Myomectomy and Pregnancies
Uterine fibroids may be encountered with pregnancy and many obstetricians will inevitably confront the dilemma of how best to manage fibroids causing complications in a gravid uterus. We describe one case of unavoidable caesarean myomectomy and myomectomy performed for the management of complications during pregnancy.
Introduction
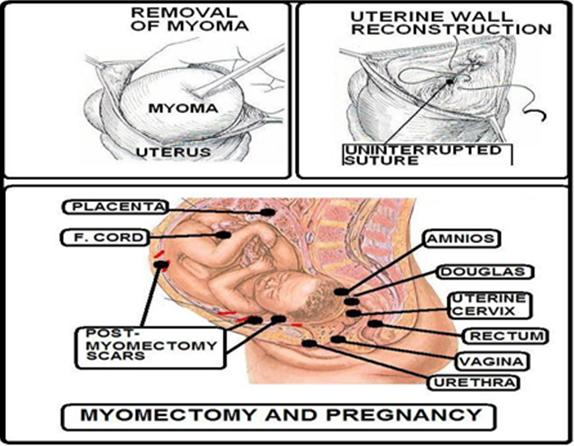
Myomas may cause infertility [1, 2, 3] and, in addition, may determine complications during pregnancy [4, 5, 6]. Unfortunately, the data regarding myomectomy for reproductive reasons are limited; they are mainly based on retrospective studies [2, 3] (Figure 1).
Till now, myomectomy has been considered a controversial procedure in non-fertile women: some authors suggest conservative surgery when there are no additional factors interfering with the pregnancy;
whereas others are in favour of waiting [2, 3, 7, 8, 9, 10, 11, 12, 13, 14, 15]. The previous doubts are correlated with the different hypothesis with which myoma can determine infertility; few reports are published on the efficacy of the treatment [16]. The pregnancy rate following myomectomy ranges between 55% and 76.9% [17, 18, 19, 20, 21]. These studies are limited owing to few cases, variable follow-up and additional factors [22]. The association between infertility and either intramural or subserous myoma without the abnormality of the uterine cavity is still controversial on the contrary, [2, 3, 10, 22] submucous myomas, that range between 5 and 8% of patients are considered responsible factors interfering with pregnancy [19, 20, 21, 23]. The main symptoms correlating with pregnancy are as follows: bleeding, pelvic pain, abortion, abnormal presentation, postpartum haemorrhage, puerperal infection [2, 23]. Submucous myoma can decrease uterine contractility thus reducing spermatic migration; besides, the vascular and morphologic modification of endometrial cavity is a relevant obstacle for implantation [24, 25, 26]. The aim of this report is to evaluate fertility and pregnancy outcome following laparotomic myomectomy.
Material and Methods
From 1988 to 2003, 473 patients within the fertile age underwent myomectomy surgery at the 1st Obstetric and Gynecological Clinic of Catania University. Surgery was performed in all cases by laparotomic route with the exception of the cases which undergone at the same time other surgery. The incision of the uterine wall was performed by electro surgery; during the operation, atraumatic skilfulness of microsurgery was performed (continuous washing of tissue and meticulous haemostasis by bipolar). Usually, the uterine wall reconstruction was made in one-two layer suture using vicryl uninterrupted suture (Figure 2). Serous layer was closed with continuous introflectent suture [27, 28, 29, 30, 31, 32, 33]. To avoid adherence formation interceed was used. In the case of multiple myomectomy, therapy with GnRh analogues was suggested. Mean follow-up was 5.2 years with a range of 1-13 years.
372(78.6%) were evaluated regularly at the follow-up; the others 101(21.4) were contacted by telephone or by e-mail. Each patient was asked news about the onset, the course and the exit of pregnancy following myomectomy, as well as eventual recurrences.
Results
We have subdivided the patients into three groups in relation to their age: A GROUP< 30 years 102(21.5%), B GROUP 30-39 years 281(59.4%), C GROUP 40-49 years old 90(19.1%); the most representative range was between 30 and 39 years of age (59.4%) (Table 1).
| Age range | Number of patients | % | |
|---|---|---|---|
| A Group < 30 years old | 102 | (21.5%) | |
| B Group 30-39 " | 281 | (59.4%) | |
| C Group 40-49 " | 90 | (19.1%) |
Table 1: [INLINE_TABLE:1:1]
Characteristics of myomas are shown on Table 2.
| Number of patients | % | |
|---|---|---|
| Site | ||
| Submucous | 75 | 15.8% |
| Intramural | 274 | 57.9% |
| Subserous | 124 | 26.3% |
| Number | ||
| Single | 226 | 47.7% |
| Multiple | 247 | 52.3% |
| Size | ||
| <5 cm | 95 | 20.1% |
| 5-9 cm | 292 | 61.8% |
| >9 cm | 86 | 18.1% |
Table 2: [INLINE_TABLE:1:2]
As regards the characteristics of myomas we have noticed that the most part had an intramural location (57.9%) followed by the subserous (26.3%) and by submucous myomas (15.8%). In our casuistic, small submucous myomas were excluded because treated hysteroscopically. No differences were found between number (single o multiple), resulting an incidence of 47.7% and 52.3% (P<0.0001), respectively. Myomas size was between 5 and 10 cm in 292 patients (61.8%), 5 cm in 95 patients (20.17%) and 10cm in 86 (18.1%) The indications to myomectomy are shown on Table 3.
| Indication | Number of patients | % |
|---|---|---|
| Blood loosing | 98 | 20.7% |
| Pelvic pain | 163 | 34.5% |
| Size of myoma | 78 | 16.4% |
| Sterility | 75 | 15.9% |
| Infertility | 46 | 9.7% |
| No symptoms | 13 | 2.7% |
Table 3: [INLINE_TABLE:2:0]
Pelvic pains consist of the pre-dominant symptoms (34.5%) followed by blood loosing (20.6%); whereas sterility and fertility weight upon 15 and 9.7%, respectively. 67.8% (321/473) were nulliparae, 15.3% referred to have previously 1 or more abortions (respectively 8.9% and 6.4%), whereas 80 patients (16.9%) had one or more pregnancies at term. A very few intra e postoperative complications were found. Only 5 (1%) patients requested haemotransfusion. Feverish postoperative course happened in 1% . In no cases hysterectomy was done owing to complications. Post-myomectomy pregnancy rate (PR) is shown on Table 4.
| Patients number | PR | |
|---|---|---|
| Whole PR | 157/230 | 68.2% |
| PR on patients with | 34/74 | 45.3% |
| PR on patients with | 22/46 | 47.9% |
| PR on patients with multiple indications | 101/110 | 91.8% |
Table 4: [INLINE_TABLE:2:0]
Only 230 patients among 473 patients wanted their pregnancy; whole pregnancy rate was of 68.2% (157/230 patients). Subdivision relating surgical indication evidenced the most significant value in the group with different indications from infertility and sterility (91.8% versus 47.9%-45.3%). Regarding the correlation between the age of the patient at the time of surgery and the pregnancy rate, we have noted a greater incidence of pregnancy (72.2%) in women younger than 35 years of age whereas in those older than 35 years, 52.4% obtained pregnancy (Table 5).
| Age | Patients number | PR | PR |
|---|---|---|---|
| 230 | 157 | 68.2% | |
| <35 | 169 | 122 | 72.2% |
| 35 | 61 | 32 | 52.4% |
Among 157 pregnancies, 17(11.3%) were spontaneous abortions, 13 (8.7%) preterm deliveries, 120 (80%) pregnancies at term and, finally, 7 are in progress. 11.4% (18 patients) had their pregnancy within 12 months, 44.6 % (70 patients) had their pregnancy after one year from surgery and 44%(69 patients) after 2 years. Regarding the modality of birth, caesarean section was performed in 55.6% (74 patients) and vaginal birth in 44.4% (59 patients). As for as the weight of the newborns, in 81.2 % the weight ranged between 10° and 90° percentile. During the period of follow-up (range 1-13 years) 76 patients had recurrences of myoma (16%): of these 48.6% requested further surgery.
Discussion and Conclusion
Uterine myoma represents a benign tumour that frequently develops during the fertile age. In our cases, the period of 30 and 39 years of age (59.4%) was the most involved. We believe opportune to perform laparotomic myomectomy on the patients who are still wanting pregnancy when multiple and voluminous myomas are found. Among complications, only 1% had post- surgical hyperpexia and haemotransfusion. Our pregnancy rate, 68.2% is in line with other studies conducted on patients who did not show other causes of infertility: 72.4%, 60% [34, 35]. The pregnancy rate in the group of patients with positive anamnesis for infertility or sterility (56/121) suggests that the presence of intramural myomas (that represent the majority of our casuistics) could influence negatively on the fertility. The pathogenic mechanism could be conducted to an alteration of normal uterine contractility or to a reduced haematic flow in the endometrial site that could interfere both with spermatic migration or with the implantation of the ovum. Among the factors preventing pregnancy after myomectomy, we may consider the age of patients; pregnancy rate reaches 72.2% on women < 35 years, whereas 52.4% in women 35 years old. Our data are in accordance with other authors [36] who consider the age, the main factor determining pregnancy rate. With regards to the modality of delivery following myomectomy in our casuistic, caesarean section was performed in 55.6% of cases, whereas vaginal delivery in 42.1%. No uterine rupture was recorded. Laparotomic
myomectomy is a procedure with few complications; in most cases following preservative operation, the patient obtains the pregnancy with a satisfactory outcome. The influence of the myomas on the fertility is still controversial owing to difficulty in evaluating efficacy of treatment in a sterile patient; the selection of women where myoma is the only factor preventing pregnancy is very hard [37, 38, 39, 40, 41, 42, 43, 44]. Furthermore, it is very interesting to note that more than half of the patients operated for myomectomy because of either polyabortivities or sterility obtain a successful pregnancy in a short period. Evaluating previous considerations, the laparotomic myomectomy is a suitable procedure for patients suffering with uterine myomas and sterility not understood; in addition, it should be judged elective surgery on women at reproductive age, desiring pregnancy while still young.
Acknowledgment
Valentina Pafumi has carried out English language editing for this article.
References
-
Babaknia A, Rock JA, Jones HW (1978) Pregnancy success following abdominal myomectomy for infertility. Fertil Steril 30(6): 644-648.
-
Buttram VC, Reiter RC (1981) Uterine leiomyomata: etiology, symptomatology and management. Feril Steril 36(4): 433-445.
-
Verkauf BS (1992) Myomectomy for fertility enhancement and preservetion. Fertil Steril 58(1): 1- 15.
-
Donnez J, Jadoul P (2002) What are implications of myomas on fertility? A need for debate? Hum Reprod 17(6): 1424-1430.
-
Dessolle L, Soriano D, Poncelet C, Benifla JL, Madelenat P, et al. (2001) Determinans of pregnancy rate and obstetric outcome after laparoscopic myomectomy for infertility. Fertil Steril 76(2): 370- 374.
-
Vercellini P, Maddalena S, De Giorni O, Pesole A, Ferrari L, et al. (1999) Determinans of reproductive outcome after abdominal myomectomy for infertilità. Fertility and Sterility 72(1): 109-113.
-
Deimer HP, Kozlosky P (1990) Schwanger schaftund myomectomy operieren? Gynakologe 23: 71-74.
-
Kommos F, De Gregorio G, Strittmatter B, Pfisterer J, Karck U, et al. (1993) Geburtshilfliche komplikationen. Frequent und indikationen der kaiserscchni hent bindungen bei uterus myomatosus. Geburtsh Frauenheilk 53: 564-567.
-
Rosenfeld DL (1986) Abdominal myomectomy for oterwise unexplained infertility. Fertil Steril 46(2): 328-330.
-
Buttran VC (1992) Indication for myimectomy. Reprod Endocrinol 20: 378-390.
-
Verkauf BS (1996) Myomectomy as a fertility promoting procedure. Infertility and reproductive medicine clinics of North America 7: 79-89.
-
Berkeley AS (1983) Abdominal myomectomy and subsequent fertility. Surg Gynecol Obstet 156(3): 319-322.
-
Paecock LM (1996) Indications for and tecnique of myomectomy. Infertility and Reproductive Medicine Clinics of North America 7: 109-127.
-
Poulsen RJ (1994) Value of myomectomy in the teatment of infertility. Fertil Steril 59(6): 1332-1333.
-
Acob Technical Bullettin. Uterine leiomyomata 192: 1-9.
-
Farhi J, Ashkenazi J, Feldberg D, Dicker D, Orvieto R (1995) Effect of uterine leiomyomata on the result of in vitro fertilization tattament.Hum Reprod 10(10): 2576-2278.
-
Stovall DW (1998) Sparks AET, Syrap cycles:results of a matched follow-up study. Hum Reprod 13: 192-197.
-
Ramzy AM, Sattar M, Amin Y, Mansour RT, Serour GI, et al. (1998) Uterine myomata and outcome of assisted reproduction. Hum Reprod 13(1): 198- 202.
-
Garcia CR, Tureck RW (2000) Submucosal leiomyomas and fertility. Fertil Steril 42(1): 16-19.
-
Bajekal N, Li TC (2000) Fibroids, infertility and pregnancy wastage. Hum Rprod Update 6(6): 614- 620.
-
Reyniak JV, Corenthal L (1987) Microsurgical laser technique for abdominal myomectomy. Mcrosurgery 8(2): 92-98.
-
Brooks PG, Loffer FD, Serden SP (1989) Resectoscopic removal of symptomatic intrauterine lesions. J Reprod Med 34(7): 435-437.
