Successful Treatment of Acquired Uterine Arteriovenous Fistula Following Induced Abortion: A Case Report and Literature Review
Aterioveinous malformation (AVM) means a vascular structural anomaly involving abnormal communication between arteries and veins that bypass the capillary system [1].
Introduction
Aterioveinous malformation (AVM) means a vascular structural anomaly involving abnormal communication between arteries and veins that bypass the capillary system [1]. It can be found anywhere in the vascular system, including uterus, and is divided into two sub- types: congenital and acquired. Congenital uterine AVM is thought to be secondary to abnormal embryonic differentiation; while acquired uterine AVM is a rare cause of life-threatening bleeding and is typically a result of any uterine trauma, surgical intervention (such as uterine curettage) or in the setting of a preexisting pathological process [2]. Arteriovenous fistula (AVF), as a kind of AVM, isa condition representing the direct connection of artery and vein without an intervening capillary bed. Similar to AVM, AVF also can be congenital or acquired. The venous system cannot accommodate the high pressure and high flow state as the arterial system, resulting in a higher propensity for bleeding. Uterine AVM accounts for 1%-2% of all genital hemorrhage [2]. Initial imaging always done by Color Doppler ultrasonography. Because the most of these two rarity involve women of reproductive age, fertility- sparing methods always need to be considered. Here we reported a case with acquired uterine AVM treated by laparoscopy combine with internal iliac artery embolization to preserve the uterus.
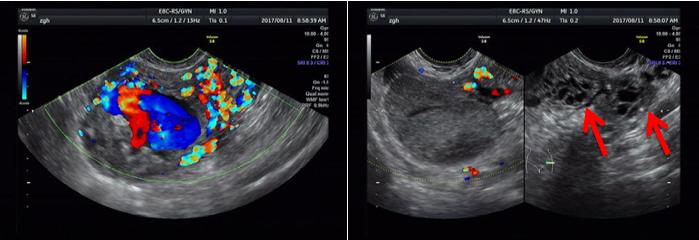
The left showed focus full of high-velocity, low- resistance blood flow. The right showed the typical characterization of honeycomb-like mass (red arrows). Meanwhile, a cyst with a size of 5.1x3.9x5.0cm3 was found at the right adnexa. Serum β-hCG level was 8.9mIU/ml. The patient denied vaginal bleeding, fever, nausea, vomiting, dizziness, chest pain and other discomfort.
After admission, we checked the vital signs for the patient and they were stable. Her laboratory studies revealed normal hemoglobin with the level of 12.8g/dl. We arranged a trans-vaginal contrast-enhanced ultrasound. The result showed a strong echo with a size of 4.9x5.0x4.8cm3 was localized in the myometrium of the left uterine corner (Figure 2).
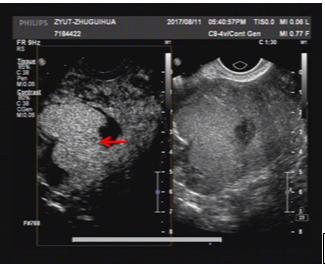
had only serous membrane left. The result suggested intramural lesion and AVF. Magnetic Resonance Imaging (MRI) was clearer to exhibit the character of the lesion (Figure 3).
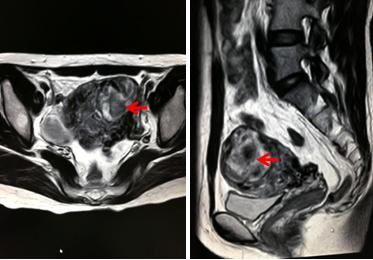
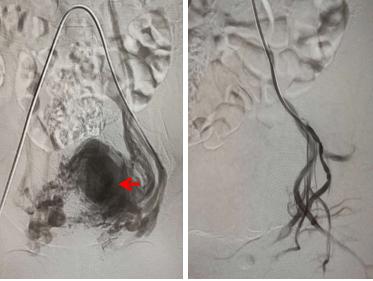
It showed the lesion was localized at the left corner and extended to adjacent part, convex to the left fundus, the left anterior and the left posterior of the uterus. Only serous membrane can be seen, the muscle layer was almost completely eroded. The mass was separated from the cavity. The entire affected region had enlarged and distorted vessels. MRI either suggested intramural lesion and AVF. A mass with a size about 4cm in diameter was Because of the high blood-flow in the mass, we arranged artery embolization firstly. Magnetic Resonance Angiography (MRA) before embolization showed malformed vessels on the left half of the uterus (Figure 4).
found on the right adnexa either by ultrasonography or MRI.
