The Great Extraction Debate, The Origin of Functional Jaw Orthopaedics and Implications for Airway
The extraction of teeth as part of orthodontic treatment has always been contentious and indeed emotional. It has varied over time between 0.2% Angle 1902 to 80% Tweed 1966 back to 1.5% Greenfield 2010. In a narrative review the paper outlines early reports of extraction and non-extraction techniques. It also highlights the advantages and disadvantages of both methods. The origins of functional jaw orthopaedics are discussed along with prefunctional upper arch expansion as an alternative to extraction of premolars and retraction of anterior segments. The relationship of the airway to skeletal pattern and functional jaw orthopaedics is outlined. Evidence is provided to show the relationship between sleep apnoea and oropharyngeal dimension and how it relates to orthodontic treatment.
Introduction
The extraction of teeth has been a common feature of orthodontic treatment since the earliest days of the specialty. However there has been surprising little research performed into the actual numbers of teeth extracted for orthodontic purposes. Extraction frequency is defined as the number of patients having permanent teeth extracted as a percentage of the total treatment sample.
In their classic article on the subject Peck, et al. [1] reported extraction frequencies taken from 12 studies over a 66 year period, that varied between 6.5 % to 83.5 %. They also recognised that the decision to extract teeth as part of orthodontic treatment was both contentious and emotive. To quote “ For years the question of extracting permanent teeth as part of corrective orthodontics has provoked professional controversy and debate, often of religious intensity”.
Conceptual Paper
As early as 1743 Robert Bunon [2] stated that “it is better to have fewer teeth than to have the usual number in a badly arranged fashion”. Conversely Pierre Joackim Lefoulon [3] in 1841 expressed the view that “extracting is not healing but destroying”. Walter Harris Coffin [4] in 1881 concluded that “extraction of possible sound teeth may of course be necessary though these (cases) are somewhat less numerous than usually imagined and a possible alternative (expansion) in many instances affords satisfactory results”.
The question of extraction in orthodontia was the title and subject of a famous and prolonged debate in the pages of the Dental Cosmos 1912 to 1913 primarily between Calvin Case and Martin Dewey a student of Edward Hartley Angle. Case strongly criticised the non-extraction dogma of Angle as it did not take into account the effect of incisor protrusion on facial aesthetics. Case [5] concluded that “when the whole question of extraction in orthodontia is summed up and the full truth is grasped, it seems a most senseless thing for men to fight over, when the truth is so self-evident; and then to quibble and cast untruthful slurs-among men whose main object in life should be for the development of truth, true principles, and true methods of practice for the advancement of their profession, and the relief of suffering humanity!” However relapse not aesthetics was the major reason why Tweed [6] and Begg [7] abandoned the non-extraction treatment they had been taught by Angle.
A number of institutional based studies have shown that the extraction rate can vary considerably over time largely attributed to changes in clinical philosophy. Proffit [8] found the extraction rate increased from 30 % in 1953 to a peak of 76 % in 1968 before falling again to 28 % in 1993. This was largely due to a surge in four first premolar extractions being 10 % in 1953, rising to 50 % in 1968 and dropping slowly back to 10 % in 1993. Peck [9] showed that reported extraction rates changed dramatically over the past 110 years as follows: Angle 1902 0.2 %, Case 1913 6.5 %, Friel 1931 8 %, Proffit 1953 30 %, Proffit 1963 70 %, Tweed 1966 80 %, Peck 1979 42 %, Proffit 1993 28 %, Damon 2000 < 5 %, Greenfield 2010 < 1.5 %.
These studies are not directly comparable because they represent differences in clinical philosophy and case mix. However the differences are very large and vary dramatically over time. They demonstrate that there is no universally accepted philosophy when it comes to deciding to extract teeth as part of orthodontic treatment. All reported extraction rates are by their very nature retrospective and not amenable to randomised control trial methodology. Extraction of teeth as part of orthodontic treatment has always been both highly variable and highly contentious and opinion based rather than evidence based.
The present paper seeks to discover when in the literature these two alternatives were first reported for the treatment of Class II division 1 malocclusion and the indications and contraindications for each alternative form of treatment.
The Extraction versus Non-Extraction approach for the treatment of Class II division 1 malocclusion.
Historical references represent uncontrolled case descriptions and do not constitute evidence of efficiency by contemporary standards. They represent as far as can be ascertained the first appearance in the literature of the methods and concepts of the two main approaches to orthodontic treatment.
