lesions 25 (55.60%), followed by fair oral hygiene status 15 (33.3%), Good oral hygiene status 3 (6.7 % ) excellent oral hygiene status 2 (4.4% ) These variables have significant association with oral hygiene practice ,The significant factors associated with the occurrence of oral lesions in our study were higher tobacco use and alcohol consumption and poor oral hygienic practices and maximum participants were from lower socioeconomic class. Higher tobacco uses and poor oral hygienic practices were also found among the HIV/AIDS patients of another study conducted in India [34]. Limitations There was shortage of time to get more patients, and low flow of patient during data collection time, and also most of patients were involuntary for interview and oral examination. There was no laboratory examination (testing) material to differentiate one lesion from the other that may be wrongly diagnosed by clinical feature only.
Conclusion and Recommendation
This study reveals that nearly half participants of the HIV/AIDS patients’ suffered from oral lesions. The most prevalent oral lesions among HIV/AIDS patients were pseudomembranous candidiasis 11(11.5%) followed by Oral hairy leukoplakia 8(8.3%) and necrotizing ulcerative periodontitis 6(6.2%). The significant factors associated with the occurrence of oral lesions in this study were higher in chat chewer, alcohol consumer, Smoking cigarettes and patients those use mouth rinse technique oral hygienic practices and has poor oral hygienic status. This may be because of the intensification of infectious lesions and the possibility of secondary infection in poor oral hygiene
Recommendation
I recommend and emphasize on the usefulness of oral examination in every HIV infected individual in clinical evaluation and management. Based on the finding in this study the following recommendations were drawn to concerned bodies.
- The Hospital administration and NGO that work on HIV/ AIDS should give special attention for such patients
- Oral health educational should be given for patients to prevent oral lesions that associated with poor oral hygiene
- It’s better to establish one center for follow up of such patients by dental doctors to solve the problem.
- Patients should be trained about the proper techniques of brushing and they should also be counseled for two times brushing because oral hygiene is necessary for having a healthy mouth and also contribute to their quality of life.
- Patients should regularly follow up of HAART and control their CD4 cell level.
Acknowledgment
First of all I would like to thank God for helping me in every aspect of my life, then I would like to give my heart full thank to my advisors Dr. Kefen Yirda (OMFS surgeon) & Dr. Fetene Humne (DMD) for your constructive comments, and also, I would like to forward my special thanks to my family and peoples beside me that give me unforgettable support to reach at this stage. Finally, I want to thank Jimma University for internet access, ART Staff members and my friends for you encourage and professional support on this research.
References
-
WHO (2020) Global HIV Epidemic.
-
WHO (2021) The Global Health Observatory.
-
FMOH (2015) HIV Epidemic Estimates by Regional States and Ethiopia. Federal Ministry of Health, HIV/ AIDS Prevention and Control Office.
-
Anita D, Sunil S, Ravindra R, Anuja A, Ruchira V, et al. (2022) Prevalence of Oral Lesions among HIV Positive Patients Attending Antiretroviral Therapy Centre in Rural Area of Western Maharashtra. Journal of Clinical and Diagnostic Research 16(4): 07-12.
-
HK Holmes, LXG Stephen (2002) Oral lesions of HIV infection in developing countries. Oral Dis 8 Suppl 2: 40- 43.
-
Narani N, Epstein JB (2001) Classification of oral lesions in HIV infection. J Clin Periodontology 28(2): 137-145.
-
Morenike O, Folayan O, Boladale M, Nneka M, Michael A, et al. (2021) Associations between mental health problems and risky oral and sexual behaviour in adolescents in a sub- urban community in Southwest Nigeria. BMC Oral Health 21(1): 401.
-
Brondani MA, Phillips JC, Kerston RP, Moniri NR (2016) Stigma around HIV in Dental Care: Patients’ Experiences. J Can Dent Assoc 82: 1.
-
Coogan MM, Greenspan J, Challacombe SJ (2005) Oral lesions in infection with human immunodefciency virus. Bull World Health Organ 83(9): 700‑706.
-
Prabhu RV, Chatra L, Shenai P, Prabhu V (2013) Bilateral fusion in primary mandibular teeth. Indian J Dent Res 24: 277.
-
Palmer GD, Robinson PG, Challacombe SJ, Birnbaum W, Croser D, et al. (1996) Aetiological factors for oral manifestations of HIV. Oral Dis 2(3): 193‑197.
-
Aškinytė D, Matulionytė R, Rimkevičius A (2015) Oral manifestations of HIV disease: a review. Stomatologija 17(1): 21-28.
-
Bajpai S, Pazare AR (2010) Oral manifestations of HIV disease. Contemp Clin Dent 1(1): 1-5.
-
Peterson PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C (2005) The global burden of oral disease and risks to oral health. Bulletin World Health Org 83(9): 661-669.
-
Petersen PE (2006) Policy for prevention of oral manifestations in HIV//AIDs; the approach of the WHO global oral health program. Adv Dent Res 19(1): 17-20.
-
Bravo IM, Correnti M, Escalona L, Perrone M, Brito A, et al. (2006) Prevalence of oral lesions in HIV patients related to CD4 cell count and viral load in a Tanzania population. Int J Dent Med Oral Patol Oral Cir Bucal 11(1): 33-39.
-
Arendorf T, BredeKamp B, Cloete C, Wood R, Keefe EO (1997) Intergroup comparisons of oral lesions in HIV positive South Africans. Oral Dis 1: 54-57.
-
Sufawati I, Raf MA, Putri FM (2021) Evaluating knowledge, attitude, and behavior of dentists on HIV/ AIDS in West Java, Indonesia, in the COVID-19era. Int J Dent 2021: 1901887.
-
Arotiba T, Adebola Z, Iliyasu M, Babashan M (2005) Oral manifestations of HIV/Aids infection in Nigerian patients 7: 176-181.
-
Solsilverman’s L.roveversole (2001) Edmond True love Essentials of oral medicine. pp: 128-142.
-
Mascarenhas AK, Smith SR (1999) Factors associated with utilization of core for oral lesion in HIV disease. Oral Med, Oral Pathol Oral Radiol Endod 87(6): 708-713.
-
(1993) Oral manifestation of HIV disease; international AIDs society of USA.
-
Lomelí-Martínez SM, González-Hernández LA, Ruiz- Anaya AD, Lomeli Martinez M, Martinez Salazar SY, et al. (2022) Oral manifestations associated with HIV/AIDS patients. Medicine 58(9): 1214.
-
Tappuni AR, Sufawati I (2020) The Bali declaration on oral health in HIV/AIDS. Oral Dis 26(1): 172.
-
Pinheiro A, Marcenes W, Zakrzewska JM, Robinson PG (2004) Dental and oral lesions in HIV infected patients: a study in Brazil. Int Dent J 54(3): 131-137.
-
Khatibi M, Moshari AA, Jahromi ZM, Ramezankhani A (2011) Prevalence of oral mucosal lesions and related factors in 200 HIV+ ⁄ AIDS Iranian patients. J Oral Pathol Med 40(8): 659-664.
-
Jana PK, Sahu SK, Sivaranjini K, Hamide A, Roy G (2022) Prevalence of oral lesions and its associated risk factors among PLHIV availing anti‑retroviral therapy from a selected tertiary care hospital, Puducherry- A Cross Sectional Analytical Study. Indian J Community Med 47(2): 235‑239.
-
Ceena E, John R, Ravikiran O, Almas B, Srikant N, et al. (2016) Oral Lesions in HIV/AIDS Patients on a highly Active Antiretroviral Therapy. World Journal of Dentistry 7(2): 95-99.
-
Bagus S, Parmadiati AE, Hendarti HT, Radithia D, Ernawati DS (2019) The Prevalence of Oral Manifestation in Transgenders with HIV/AIDS in Surabaya, East Java, Indonesia. Indian Journal of Public Health Research & Development 10(1): 577-580.
-
Arotiba RA, Adebola Z, Shokunbi M, Osude OD (2005) Oral manifestations of Hiv/Aids infection in Nigerian patients seen in Kano. Nigerian Journal of Surgical Research 7: 1-2,176-181.
-
Gutter S, Feleke Y, Fekade D, Neway M, Diro E (2008) Prevalence of oral and perioral manifestations in HIV adults at TikurAnbessa teaching Hospital: Department of Internal medicine, AAV, Ethiopia. Ethiop Med J 46(4): 349-357.
-
Gelgelo A (2013) Assessment of oral lesion and its associated factors in HIV/AIDs patients, attending Arero Health Center at ART clinic, Arero Town, Borena zone, Oromia Regional State, South Ethiopia. Jimma. Ethiop Med J.
-
Taiwo OO, Okeke EN, Jalo PH, Danfillo IS (2006) Oral manifestation of HIV/AIDs in plateau state indigene. West Afr Med 25(1): 32-37.
-
Muralidharan S, Acharya AK, Margabandhu S, Kalekhan S, Ahsan S, et al. (2018) Prevalence of periodontitis and soft tissue lesions amohuman immunodeficiency virus‑positive patients on antiretroviral therapy in Raichur Taluk, Karnataka, India. J Contemp Dent Pract; 19(1): 42‑46.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells