A Case of Embryonal Rhabdomyosarcoma of Cervix Uteri in a 14 Year Old Girl
Rhabdomyosarcoma is an aggressive soft tissue malignancy of childhood and adolescence arising from embryonal mesenchyme [1]. As compared to literature available, these tumours are mainly discussed in context of case studies. Most common affected sites are head, neck, abdomen and genitourinary tract [2].
Introduction
Rhabdomyosarcoma is an aggressive soft tissue malignancy of childhood and adolescence arising from embryonal mesenchyme [1]. As compared to literature available, these tumours are mainly discussed in context of case studies. Most common affected sites are head, neck, abdomen and genitourinary tract [2]. Embryonal rhabdomyosarcoma is the most common subtype, of which botryoid is a polypoidal variant. Botryoid rhabdomyosarcoma of female genital tract involves uterus, cervix and vagina, among which cervical type is a rare one. Due to involvement of younger age group, its management poses a clinical change as preservation of hormonal, sexual and reproductive function is essential.
Case History
A 14yr old girl presented to our Gynae-OPD with chief complaints of irregular bleeding pv off & on associated with passage of fleshy discharge pv off & on for last 4m. She attained her menarche 1yr back and her menstrual cycles were regular till the onset of presenting complaints. There was no significant medical or surgical history in the past. On general and systemic examination nothing abnormally was detected. On local examination, it was normal except that on straining, a yellowish, vesicular-like structure protruded through the vagina. EUA revealed a friable, fleshy polypoidal growth arising from the right anterolateral aspect of ectocervix. All the fornices and vaginal wall were smooth and free. Per vaginal examination, uterus was normal size, mobile and parametrium was free.
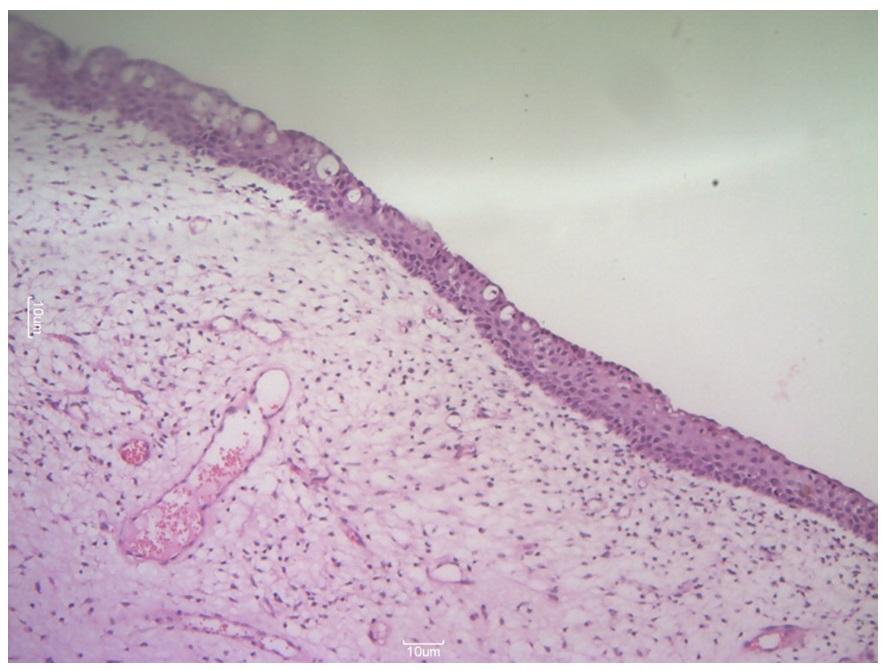
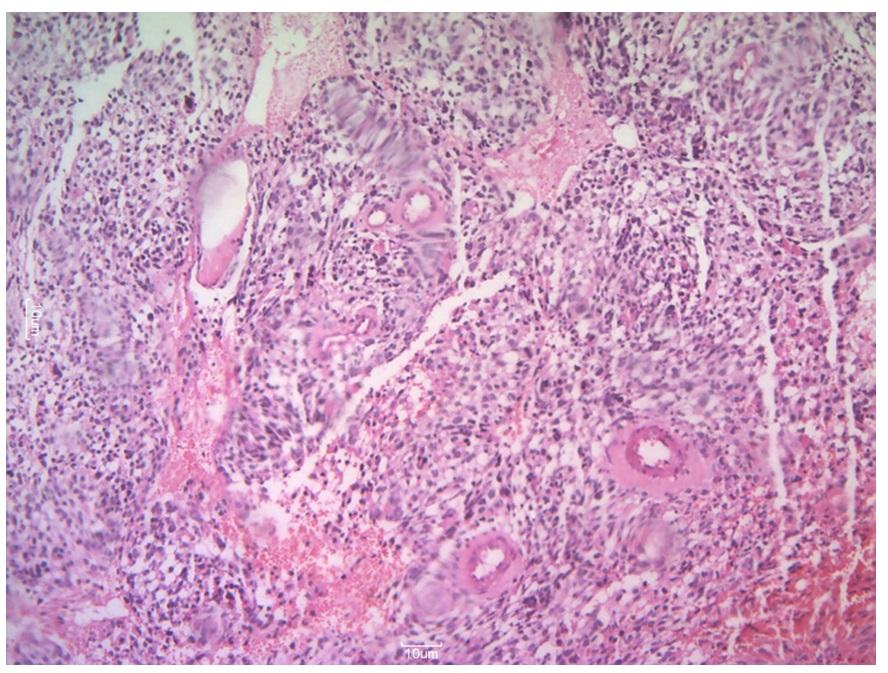
USG – revealed a heterogenous hypoechoic mass of approx. 5X5cm in vagina, interface with anterior lip of cervix not well defined. CFI showed mild vascularity within the lesion (needs histopathological correlation), others nothing abnormally detected. This finding was confirmed by MRI which also revealed the localized and limited nature of the lesion, other organs including uterus not involved. CXR was also normal i.e. no evidence of metastasis. All routine blood investigations were within normal limits. After its classification as stage-Ia (according to Intergroup Rhabdomyosarcoma Study Group clinical classification system), fertility-sparing surgery i.e.local excision was done and its base on ectocervix was coagulated with electric cautery. Post-op she was referred for chemotherapy and was given 3 cycles of VAC. HPE (Figure 1) was suggestive of mesenchymal tumour arranged in form of sheets of small tumor cells with dense cellularity around blood vessels. At few places round cells with high N:C ratio, vacuolated cytoplasm, round-to-oval hyperchromatic nuclei with marked pleomorphism and increased mitotic activity, seen in clusters. Focal myxoid areas were also noted with areas of haemorrhage and necrosis. With final impression of Embryonal Rhabdomyosarcoma(Botroid subtype), IHC was suggested for further evaluation.

Discussion
Rhabdomyosarcoma is a highly malignant soft tissue tumour of childhood and adolescence accounting for 4- 6% of all malignancies in this age-group [1]. According to WHO, it is classified into embryonal, alveolar, pleomorphic and spindle cell / sclerosing rhabdomyosarcoma [3]. In genitourinary tract, though vagina is the most common site, but 0.5% occurs primarily in cervix [4]. Usually the primary site is vagina in infancy and early childhood, cervix in early reproductive age and corpus uteri in post menopausal women [5]. According to a study the median age of involvement in case of cervix is 13 years as compared to other anatomic sites in which 80% presents before 9 years [6]. Botryoid type of cervical embryonal rhabdomyosarcoma typically grows in polypoidal fashion, sessile or pedunculated, soft, with grape-like clusters. Most common presenting symptom is feeling of mass at introitus with or without bleeding or discharge per vaginum. Its pathologic diagnosis is usually confirmed by immunohistochemistry which is positive for Desmin, Vimentin and Myogenin apart from increased proliferative activity and hormone receptor expression is usually absent7. Traditionally the treatment has been radical i.e. hysterectomy but recently the trend has been changed towards conservation of genitourinary organs by fertility sparing surgery along with chemotherapy and / or radiation with no change in survival rate especially in early localized disease [6, 7]. Though this should not be considered in presence of metastasis or extensive uterine involvement. In patients with localized disease, the overall survival rate is more than 80% with combined use of surgery and chemoradiation whereas in metastatic disease it is less than 30% [8]. A study has shown the survival rate in case of cervix to be 96% as compared to vaginal with 60% only [9]. Among chemotherapy VAC regimen is still considered to be most effective5. Radiotherapy is usually reserved for residual diseases [10]. Hence, knowledge of this uncommon lesion at this site and its clinical implications are important to avoid misdiagnosis as early disease stage at diagnosis is a highly favourable prognostic factor [11].
Conclusion
Awareness of this rare rapidly growing tumour in younger age-group is essential to reach final diagnosis and limited surgery along with or without chemotherapy has good prognosis especially in early stage rhabdomyosarcomas.
References
-
Behtash N, Mousavi A, Tehranian A, Khanafshar N, Hanjani P (2003) Embryonal rhabdomyosarcoma of the uterine cervix: case report and review of literature. Gynecol Oncol 91(2): 452-455.
-
Dehner LP (2011) Soft tissues. In: Stocker TJ, et al. (Eds.), Stocker and Dehner's Pediatric Pathology, (3rd edn), Wolter Kluwer-Lippincott Williams & Wilkins, Philadelphia, pp. 1079-1087.
-
Fletcher C, Bridge J, Hogendroom P, Mertrens F (2013) WHO Classification of Tumours of Soft Tissue and Bone. (4th edn), Lyon: IARC 5(5): 468.
-
Kriseman ML, Wang WL, Sullinger J, Schmeler KM, Ramirez PT, et al. (2012) Rhabdomyosarcoma of the cervix in adult women and younger patients. Gynecol Oncol 126(3): 351-356.
-
Atlante M, Dionisi B, Cioni M, Di Ruzza D, Sedati P, et al. (2000) Sarcoma botryoides of the uterine cervix in a young woman: A case report. Eur J Gynaecol Oncol 21(5): 504-506.
-
Dehner LP, Jarzembowski JA, Hill DA (2012) Embryonal rhabdomyosarcoma of the uterine cervix: a report of 14 cases and a discussion of its clinicopathological associations. Mod Pathol 25(4): 602-614.
-
Li RF, Gupta M, McCluggage WG, Ronnett BM (2013) Embryonal rhabdomyosarcoma (botryoid type) of the uterine corpus and cervix in adult women: report of a case series and review of the literature. Am J Surg Pathol 37(3): 344-355.
-
Bernal KL, Fahmy L, Remmenga S, Bridge J, Baker J (2004) Embryonal rhabdomyosarcoma of the cervix presenting as a cervical polyp treated with fertility- sparing surgery and adjuvant chemotherapy. Gynecol Oncol 95(1): 243-246.
-
Gruessner SE, Omwandho CO, Dreyer T, Blutters- Sawatzki R, Reiter A, et al. (2004) Management of stage I cervical sarcoma botryoides in childhood and adolescence. Eur J Pediatr 163(8): 452-456.
-
Dayyabu AL, Adogu IO, Makama BS (2014) Sarcoma botryoides, a management dilemma: A review of two cases. Int J Case Rep Imag 5(7):15-20.
-
Bajpai N, Manjunath AP, Girija S, Pratap K (2015) Botryoid Rhabdomyosarcoma of the Cervix: Case report with review of literature. Sultan Qaboos Univ Med J 15(3): e433-e437.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’