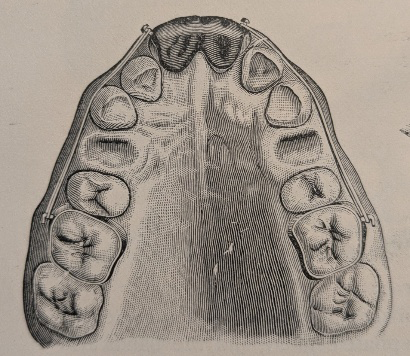
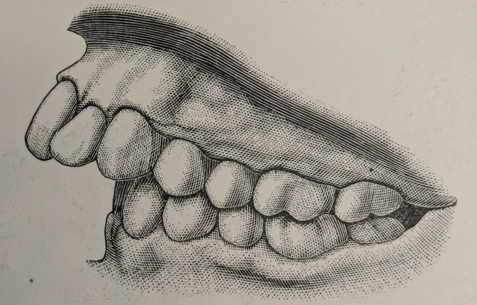
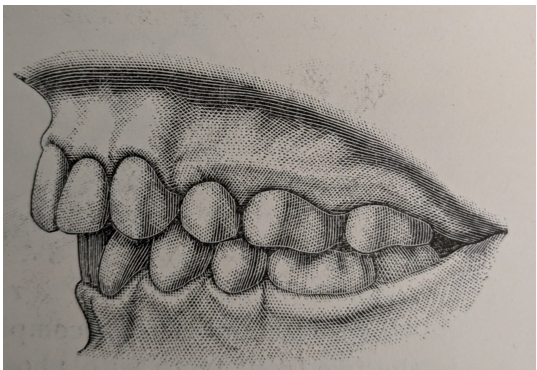
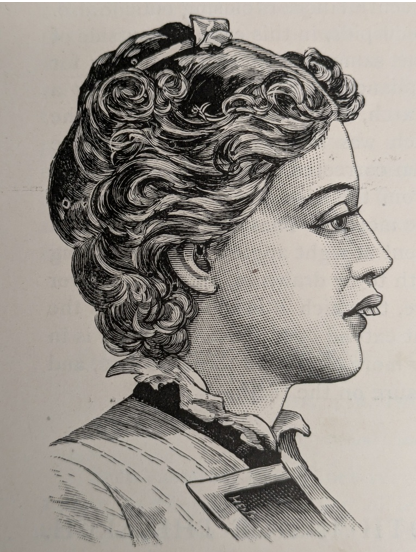
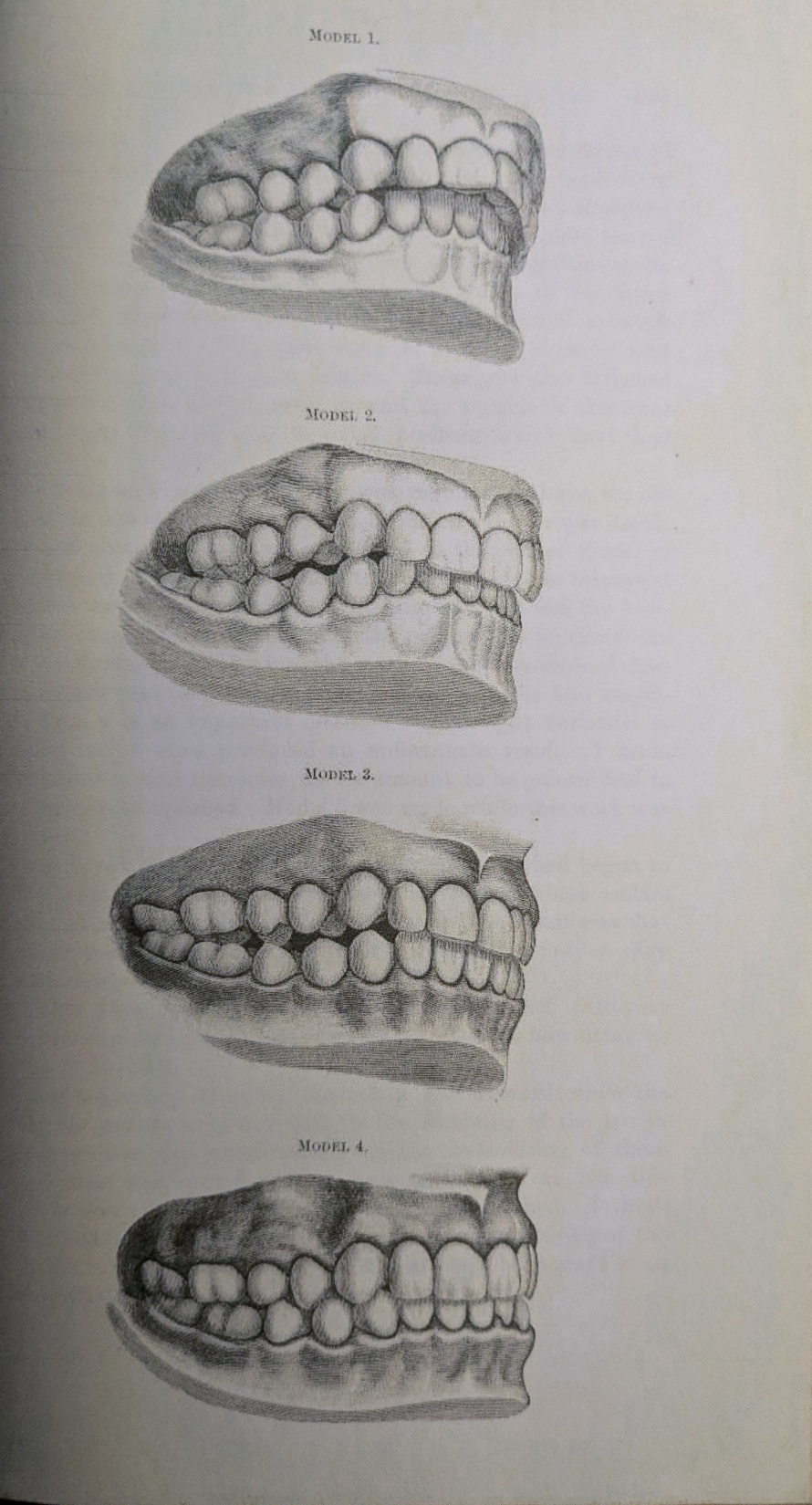
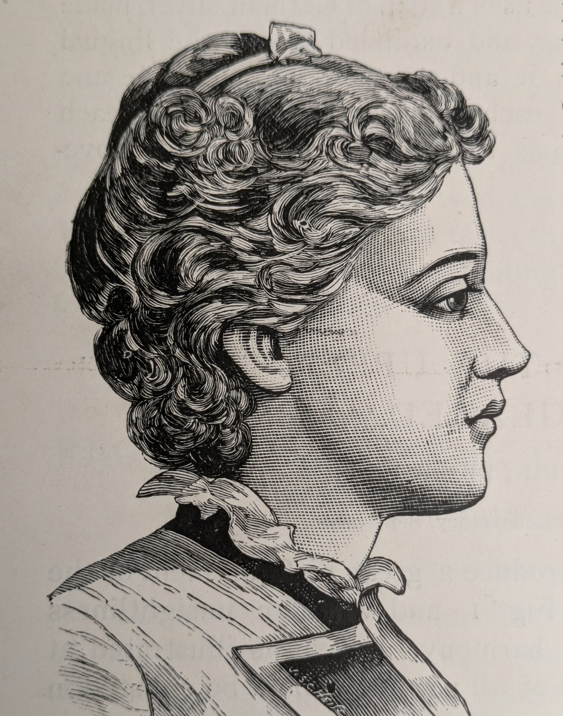
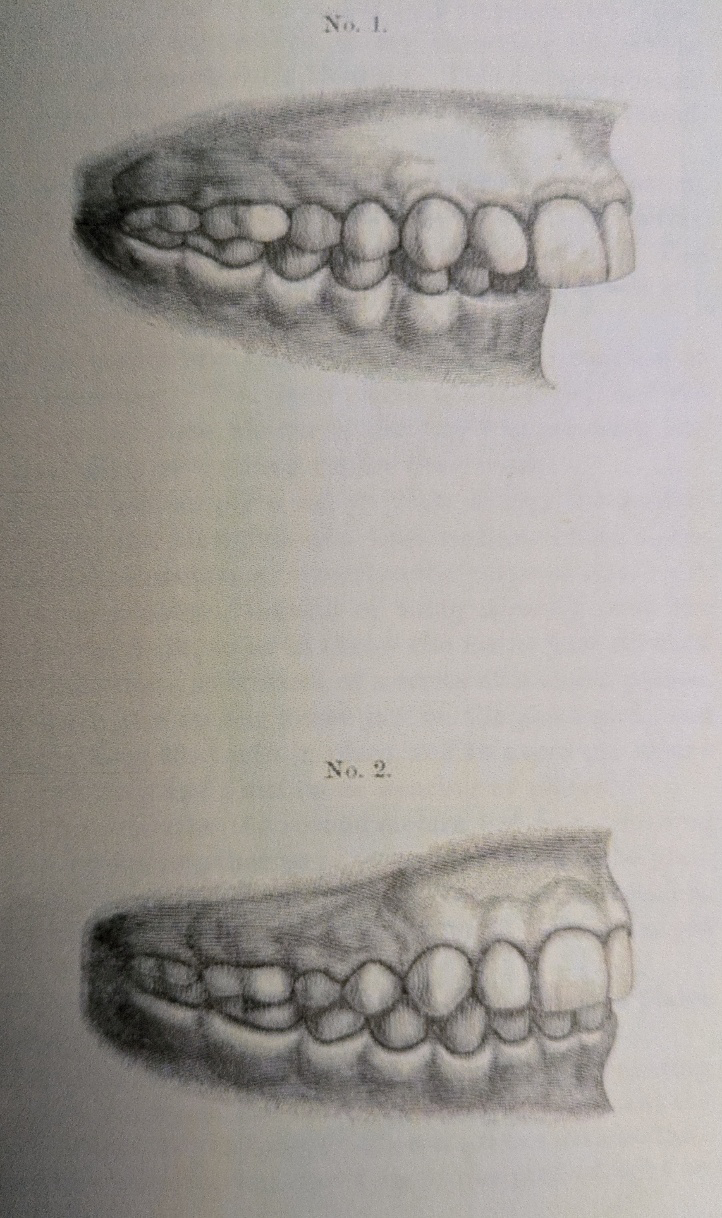
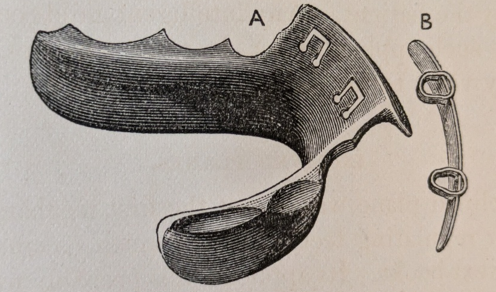
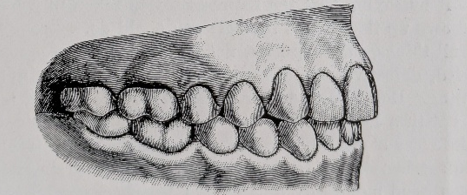
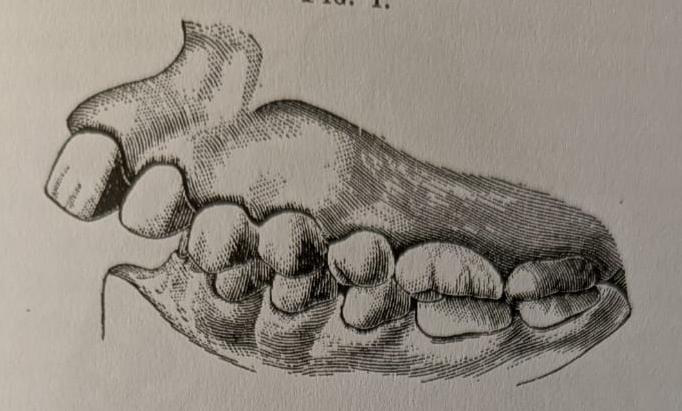
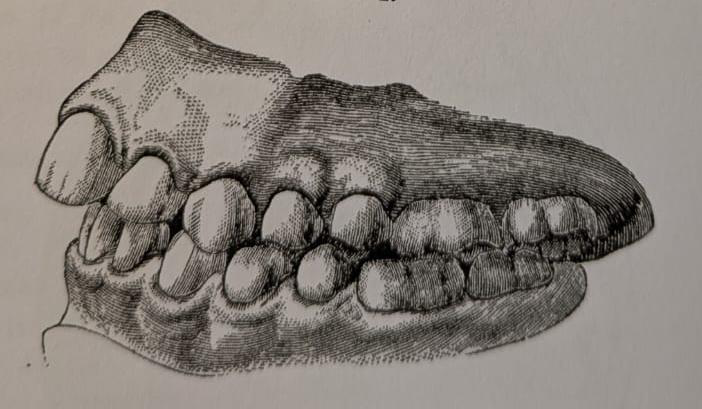
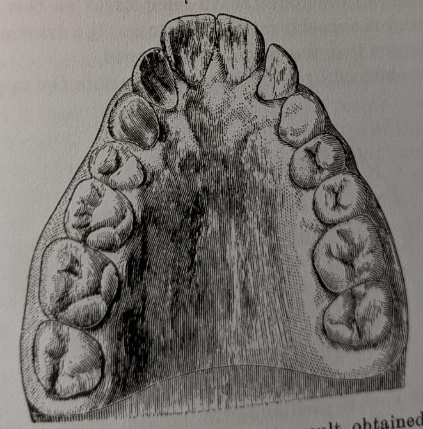
Chupein [10] was one of the earliest references to the extraction of maxillary first premolar teeth for the treatment of Class II division 1 malocclusion although the first person to propose this may well be lost in the mists of time. This landmark paper was published in Catching’s Compendium of Practical Dentistry 1894, Entitled “Protrusion of upper teeth regulated”. He used a gold cap cemented onto the upper central incisors with two small distal hooks. German silver bands with buccal hooks were cemented on the upper first molars. Elastic bands were stretched from the hooks on the central incisor cap to the molar bands on both sides after extraction of the upper first premolars (Figure 1). Etchings of before and after models (Figures 2 & 3) together with a profile views (Figures 4 & 5) of the patient show a successful result.
In the same volume of Catching’s Compendium Cutter [11] published an article entitled “Drawing the lower jaw forward”. This article had no illustrations but a similar paper was read before the American Academy of Dental Science with illustrations [12] (Figure 6). This involved upper arch midline expansion with a jack screw in a vulcanite plate. This was followed by an early design of functional appliance. One was thickened in the molar and premolar regions with depressions to carry the mandible forwards on occlusion. This was followed with an appliance thickened behind the upper incisors to maintain the forward mandibular posture.
Hamilton originally described the functional appliances used by Cutter in the American Academy of Dental Science January 1892 [13] and Catchings Compendium June 1892 [14] (Figure 7). An uncrowded Class II division 1 case without pre-functional expansion was described. “The method used was simply a rubber plate fitting the roof of the mouth and over the bicuspids and first molars where it was made thick and with depressions to receive the cusps of the lower teeth. But these depressions, instead of being directly over the cusps, were slightly in front, so as to throw the lower jaw forward when closed, by the action, as it were, of a series of inclined planes”. The upper plate was alternated with a lower one of similar design and the treatment was completed in four months. Hamilton speculated on the mechanism of action. “This advance of the lower jaw comes, I think, from preventing the condyle going to its place; but there is a change going on at the angle of the jaw which will ultimately allow a perfect articulation”. No illustration of the appliance itself was given.
Robert Duncan McBride [15] in 1904 commented that “Orthodontia is no longer in a realm of chaos. The true practice of orthodontia has little to do with dentistry proper”. More important “Orthodontia and facial art can not be separated”. He used inter-maxillary (Baker) anchorage to achieve antero posterior (Class II) correction without extractions and noted improved profiles.
Dolomore WH [16] noted in his paper on Inferior Retrusion in 1923 that “As a student I was taught to regard as superior protrusion and about which much has been written are not so at all but are cases of inferior retrusion. The treatment by retraction of the upper front teeth may have been relatively successful and the facial effect of the present abnormal occlusion is masked by the patient having an unusually flat face”.
Norman Kingsley and the Sloping Anterior Bite Plane: “Jumping the bite.” Norman William Kingsley (1829-1913) was known as “the father of orthodontia” (Figure 8). He wrote “A treatise on oral deformities as a branch of mechanical surgery”. [17] Although it was 541 pages in length only 3 ½ pages were devoted to the subject of bite planes.
First the lower inclined bite plane was described and illustrated (Figure 9). This was constructed in vulcanite and fitted in the lower arch. It impinged on any retroclined teeth in the upper arch on occlusion. As a result a force was applied to move them forwards over the bite in the traditional way described by previous workers. “The inclined plane was one of the first mechanical forces adopted for regulating teeth, and was much recommended in earlier text-books”.
Kingsley’s genius was to flip the lower inclined bite plane upside down to the upper arch and change its function. The appliance consisted of a vulcanite base plate tied in situ with molar ligatures (Figure 10). There was an anterior bite plane with a steep forward facing slope which caused the mandible to posture forwards. In addition, a gold bar was placed labially to the upper incisors. Elastic ligatures ran over the gold bar and then through the holes in the vulcanite base plate to a gold hook on the palate. When activated they helped to reduce the incisor prominence. He was the first person to introduce the concept of functional orthopaedics to correct a class II malocclusion by “jumping the bite”. “The object was not to protrude the lower teeth, but to change or jump the bite in the case of an excessively retreating lower jaw. The objection urged against the use of an incline , because the time required against the use of an incline, because the time required had tendency to alter the articulation of the teeth, was in this case an argument in its favour, and an advantage, because a new articulation was desired and the incline, as adapted, offered no opposition to the antagonism of the teeth. The principle of the inclined plane is always operating in the mouth, and may often be taken advantage of beneficially, while at other times it will tax our ingenuity to the utmost to overcome its powerful influence”.
![Figure 10: Upper inclined plane appliance for “jumping the bite.” Rodrigues Ottolengi [18] stated in 1907 that “Dr. Kingsley long ago announced the doctrine of “jumping the bite” but Dr. Angle has pointed out that in cases treated after the full complement of teeth has erupted while of course the bite may be jumped, the mandible will not always remain in forward pose. Clearly an age factor is involved and Ottolengui recommended “releasing the mandible from its imprisionment as early as possible”.](/fulltextimages/14233/fig_10.png)
Figure 10: Upper inclined plane appliance for “jumping the bite.” Rodrigues Ottolengi [18] stated in 1907 that “Dr. Kingsley long ago announced the doctrine of “jumping the bite” but Dr. Angle has pointed out that in cases treated after the full complement of teeth has erupted while of course the bite may be jumped, the mandible will not always remain in forward pose. Clearly an age factor is involved and Ottolengui recommended “releasing the mandible from its imprisionment as early as possible”.
To quote Bogue [19] “its peculiarity consists in this, that whilst nearly every other regulating operation aims simply at altering the position of the teeth in relation to the jaw which carries them, this operation alters the relation existing between the jaws themselves”.
“The operation is called for in cases where the upper incisors project, where the lowers bite far behind them, and where, besides these conditions, the bicuspids and molars inter-articulate abnormally, the lowers closing too far back, by the whole width of a tooth, the chin being consequently very retreating, and the whole facial expression weak and foolish”.
“What has to be done here, if possible, independently of some retraction of the upper incisors, is an alteration in the position of the lower jaw, so that the chin may be brought forwards”.
“Having drawn back some prominent upper incisors in a case with a markedly retreating chin, and desiring to keep them in position, I attached a retaining wire to gold caps made to fit the second upper bicuspids. In order to prevent the bicuspids themselves being braught forward, instead of the incisors being held back, I furnished the caps with tiny inclined planes directed downwards and backwards for the lower bicuspids to bite against. In a weeks time it was noted that the lower jaw had come right forward by the width of a tooth, and the retreating chin offended ones eye no longer”.
Pre-Functional Upper Arch Expansion
Dolomore [16] in his paper on inferior retrusion in 1923 states “when the mandible bites forward it is apparent that the upper arch is too narrow to allow normal occlusion of the molars in this position”. Therefore it is necessary to expand the upper arch. He recommends the Badcock screw.
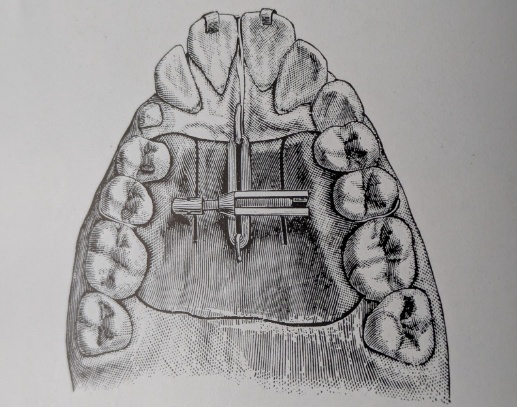
Weinberger [20] in a historical review of Kingley’s work in 1926 stated “Treatment involves widening the upper arch so that the lower teeth could not articulate, compelling a new articulation in an advanced position, flattening the v shaped arch”. An upper removable vulcanite plate with a jack screw was used to achieve this (Figuure 11). This was followed by “jumping the bite” with the upper inclined plane appliance (Figure 10). “The plan which I formed to correct this deformity was the result of my own judgment and partly to humour the strong desire of the mother that it should be done if possible without extracting any teeth”. Etchings show before and after treatment (Figure 12). A similar approach has been adopted by all later functional appliance systems as demonstrated by the paper on the early origins of Functional Jaw Orthopaedics by Trenouth [21] in 2024.
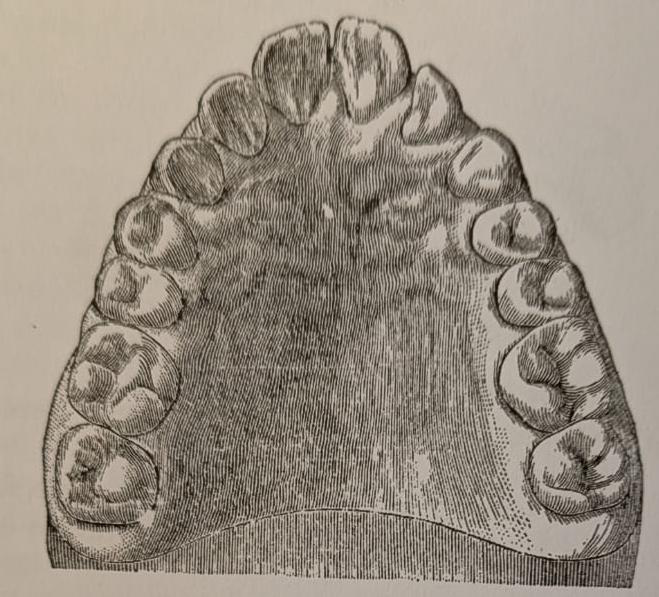
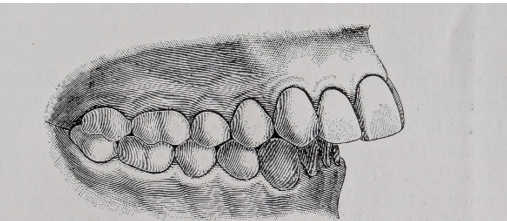
In a case published by Dr. Bogue in the Dental Cosmos May 1887 [22]. “The bite was jumped simply expansion of the upper arch in the canine region” (Figures 13 & 14). The occlusion changed from Class II to Class I relationship (Figures 15 & 16).
Airway and Functional Jaw Orthopaedics
Pierre Robin (1867-1950) first trained as a pharmacist then a dentist and finally became a Doctor of Medicine. He served as a maxilla-facial surgeon in the first World War [23]. He described a condition he named “glossoptosis” which involved backward movement of the tongue and mandible caused by narrowing of the maxilla. This led to enlarged adenoids, mouth breathing, airway obstruction, being pidgeon chested, failure to thrive and being backward at school.
The article by Robin in 1902 which is often quoted is in fact two separate papers published in the same volume of the journal. The first described maxillary expansion using an upper removable vulcanite appliance with an expansion screw [24]. The second describes the monoblock to correct Class II jaw relationships [25]. The long term effect was to treat mandibular hypoplasia and glossoptosis by enlarging the airway.
Further Ottolengui [18] states Adenoids compel mouth breathing and mouth breathing produces irregularity. Drooping of the mandible takes the tongue away from its normal place against the vault allowing lateral pressure from the cheeks to narrow the upper arch. This leads to deficient development of the mandible. ie Class II malocclusion.
Oropharyngeal Airway and Skeletal Pattern
Oropharyngeal airway size has been shown to be related to skeletal pattern being greater in Class III than Class II and intermediate in Class I [26]. Also Class I and Class II subjects with vertical growth patterns have significantly narrower upper pharyngeal airways [27]. Class II malocclusion is known to be associated with oral breathing especially where there is mandibular retrusion and increased lower face height [28]. There has been shown to be a reduction in oropharyngeal airway size after headgear treatment [29, 30, 31, 32]. More important a reduction in oropharyngeal airway size has been shown to take place after extraction of premolars and incisor retraction [33, 34, 35, 36, 37, 38].
Hakan, et al. [39] found the minimal cross-sectional area of the oropharynx correlated with Go-Gn (r=0.39) to a greater extent than SNB (r=0.22). Similar results were found by Trenouth, et al. [26] OPA with Go-Me (r=0.5) SNB (r=0.2), and Trenouth, et al. [40] OPA with Go-Me (r=0.3). The increase in the oropharyngeal airway was mainly related to lengthing of the mandible (Go-Gn/Me) rather than its position relative to the cranial base (SNB). The hyoid bone tends to follow the mandible as the airway increases. A significant correlation has been found between jaw relation hyoid position and width of the pharyngeal cavity by Allhaija, et al. [41]. Jenna, et al. [42] showed that the axial inclination of the hyoid bone closely followed that of the mandible in three groups of patients based on high, low and average Frankfort mandibular plane angle. Similar results were found by Ghodke, et al. [43].
Timms, et al. [44] found that increased maxillary mandibular planes angle and facial lengthening and narrowing were associated with increased nasal airway resistance.
Obstructive Sleep Apnoea and Oropharyngeal Dimension
Patients with obstructive sleep apnoea have been shown to have reduced dimensions of the oropharyngeal airway [45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55]. Ghodke, et al. [43] found that sagittal distances, cross-sectional area and volume measurements of the oropharyngeal airway all had negative correlation with the apnoea-hyponea index and positive correlation with sleep efficiency and mean oxygen saturation. Obstructive sleep apnoea syndrome is characterised by signs and symptoms related to arterial oxygen desaturation with cessation of breathing resulting in arousal and sleep fragmentation caused by pharyngeal obstruction during sleep. Obstructive sleep apnoea can result in serious morbidity and mortality mainly as a result of cardiovascular disease and road traffic accidents [56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66]. Children with obstructive sleep apnoea are more prone to having poor learning skills, behavioural problems, attention deficit hyperactivity disorder and depression [67, 68, 69, 70, 71].
The site of airway obstruction during episodes of apnoea is usually located in the oropharyngeal region involving the soft palate, dorsum of the tongue and posterior pharyngeal wall. The most constricted area of the airway has an inverse relation to the resistance to air flow. Poiseulle’s law [72] demonstrates that even a modest decrease in radius of the airway will result in a disproportionate increase in airway resistance (halving the radius results in a 16 times increase in resistance, because resistance is inversely proportional to the fourth power of the radius.
Class II correction using functional appliances has been found not only to enlarge the oropharyngeal airway but to improve nocturnal breathing. Schulz, et al. [73] found Maxillary expansion followed by Herbst appliance treatment decreased the number of respiratory effort -related arousals and respiratory disturbance index.
Systematic reviews have shown that functional jaw orthopaedics has a positive influence on the airway [74, 75].
Mahony, et al. [76] 2025 tested for obstructive sleep apnoea obstructive sleep apnoea in 100 adults (50 OSA & 50 Controls). They found a correlation between obstructive sleep apnoea and intermolar distance and also palatal height.
Mahony, et al. [77] 2025 studied 3671 children aged between 7 and 9 years of age on there first orthodontic consultation. Of those who had an apnoea/hyponea index >11, 87.3 % had a long facial pattern, Class II facial profile, maxillomandibular retrusion. Class III and Class I cases all had lower AHI scores. Discussion and Conclusion Class II division 1 malocclusion is the most common condition the orthodontist has to deal with. It is in part both a dentoalveolar and skeletal deformity. It is therefore important to treat both components when established methods are available to achieve these ends. The alternative is compromise dentoalveolar correction only, which involves premolar extractions converting a Class II division 1 malocclusion into a Class II division 2 malocclusion leaving a residual skeletal disproportion. This can alter the profile and flatten the face. There is also evidence that such an approach will reduce the airway and increase the susceptibility to sleep disordered breathing and sleep apnoea. The alternative involves upper arch expansion to achieve dentoalveolar alignment followed by functional jaw orthopaedics to correct the skeletal disproportion. This latter approach reduces the need for extractions, improves the profile and enhances the airway. It should be the treatment of choice where it is clinically feasible.
References
-
Peck S, Peck H (1979) Frequency of tooth extraction in orthodontic treatment. Am J Orthod 76(5): 491-496.
-
Bunon R (1743) Essay sur les maladies des dents. Paris: Briasson.
-
Lefoulon PJ (1841) Nouveau traite theorique et pratique de l’art du dentist. Paris: Chamerot.
-
Coffin WH (1881) A generalized treatment of irregularities. J Br Dent Ass 2: 587-595.
-
Case CS (1913) The question of extraction: an answer to Dr. Ferris’ discussion. Dent Cosmos 55: 54-55.
-
Tweed CH (1945) A philosophy of orthodontic treatment. Am J Orthod 31: 74-85.
-
Begg PR (1954) Stone age man’s dentition. Am J Orthod 40: 289-312.
-
Proffit WR (1994) Forty-year review of extraction frequencies at a university orthodontic clinic. Angle Orthod 64: 407-414.
-
Peck S (2017) Extractions, retention and stability: the search for orthodontic truth. Eur J Orthod 39(2): 109- 115.
-
Chupein TF (1894) Protrusion of the upper teeth regulated. In: Byrd CP (Ed.), Catchings Compendium of Practical Dentistry. Atlanta, USA, pp: 185-188.
-
Cutter HE (1894) Drawing the lower jaw forward. In: Byrd CP (Ed.), Catchings Compendium of Practical Dentistry. Atlanta, USA pp:167-169.
-
Cutter HE (1894) A case of drawing the lower jaw forward. Int Dent J (Phila) 15(6): 353-355.
-
Hamilton HF (1892) Description of a case of regulating. Int Dent J (Phila) 13(6): 416-447.
-
Hamilton HF (1892) Throwing the lower jaw forward. Catchings Compendium of practical dentistry. In: Byrd CP (Ed.), Atlanta, USA, pp: 180-181.
-
McBride RD (1904) Modern developments in orthodontia. Dent Rev Chicargo 18: 1029-1051.