Surgical Technique
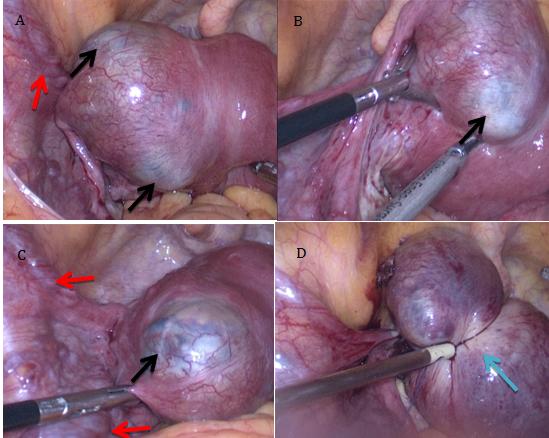
Transcatheter embolization (TAE) of the left internal iliac artery was performed and we can find the blood flow decreased dramatically. 24 hours later, we performed hysteroscopy and laparoscopy. During hysteroscopy, we found mild intrauterine adhesion located in the left corner. We separated adhesion, and then found the left corner was obviously deeper than the right. No AVM or pregnant tissue was found in the uterine cavity. In laparoscopy, we found the uterus was larger than the normal and was with a size of 50days as pregnancy. The left portion of the uterus was blue colored, enlarged and convex to the serous membrane, which formed a mass of 6x6x6cm3 in size (Figure 5).
Discussion
Uterine arteriovenous malformation (AVM) is a rare condition in gynecology, which potentially leads to fatal vaginal or intraperitoneal bleeding. Dunreuil and Loubat firstly reported it in 1926. It consists of proliferation of arterial and venous channels with fistula formation and a mixture of capillary-like vessels. Uterine AVM can be divided into two types, one is congenital and the other is acquired. Congenital AVM result from a defect in the differentiation of the primitive capillary plexus during fetal angiogenesis, while acquired AVM is usually resulted from uterine trauma, surgical intervention, or in the setting of a preexisting pathologic uterine process. Case reports have described acquired AVM formation following uterine dilation and curettage (D&C), cesarean section, and hysteromyomectomy [4, 5]. Pathologic processes including infection, trophoblastic disease, and malignancies have been also described to be associated with acquired AVM [6]. AVF is different from AVM. The later is characterized by a nidus of poorly differentiated blood vessels connecting the arterial and venous system. The exact incidence of either AVM or AVF is unknown. What we can look up are case reports. The main symptom is unexplained vaginal bleeding. While for our patient, the symptom was low abdominal pain. The reason may be due to the location of the lesion, for it was convex to the serous membrane of the uterus. We assumed it was an acquired AVF for our patient, which characterized by multiple direct connections of the artery and vein without intervening capillary. The patient had 5 times of pregnancy and four times of induced abortion. For every time she received ultrasonography to conform pregnancy and either received the examination to ensure no residual tissue after terminating pregnancy. She denied abnormal finding before the last pregnancy. During the treatment, we performed hysteroscopy firstly and found the left corner of uterine cavity was obviously deeper than the right. It was thought that an incomplete uterine perfusion occurred during the last D&C. Then we performed laparoscopy and found a huge blue mass on the left corner of the uterus, the mass involved almost half of the uterus. Pathological result verified residual pregnant tissue within the mass. The serous membrane was so weak, it was broken when we touched it gently. Fortunately, we dealt with the patient timely to avoid lethal intraperitoneal hemorrhage. Diagnosing AVM or AVF rely on imaging examination. Color Doppler ultrasonography is the preferred choice. Specific characters of the tangle of vessels as serpiginous/tubular anechoic structures within the myometrium with a low-resistance and high-velocity flow pattern can be found [7]. Nevertheless, pelvic angiography remains the gold standard for the diagnosis. For our patient, we ranged Color Doppler ultrasonography, transvaginal contrast-enhanced ultrasonography and MRI successively with the aim of choosing the most appropriate regimen [8]. There is no standard criterion for treating AVM. It should be personalized and mainly depends on patients’ hemodynamic status, age, desire for future fertility. Calzolari, et al. [9] reported that hysteroscopy was a feasible and safe alternative treatment modality for AVM. Their selected patients were stable hemodynamics and presented with mild symptoms. The lesion was located in the uterine cavity or adjacent muscular layer. Our patient also had stable hemodynamics without vaginal or intraperitoneal bleeding, but the focus was located in the out layer of the uterus with an almost ruptured serous membrane. Hysteroscopy found no lesion in the cavity. Because the mass was so large and the blood-flow was so high, we arranged internal iliac artery embolization before surgery with the aim to control intraoperative bleeding. The total bleeding amount was no more than 40ml during the operation. We have given her a timely treatment to avoid serious outcome and preserved her uterus. We should bear in mind that both congenital and acquired AVM have a high propensity to bleed given the inability of these arterivenous connections to withstand high blood flow and elevated pressure, and appropriate consideration must be given before surgical intervention [10]. The mean age of the patients with AVM is 33.5 years old [2], so fertility-preserving is important for these childbearing-age patients. Historically, laparotomy hysterectomy was the main treatment for AVM. This kind of surgery cannot keep the fertility function for young patients. As the emerging and advancing of trans-catheter embolization, minimally invasive surgical approaches such as laparoscopy and hysteroscopy are rapidly becoming the main treatment modalities. Small hurts, little bleeding, light pain and come back quickly are all the advantages. It was reported that trans- catheter embolization had a primary success rate of 61% and secondary success rate of 91% after repeated embolization [2]. However, hysterectomy is an appropriate alteration when these conservative methods have failed to prevent a life-threatening hemorrhage, also it is indicated for those women who do not desire fertility- sparing and those who have limited access to medical facilities [11]. Differential diagnosis should be considered. Gestational trophoblastic neoplasm (GTN) cannot be ruled out before surgery as the patient had an incomplete history of induced abortion 3 months before this onset. 8.9mIU/ml β-HCG level cannot suggest that it was not associated with GTT, especially placental site trophoblastic tumor (PSTT). PSTT produces less β-hCG and usually presents with abnormal vaginal bleeding. It can arise after any type of pregnancy. For patients with suspected GTN foci confined to uterus, resection under laparoscopy are feasible and are an important method for diagnose and differential diagnose [12]. Another disease should be differentiated is intramural pregnancy. Intramural pregnancy is one of the rare types of ectopic pregnancy. It refers to a unterine conceptus within the myometrium, without the connection with the fallopian tubes or endometrial cavity. It accounts for less than 1% of all ectopic pregnancy and the incidence is increasing in recent years [13]. The cause of intramural pregnancy is unclear, and the possible risk factors include a prior uterine trauma, adenomyosis, pelvic surgery, and in vitro fertilization [14]. The clinical symptom of intramural pregnancy is nonspecific. The complaints can be vaginal bleeding and/or mild abdominal pain. It is a very rare condition and the diagnosis is difficult to be made due to its nonspecific symptoms and signs. We could not rule out this kind of disease before surgery.
References
-
Lowe LH, Marchant TC, Rivard DC (2012) Vascular malformations: classification and terminology the radiologist needs to know. Semin Roentgenol 47(2): 106-117.
-
Yoon DJ, Jones M, Taani JA, Buhimschi C, Dowell JD (2016) A systematic review of acquired uterine arteriovenous malformations: pathophysiology, diagnosis, and transcatheter treatment. AJP Rep 6(1): e6-e14.
-
Cura M, Martinez N, Cura A (2009) Ateriovenous malformation of the uterus. Acta Radiol 50(7): 823- 829.
-
Przybojewski SJ, Sadler DJ (2011) Novel image- guided management of a uterine arteriovenous malformation. Cardiovasc Intervent Radiol 34(2): S161–S166.
-
Takeda A, Koyama K, Imoto S, Mori M, Sakai K, et al. (2009) Progressive formation of uterine arteriovenous fistula after lapa- roscopic-assisted myomectomy. Arch Gynecol Obstet 280(4): 663-667.
-
Grivell RM, Reid KM, Mellor A (2005) Uterine arteriovenous malformations: a review of the current literature. Obstet Gynecol Surv 60(11): 761-767. minimally invasive management of intramural pregnancy. J Minim Invasive Gynecol 20(1): 123-126.
-
O'brien P, Neyastani A, Buckley AR, Chang SD, Legiehn GM (2006) Uterine arteriovenous malformations: from diagnosis to treatment. J Ultrasound Med 25(11): 1387e92.
-
Fleming H, Ostor AG, Picket H, Fortune DW (1989) Arteriovenous malformation of the uterus. Obstet Gynecol 73: 209e14.
-
S Calzolari, Cozzolino M, Castellacci E (2017) Hysteroscopic management of uterine arteriovenous malformation. JSLS 21(2): e2016.00109.
-
Brown JV III, Asrat T, Epstein HD (2008) Contemporary diagnosis and management of a uterine arteriovenous malformation. Obstet Gynecol 112(2): 467-470.
-
Bagga R, Verma P, Aggarwal N (2008) Failed angiographic embolization in uterine arteriovenous malformation: a case report and review of the literature. Medscape J Med 10(1): 12.
-
Seckl MJ, Sebire NJ, Fisher RA, Golfier F, Massuger L, et al. (2013) Gestational trophoblastic disease: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology 24(6): 39-50.
-
Glass T, Smith P, Hodges R, Holmes HJ (2010) Intramural pregnancy presenting in a patient with tuberous sclerosis. J Clin Ultrasound 38(7): 393-396.
-
Wu PJ, Han CM, Wang CJ (2013) Early detection and
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’