-
Carson LS, Brook PC (1991) Resectoscopic myomectomy. Fertil Steril 55(6): 1041-1044.
-
Sudik R, Hüsch K, Steller J, Daume E (1996) Fertility and pregnancy outcome after myomectomy in sterility patients. Eur J Obstet Gynecol Reprod Biol 65(2): 209-214.
-
Dubuisson JB, Lecuru F, Foulot H, Mandelbrot L, Aubriot FX, et al. (1991) Myomectomy by lapascopic :a preliminare report of cases. Fertil Steril 56(5): 827- 830.
-
Smith DC, Uhlir JK (1990) Myomectomy as a reproductive procedure. Am J Obstet Gynecol 162(6): 1476-1482.
-
Fauconnier A, Dubuisson JB (2000) Prognostic factors of reproductive outcome after myomectomy in infertile patients. Hum Reprod 15(8): 1751-1757.
-
Fedele L, Bianchi S (1995) Transvaginal ultrasonography versus histeroscopic myomectomy. Hum Reprod Update 1: 81-90.
-
Pritts EA (2001) Fibroids and infertility: a systematic review of the evidence. Obstet Gynecol Surv 56(8): 483-491.
-
Verkauf BS (1993) Value of myomectomy in the treatment of infertility. Fertil Steril 59(6):1332- 1333.
-
Friedmann W, Maier RF, Luttkus A, Schäfer AP, Dudenhausen JW (1996) Uterine rupture after laparoscopic myomectomy. Acta Obstet Gynecol Scand 75(7): 683-684.
-
Pafumi C, Leanza Vito, Carbonaro Antonio, Leanza Gianluca, Stracquadanio Maria Grazia, et al. (2011) Efficacy evaluation of a test CINtec® p16INK4a in screening for cervical HPV infection. open journal of preventive medicine 1(3): 154-163.
-
Pafumi C, Iraci Sm, Abate G, Clemente Cm, La Rosa I, et al. (2010) Protection of ovarian tissue from radiotherapy. Bratislavské Lekárske Listy 111(8): 443-448.
-
Zarbo G, Giunta MR, Giannone TT, Pafumi C, Leanza V (2014) Correlazione Tra Hpv E Adenocarcinoma Dell’ Endocervice. Gazzetta Medica Italiana. Archivio Per Le Scienze Mediche 173(5): 259-264.
-
Leanza V, Fichera S, Leanza G, Cannizzaro MA (2011) Huge fibroid (g. 3.000) removed during cesarean section with uterus preservation. A case report. Ann Ital Chir 82(1): 75-77.
-
Leanza V, D’Agati A, Accardi M, Russo ER (2009) Multiple myomectomy performed during cesarean section: a case report. Minerva Ginecologica 61(3): 245.
-
Rossetti A, Sizzi O, Soranna L, Mancuso S, Lanzone A (2011) Fertility outcome: long-term results after laparoscopic myomectomy. Gynecol Endocrinol 15(2): 129-134.
-
Dubuisson JB, Chavet X, Chapron C, Gregorakis SS, Morice P (1995) Uterine rupture during pregnancy after laparoscopic myomectomy. Hum Reprod 10(6): 1475-1477.
-
Malberti S, Rolla M, Vignali M (2003) Conservative surgical abdominal treatment of uterine myoma: recurrence and fertilità. J Gynaecol Obstet 15(1): 21- 28.
-
Seracchioli R, Rossi S, Covoni F (2008) Pregnancy rates in infertile women were similar after laparascopic or abdominal myomectomy of large myomata Hum Reprod 15: 2663-2668
-
Vercellini P, Maddalena S, De Giorgi O (1999) Determinats of reproductive outcome after abdominal myomectomy for infertility. Fertil Steril 72(1): 109-114.
-
Campo S, Campo V, Gambadauro P (2003) Reproductive outcome bifore and after laparascopic or abdominal myomectomy for subserous or intramural myomas. European J of Obstet Gynecol and Reproductive Biology 110(2): 215-219.
-
Dessolle L, Soriano D, Poncelet C, Benifla JL, Madelenat P, et al. (2001) Determinats of pregnancy rate and obstetric outcome after laparascopic myomectomy for infertility. Fertil Steril 76(2): 370- 374.
-
Dessolle L, Soriano D, Poncelet C, Benifla JL, Madelenat P, et al. (2003) Pregnancy outcome after laparascopic and laparoconverted myomectomy. European J of Obstet Gynecol and Reproductive Biology 108(2): 194-198.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’