-
Dolamore WH (1925) Inferior retrusion. Int J Orthod Oral Surg Radiol 11: 50-65.
-
Kingsley NW (1880) A treatise on oral deformities as a branch of mechanical surgery: In: Appleton D (Ed.), USA.
-
Ottolengi R (1907) A contribution to knowledge of the etiology and treatment of cases in Class II. Amer Soc Orthodontia pp: 495-514.
-
Matheson L (1891) Some practical points involved in the relation of the upper to the lower teeth. Trans Odont Soc Great Britain 23:6-31. Quoted Dr. Bogue (3) “Jumping” the bite pp: 23-25.
-
Weinberger BW (1926) Orthodontics an historical review of its origin and evolution. St Lois, Mosby Co. 2: 487-413.
-
Trenouth MJ (2024) Early Origins of Functional Jaw Orthopaedics. J Dent Sci 9(4): 000409.
-
Bogue EA (1887) Case of undue prominence of the upper jaw. Dental Cosmos 29: 318-325.
-
Robin P (1934) Glossoptosis due to atrisia and hypotrophy of mandible. Amer J Dis Child 48: 541-547.
-
Robin P (1902) Observation sur un novel appareil de redressment. Rev Stomat 9: 423-432.
-
Robin P (1902) Demonstration practique sur la construction et la mise on bouch d’un nouvel appariel de redressement. Rev Stomatol 9: 561-590.
-
Trenouth MJ, Desmond SR (2016) A cephalometric evaluation of oropharyngeal airway changes during Twin-block appliance treatment. Int J Dentistry Oral Sci S4:004: 22-30.
-
De Fretus MR, Alcazar NMPV, Janson G, De Fretus KMS, Henriques JFC (2006) Upper and lower pharyngeal airways in subjects with Class I and Class II malocclusions and different growth patterns. Am J Orthod Dentofacial Orthop 130(6): 742-745.
-
Rossi RC, Rossi NJ, Rossi NJC, Yamashita HK, Pignatari SSN (2015) Dentofacial characteristics of oral breathers in different ages: a retrospective case-control study. Progress in Orthod 16: 23.
-
Priller-Parkkinen K, Pirttiniemi P, Nieminen P, Lopponen H, Tolonen U, et al. (1999) Cervical headgear therapy as a factor in obstructive sleep apnea syndrome. Pediatr Dent 21(1): 39-45.
-
Godt A, Koos B, Hagen H, Goz G (2021) Changes in upper airway width associated with Class II treatments (headgear vs Activator) and different growth patterns. Angle Orthod 81(3): 440-446.
-
Hiyama S, Ono T, Ischiwata Y, Kuroda T (2001) Changes in mandibular position and upper airway dimension by wearing cervical headgear during sleep. Amer J Orthod Dentofacial Orthop 120(2): 160-168.
-
Lalani O (2015) Fluid mechanic impacts of cervical headgear on the structure and function of the upper airway. J Intigrated Cranio Dent 2: 21-28.
-
Xu K, Chen W, Liu Y (2010) Effects of large retraction of incisors due to orthodontic treatment on the upper airway dimensions in young adult patients with malocclusion. J Clin Stomatol 26: 600-603.
-
Germec-Cakan D, Taner T, Akan S (2011) Uvelo- glossopharyngeal dimensions in non-extraction, extraction with minimum anchorage and extraction with maximum anchorage. Eur J Orthod 33(5): 512-520.
-
Wang Q, Jia P, Anderson NK, Wang L, Lin J (2012) Changes in pharyngeal airway size and hyoid bone position following orthodontic treatment of Class I bimaxillary protrusion. Angle Orthod 82(1): 115-121.
-
Chen Y, Hong L, Wang CL, Zhang S, Cao C, et al. (2012) Effect of large incisor retraction on upper airway morphology in adult bimaxillary protrusion patients. Angle Orthod 82(6): 964-970.
-
Sharma K, Shrivastav S, Sharma N, Hotwani K, Murrell MD (2014) Effects of first premolar extraction on airway dimensions in young adolescents: A retrospective cephalometric appraisal. Contemp Clin Dent 5(2): 190- 194.
-
Hu Z, Yin X, Lao J, Zhou C, Yang Z, et al. (2015) The effect of teeth extraction for orthodontic treatment on upper airway: a systematic review. Sleep Breath 19(2): 441- 451.
-
Hakan E, Palmo JM (2013) An airway study of different maxillary and mandibular sagittal positions. Eur J Orthod 35(2): 262-270.
-
Trenouth MJ, Timms DJ (1999) Relationship of the functional oropharynx to craniofacial morphology. Angle Orthod 69: 419-423.
-
Allhaija ESA, Al-Khateeb SN (2005) Uvulo-glosso- pharyngeal dimensions in different anteroposterior skeletal patterns. Angle Orthod 75: 1012-1018.
-
Jenna AK, Duggal R (2011) Hyoid bone position in subjects with different vertical jaw dysplasias. Angle Orthod 81: 81-85.
-
Ghodke S, Utreja AK, Singh SP, Jenna AK (2014) Effects of twin-block appliance on the anatomy of the pharyngeal airway passage (PAP) in Class II malocclusion subjects. Prog Orthod 15: 68-76.
-
Timms DJ, Trenouth MJ (1999) A quantified comparison of craniofacial form with nasal respiratory function. Am J Orthod Dentofacial Orthop 94: 216-221.
-
DeBerry-Borowiecki B, Kykwa A, Blanks B (1998) Cephalometric analysis for diagnosis and treatment of obstructive sleep apnoea. Laryngoscope 98(2): 226-234.
-
Sher AE (1990) Obstructive sleep apnoea syndrome: A complex disorder of the upper airway. Otolaryngol Clin North Am 23(4): 593-608.
-
Riley RW, Guilleminault C, Herran J, Powell N (1983) Cephalometric analysis of flow-volume loops in obstructive sleep apnoea patients. Sleep 6(4): 302-311.
-
Bohlman ME, Haponik EF, Smith PL, Allen RP, Bleecker ER, et al. (1983) CT demonstration of pharyngeal narrowing in adult obstructive sleep apnoea. Am J Roentgenol 140: 543-548.
-
Lyberg T, Krogstad O, Djupesland G (1989) Cephalometric analysis in patients with obstructive sleep apnea syndrome: I. Skeletal Morphplogy. J Laryngol Otol 103: 287-292.
-
Lyberg T, Krogstad O, Djupesland G (1989) Cephalometric analysis in patients with obstructive sleep apnea syndrome: II. Soft tissue morphology. J Laryngol Otol 103(3): 293-297.
-
Strelzow VV, Blanks RH, Basile A, Strelzow AE (1998) Cephalometric airway analysis in obstructive sleep apnea syndrome. Laryngoscope 98(11): 1149-1158.
-
Partinen M, Guilleminault C, Quera-Salva MA, Jamieson A (1998) Obstructive sleep apnea and cephalometric roentgenograms: The role of anatomic upper airway abnormalities in the definition of abnormalities in the definition of abnormal breathing during sleep. Chest 93(6): 1199-1205.
-
Crumley RL, Stein M, Gamsu G, Golden J, Dermon S (1987) Determination of obstructive site in obstructive sleep apnoea. Laryngoscope 98: 301-308.
-
Pracharktam N, Nelson S, Hans MG, Broadbent BH, Redline S, et al. (1996) Cephalometric assessment in obstructive sleep apnea. Am J Orthod Dentofacial Orthop 109:410-419.
-
Battagel JM, Johal A, Kotecha B (2000) A cephalometric comparison of subjects with snoring and obstructive sleep apnoea. Eur J Orthod 22(4): 353-365.
-
He J, Kryger MH, Zorick FJ, Conway W, Roth T (1998) Mortality and apnea index in obstructive sleep apnea. Experience in 385 male patients. Chest 94(1): 9-14.
-
Gonzalez-Rothi RJ, Foresman GE, Block AJ (1998) Do patients with sleep apnea die in their sleep? Chest 94(3): 531-538.
-
Findlay L, Levinson M, Bonnie R (1992) Driving performance and automobile accidents in patients with sleep apnoea. Clin Chest Med 13(3): 427-435.
-
Partinen M, Jamieson A, Guilleminault C (1998) Long- term outcome for obstructive sleep apnea syndrome patients mortality. Chest 94: 1200-1204.
-
Ancoli-Isreal S, Kripke DF, Klauber MR, Fell R, Strepnowsky C, et al. (1996) Morbidity, mortality and sleep-disordered breathing in community dwelling elderly. Sleep 19: 277-282.
-
Lavie P, Herer P, Peled R, Berger I, Yoffe N, et al. (1995) Mortality in sleep apnoe patients: a multivariate analysis of risk factors. Sleep 18(3): 149-157.
-
Nieto F J, Young TB, Lind BK, Shahar E, Samer JM, et al. (2000) Association of sleep-disordered breathing, sleep apnoea and hypertension in a large community-based study. Sleep Heart Health Study JAMA 283(14): 1829- 1836.
-
Sharar E, Whitney CW, Redline S, Lee ET, Newman AB, et al. (2001) Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the Sleep Heart Health Study. Am J Respir Crit Care Med 163(1): 19-25.
-
Barbe B, Percas J, Munoz A, Findley L, Anto L M, et al. (1998) Automobile accidents in patients with sleep apnea syndrome. An epidemiological and mechanistic study. Am J Respir Crit Care Med 158(1): 18-22.
-
Klitzman D, Miller A (1994) Obstrructive sleep apnea syndrome: complications and sequelae. Moint Sinai J Med 61(2): 113-121.
-
Marin JM, Carrizo SJ, Vicente E, Agusti AG (2005) Long- term cardiovascular outcomes in men with obstructive sleep apnoea-hyponoea with or without treatment with continuous positive airway pressure: an observational study. Lancet 365(9464): 1046-1053.
-
Ali N, Pitson DJ, Stradling JR (1993) Snoring, sleep disturbance and behaviour in 4-5 year olds. Arch Dis Child 68(3): 360-366.
-
Weissbluth M, Davies AT, Poncher J, Reiff J (1983) Signes of airway obstruction during sleep and behaviour developmental and academic problems. J Dev Behav Pediatr 4(2): 119-121.
-
Chervin RD, Dillon JE, Bassetti C, Ganoczy DA, Pituch KJ (1997) Symptoms of sleep disorders, inattention and hyperactivity in children. Sleep 20: 1185-1192.
-
Goldstein NA, Post JC, Rsenfield RM, Campbell TF (2000) Arch Otolaryngol Head Neck Surg 126: 494-498.
-
Gozal D (1998) Sleep-disordered breathing and school performance in children. Pediatrics 102: 612-620.
-
Pfitzner J (1976) Poiseulle and his law. Anaesthesia 31(2): 273-275.
-
Schutz TCB, Dominguez GC, Hallinan MP, Cunha TCA, Tufik S (2011) Class II correction improves nocturnal breathing in adolescents. Angle Orthod 81(2): 222-228.
-
Anusuya V, Jenna A K, Sharan J (2019) Effects of functional appliance treatment on pharyngeal airway passage dimensions in Class II malocclusion subjects with retrognathic mandibles: A systematic review. APOS Trends in Orthodontics 9: 138-148.
-
Abdella Y, Sonnesen L (2024) Association between orthodontic treatment and upper airway changes in children assessed with cone-beam computed tomography (CBCT): Asystematic review. J Oral Rehabil 51: 2195-2208.
-
Mahony D, Harding S, Chowdhury CR, Jamilian A, Fetrati A, et al. (2025) Correlation between severity of Obstructive Sleep Apnoea and Dental Arch Form in adults. J Clin Med 14(20): 7183.
-
Mahony D, Bhattari N, Simona C, Rosaria B, Borbely P, et al. (2025) Facial Patterns and Obstructive Sleep Apnoea in Children seeking for Orthodontic Treatment: Data from 3671 polysomnographic recordings. Orthod Craniofac Res 29(3): 497-505.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells