Outcome of Induction of Labour in a Tertiary Hospital, North Western Nigeria
Background: Induction of labour is a well-known procedure performed to artificially initiate uterine contraction in the interest of the mother, the fetus, or both in order to achieve vaginal delivery. Objectives: The aim of this study is to determine the incidence, indications and outcome of induction of labour in a tertiary health institution in North-West Nigeria. Materials and Method: This is a prospective cross sectional study carried out on the patients undergoing induction of labour in the main labour room of the UDUTH, Sokoto between January, 2016 and December, 2016 Results: During the period of study, there were 3112 deliveries out of which 111 had induction of labour. The incidence of labour induction is therefore 3.6%. The most common indications were postdated/post term pregnancies 51 (46.0%), followed by hypertensive disorders of pregnancy 43(38.7%), and pre-labour rupture of membranes 14(12.6%). Majority of the women 91.0% (101/111) had cervical ripening with Misoprostol, while induction of labour was achieved with Oxytocin infusion combined with artificial rupture of membrane in 71 (64.0%). The mean induction delivery interval was 11.5 (SD 11.6) hours. The study did not demonstrate any statistically significant difference between the methods of IOL and induction delivery interval (n=86, P= 0.531, F=0.638). Majority 78 (70.3%) had spontaneous vaginal delivery, 8 (7.2%) had assisted vaginal delivery, while 25 (22.5%) had emergency Caesarean section. The fifth minute mean Apgar score was 8.1±2.5. The fetal outcome was better among the women who had combination of artificial rupture of membranes (ARM) and oxytocin infusion compared to those who had misoprostol (p-value=005). There were 6 (5.4%) perinatal and one maternal death, thus giving a case fatality rate of 0.9%. The maternal complications observed were primary postpartum haemorrhage 10 (9%) and ante partum haemorrhage 6 (5.4%). Conclusion: The main indications for labour induction in this study were postdated pregnancy and hypertensive diseases. Labour induction was achieved mostly with intravaginal misoprostol and a combination of ARM and oxytocin infusion. Majority of cases resulted in spontaneous vaginal delivery and good fetal outcome.
Introduction
Induction of labour (IOL) is an important intervention in obstetrics. It becomes necessary when the risk of continuing the pregnancy far outweighs the risk of intervention [1, 2]. Induction of labour can be defined as artificial initiation of labour after the 28th week of gestation for the purpose of achieving vaginal delivery in situations where the continuation of pregnancy may not be favorable to the mother, baby and/or both [1]. Careful selection of patients is critical for labour induction to succeed as failure means a resort to caesarean section, which tends to contribute to the current increase in the Caesarean section (C/S) rate [3, 4].
The commonly accepted indications for IOL include prolonged pregnancy, intrauterine growth restriction, and hypertensive disorders of pregnancy, Diabetes mellitus, Rhesus iso-immunization, premature rupture of membranes (PROM) and intrauterine fetal death [4, 5, 6]. However, there is evidence for an increase in the frequency of labour induction without any such agreed indications, and this may result into unnecessary Caesarean deliveries [7, 8]. The success of IOL depends largely on state of the cervix [5, 9]. An unfavorable cervix implies that vaginal delivery may not be feasible [10, 11].
Induction of labour after 41 weeks of gestation, is associated with small reduction in perinatal deaths and meconium aspiration syndrome [12, 13]. The World Health Organization (WHO) recommends IOL when there is a clear indication and when expected benefits outweigh potential harms [10]. Induction of labour is sometimes performed for social indications in the absence of medical or obstetric reasons [14]. Similarly, IOL following PROM tends to reduce the incidence of chorioamnionitis, endometritis and neonatal admissions [15].
This study aims to determine the incidence, indications and feto-maternal outcome following labour induction in a tertiary health institution in North-west Nigeria.
Methodology
This is a prospective cross sectional study conducted on the patients undergoing induction of labour in the main labour ward of the UDUTH, Sokoto between 1st January 2016 and 31st December, 2016. A proforma was designed to obtain information on the socio-demographic characteristics of the patients, indications for labour induction, the Bishop’s score, the induction-delivery interval, methods of induction, mode of delivery, indications for caesarean section (C/S), neonatal and maternal outcomes. All women presenting for induction of labour during the study period were included. Ethical clearance was obtained from the Committee on Ethics and Research of the Usmanu Danfodiyo University Teaching Hospital (UDUTH), Sokoto. Informed written and verbal consents were obtained from the patients. Data was analyzed using SPSS version 20.0 for windows. Categorical variables were presented using proportions and percentages and quantitative variables were summarized using mean and standard deviations. Differences in proportions between categorical variables was examined using chi-square test, while mean difference were compared using independent sample t- test. Significant level is set as P < 0.05.
Results
During the period of study, there were 3112 deliveries out of which 111 had induction of labour for various reasons. The rate of labour induction is therefore 3.6%. Table 1 below shows the socio-demographic characteristics of the women who had induction of labour at UDUTH. Their ages ranged from 16 years to 40 years with a mean of 26.7 (SD 6.4 years). Majority 40/111 (36.0%) were between 25 and 29 years. Fifty four (48.6%) of the women were primigravidae, 51(45.9%) were multiparous, while 6(5.4%) were grandmultiparous. Most of the women, 86(77.5%) belonged to the Hausa/Fulani ethnic group. Majority of them 57(51.4%) attained tertiary level of education. About seventy-two (64.9%) of the women were homemakers while the remaining 39(35.1%) were civil servants.
| Frequency | Percentages | |||||||
|---|---|---|---|---|---|---|---|---|
| Variables | ||||||||
| (N = 111) | (%) | |||||||
| Age (years) | ||||||||
| ≤19 | 18 | 16.2 | ||||||
| 20-24 | 25 | 22.5 | ||||||
| 25-29 | 40 | 36 | ||||||
| 30-34 | 16 | 14.4 | ||||||
| ≥35 | 12 | 10.8 | ||||||
| Total | 111 | 100 | ||||||
| Parity | ||||||||
| Primigravidae (0) | 54 | 48.6 | ||||||
| Multigravidae (1-4) | 51 | 45.9 | ||||||
| Grandmultiparae (≥ 5) | 6 | 5.4 | ||||||
| Total | 111 | 100 | ||||||
| Educational Status | ||||||||
| Nil | 4 | 3.6 | ||||||
| Primary | 3 | 2.7 | ||||||
| Secondary | 47 | 42.3 | ||||||
| Tertiary | 57 | 51.4 | ||||||
| Total | 111 | 100 | ||||||
| Occupation | ||||||||
| Home makers | 72 | 64.9 | ||||||
| Civil servant | 39 | 35.1 | ||||||
| Total | 111 | 100 | ||||||
| Tribe | ||||||||
| Hausa/Fulani | 86 | 77.5 | ||||||
| Igbo | 12 | 10.8 | ||||||
| Yoruba | 6 | 5.4 | ||||||
| Others | 7 | 6.3 | ||||||
| Total | 111 | 100 |
Table 2: Gestational age at induction of labour.
- Indications
- Frequency Percentage
- Postdated/Prolonged pregnancy
- 51
- 46
- Hypertensive disorder of pregnancy
- 43
- 38.7
- PROM
- 14
- 12.6
- Others*
- 3
- 2.7
- Total
- 111
- 100
Table 1: Indications of induction.
Majority of the women 80(72.1%) were induced at term, 9(8.1%) before term while 22(19.8%) women had labour induction after 42 weeks as shown in Table 3.
| Gestational Age | Frequency (no) | Percentage (%) | ||||||
|---|---|---|---|---|---|---|---|---|
| Preterm | 9 | 8.1 | ||||||
| Post Term | 22 | 19.8 | ||||||
| Post term | 80 | 72.1 |
Table 3: Gestational age at induction of labour.
Table 4 below shows the events in labour and pregnancy outcome. The most common method for cervical ripening among the study group was with Misoprostol 101(91.0%), while 6(5.4%) women had cervical ripening with Foley’s catheter. Thereafter 72 (64.86%) had induction of labour with artificial rupture of membrane (ARM) followed by an Oxytocin infusion, while 39(35.13%) who had cervical ripening with Misoprostol progressed into labour after ARM.
| Method of cervical ripening | ||
|---|---|---|
| Misoprostol | 101 | 91 |
| Foley’s catheter | 6 | 5.4 |
| Favourable cervix | 4 | 3.6 |
| Method of induction of labour | ||
| ARM + Oxytocin | 72 | 64.86 |
| Misoprostol + ARM | 39 | 35.14 |
| Mode of delivery | ||
| Vaginal Delivery | 86 | 77.5 |
| Caesarean Section | 25 | 22.5 |
| Total | 111 | 100 |
| Reasons for CS (n= 25) | ||
| Failed induction | 14 | 56 |
| Fetal distress | 7 | 28 |
| Cervical dystocia | 4 | 16 |
| Total | 25 | 100 |
Table 4: Events in labour and pregnancy outcome.
Most 64(74.4%) of the women were delivered within 12 hours of commencement of induction of labour. Majority 86(77.4%) of the women had vaginal delivery while 25(22.5%) had emergency Caesarean section (Table 5). The leading indication for the Caesarean sections in the study was failed induction 14(56%). However from this study there is no statistically significant difference between the methods of IOL and induction delivery interval (n=111, P= 0.064, X2=3.426). There was no statistical association or significant difference between mode of delivery and the method of IOL with pvalue = 0.072, X2= 3.243 this is shown in table 6
| Induction delivery | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Statistics | |||||||||
| Method of IOL | interval | ||||||||
| ≤12 Hours | >12 hours | P value = .064 | |||||||
| ARM + Oxytocin | 34 | 17 | X2= 3.426 | ||||||
| Misoprostol only | 28 | 5 | Df =1 |
Table 6: Association between Induction delivery interval and methods of IOL.
| Mode of delivery | Statistics | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Method of IOL | |||||||||
| Vaginal | CS | Pvalue = .072 | |||||||
| ARM + Oxytocin | 52 | 20 | X2= 3.243 | ||||||
| Misoprostol only | 34 | 5 | Df=1 |
Table 7: Association between Method of IOL and Mode of delivery.
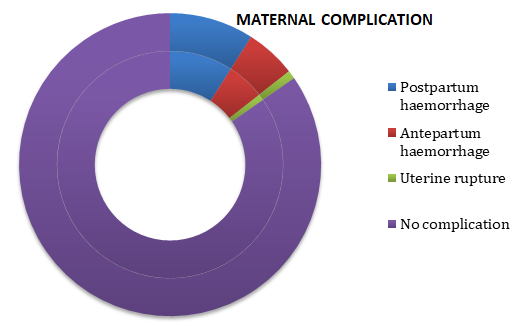
The maternal complications encountered were primary post-partum haemorrhage 10(9.0%), antepartum haemorrhage (Abruptio placentae) 6(5.4%) and uterine rupture 1(0.9%) (Figure 1).
The mean estimated fetal weight was 3.4±0.3kg, while the mean fetal weight at delivery was 3.0±0.5kg. From the study the first minute mean Apgar score was 6.8±2.4 while the fifth minute means Apgar score was 8.1±2.5. Among the babies delivered, 100(90%) had normal Apgar scores of 7 and above while 8(7.2%) of the babies had severe birth asphyxia. This is shown in the table below. The mean Apgar scores are better among the women who had combination of ARM and oxytocin infusion compare to women following cervical ripening with Misoprostol. (df=2, X2=22.54 , P<0.000). This is shown in table 7.
| 5th Minute Apgar group | ||||||||
|---|---|---|---|---|---|---|---|---|
| Method of IOL | ||||||||
| <=3 | 4-6 | >=7 | P value = .000 | |||||
| ARM + Oxytocin | 0 | 0 | 72 | X2= 22.543 | ||||
| Misoprostol only | 8 | 3 | 28 | Df=2 |
Table 5: Fetal outcome Following Induction of labour.
Discussion
The IOL rate of 3.6% found in this study is lower than the 6.6% and 6.5% that were reported from Maiduguri in the North-eastern and Bayelsa of Niger Delta regions of Nigeria respectively [7, 16]. However it is slightly higher than 2.35% observed in Kano and closer to 3% that was previously reported from this centre [17, 18]. These figures are low compared to reports from developed countries where rates of induction of labour of up to 20% have been documented [19]. The reasons for the low figures reported from the developing countries could be the fear that failed induction of labour may result to Caesarean section of which there is a strong aversion [20]. Similarly, many patients believe that the pain of oxytocin infusion is more than that of spontaneous uterine contraction, hence the resistance to IOL even when it is medically indicated [20].
The most common indications for IOL in this study were; postdated/prolonged pregnancy 51(46.0.8%) hypertensive disorders in pregnancy 43(38.7%), and PROM 14(12.6%). This is similar to some studies from other centres in Nigeria [18, 19, 20, 21, 22, 23]. Induction of labour after 40 weeks of gestation is justified to reduce perinatal mortality, which increases after this period due to the reduction in the function of an aging placenta. Most of the indications for labour inductions are medical there were no case of induction of labour for social reasons in our centre. However, IOL on social indications accounts for up to 5-10% of cases particularly in some industrialized nations [22].
The most common method of induction of labour in this study was by combination of artificial rupture of membrane and Oxytocin infusion but in 18.0% of the women who had cervical ripening with misoprostol needed only artificial rupture of membrane to go into active phase of labour. However there from this study there is no statistical significant difference between the different methods of induction and fetal outcome. Reports from some centres in Nigeria and other African countries showed a preference to Misoprostol as the most common method of induction of labour [7, 16, 19, 20, 23]. The choice of Oxytocin infusion method in our centre may be due to the high proportion of multiparous subjects that present for IOL with some risk factors for uterine rupture. Conversely, a significant number of our patients (15.3%) who had cervical ripening with Misoprostol went into active phase of labour without requiring further oxytocin infusion for induction.
Our study revealed that the majority (74.4%) of the women were delivered within 12 hours of commencement of IOL. This was similar to what was reported in some other studies [7, 17, 23, 24]. The 12 hours induction delivery-interval may be considered as an advantage since it reduces congestions in both the labour and lying in-wards. It also reduces the length of stay in the hospital for the patients and their families. However from this study there is no statistically significant difference between the methods of IOL and induction delivery interval.
The overall success rate for labour induction in this study was 77.5%. This is lower than the 85% and 90.4% reported from the Bayelsa and Benin City respectively [7, 24]. However it is similar to the 82% success reported from previous study in this institution and 83.5% from Kano [17, 18]. This differences might be due to the fact that while the study from Benin City was limited to term pregnancies, this study was unselective in terms of gestational age.
In this study, 22.5% of our subjects had Caesarean section when labour induction was unsuccessful. A similar figure was reported from the Kano and Bayelsa studies but a higher CS rate of 53.6% has been reported in another study [7, 18, 25]. The other reasons for the failure to achieve vaginal delivery in these patients included fetal distress and cervical dystocia. Caesarean section therefore becomes the inevitable option under these conditions. There is therefore need for proper and adequate counseling before commencement of IOL.
This study showed that most of the neonates (88.3%) had good Apgar scores of 8 and above while 8(7.2%) of the neonates had severe birth asphyxia. The mean 5th minute APGAR Score was 8.1±2.5 which is comparable to findings from other studies [7, 16, 23]. However from this study the mean Apgar scores were better among the women who had combination of ARM and oxytocin infusion compared to those who had ARM only following cervical ripening with Misoprostol.
The maternal complications encountered in this study included primary post-partum haemorrhage, antepartum haemorrhage and uterine rupture. These complications were also reported in some studies [7, 17, 23]. There was only one maternal death, which was due to uterine rupture thus giving a case fatality rate of 0.9%. Though IOL is not without risks, the lone maternal death m recorded in this study further reinforces the safety of the procedure when there is a clear indication [7, 17, 18].
Conclusion
The main indications for labour induction in this study were postdated pregnancy and hypertensive diseases. Labour induction was achieved mostly with intravaginal misoprostol and a combination of ARM and oxytocin infusion. Majority of cases resulted in spontaneous vaginal delivery and good fetal outcome. The rate of labour induction was slightly higher compared to other studies.
References
-
WHO (2011) Recommendations for induction of labour. World Health Organization, Geneva.
-
Royal College of Obstetricians & Gynaecologists (RCOG) (2012) Induction of labour RCOG, London.
-
Thorsell M, Lyrenäs S, Andolf E, Kaijser M (2011) Induction of labour and risk for emergency Caesarean section in nulliparous and multiparous women. Acta Obstet Gynaecol 90(10): 1094-1099.
-
Rattigen MI, Afkinso AL, Baum JD (2013) Delivery routes following elective induction of labour at term: Analysis of 807 patients. J Atin Med Res & Elmer press 5(4): 305-308.
-
ACOG Committee on Practice Bulletins-Obstetrics (2009) ACOG practice Bulletin No. 107: induction of labour. Obstet & Gynaecol 114(2): 386-397.
-
Ekele BA, Nnadi DC, Gana MA, Shehu CE, Ahmed Y, et al. (2007) Misoprostol use for cervical ripening and induction of labour in a Nigerian Teaching Hospital. Nig J Clin Pract 10(3): 234-237.
-
Ayuba II, Abhulimen O, Ekine AA (2012) Safety of induction of labour in the Niger Delta Region. Nig Grener J Med Sci 2(2): 173-178.
-
Moore LE, Rayburn WF (2006) Elective induction of labour. Clin Obstet Gynaecol 49(3): 698-704.
-
Mealing NM, Roberts CL, Ford JB, Simpson JM, Morris JM (2009) Trends in induction of labour 1998-2007 a population based study. ANZJOG 49(6): 599-605.
-
Vogel JP, Paulosouza J, Gulmezoghi AM (2013) Pattern and outcome of induction of labour in Africa and Asia: A secondary analysis of the WHO global survey on maternal and neonatal Health. PLoS One 8(6): 65612.
-
Sanchez Z, Ramos L (2005) Induction of labour. Obstet Gynaecol Clin Am 32(2): 181-200.
-
Brindley BA, Sokol RJ (1998) Induction and augmentation of labour: Basis and methods for current practice. Obstet Gynaecol Surv 43(12): 730- 743.
-
Gülmezoglu AM, Crowther CA, Middleton P, Heatley E (2012) Induction of labour for improving birth outcome for women at or beyond term. Cochrane 06 Syst Rev 6: CD04945.
-
Lawani OL, Onyebuchi AK, Iyoke CA, Okafo CN, Ajah LO (2014) Obstetric outcome and significance of labour induction in a health resource poor setting. Int J Obstet Gynaecol 2014: 419621.
-
Mozurkewich E, Chilimigras J (2009) Indication for induction of labour: a best evidence review. BJOG 11(5): 626-636.
-
Bako BG, Obed JT, Sanusi I (2008) Methods of induction of labour at UMTH, Maiduguri, a 4 year review. Nig J Med 17(2): 139-142.
-
Ekele BA, Oyetunji JA (2002) Induction of at Usmanu DanFodiyo University Teaching Hospital. Trop J Obst Gynaecol 19(2): 74-77.
-
Aliyu D, Yakassai IA (2013) Comparing the outcomes of labour induction with Misoprostol and Dinoprostone at Aminu Kano Teaching Hospital. Trop J Obstet Gynaecol 30(1).
-
Malande B, Moodley J, Kambarau SR (2014) Induction of labour at a regional hospital in Kwazulu-Natal South Africa. SAJOG 20(1).
-
Mac Dorman MF, Mathew TJ, Marthin JA, Malloy MH (2002) Trench and Characteristics of induced labour in the United States, 1989-1998. Paed Perinat Epidermiol 16(3): 263-273.
-
Mbele AM, Makin JD, Pathson RC (2007) Can the outcome of induction of labour with oral Misoprostol be predicted? S Afr Med J 97(4): 289-292.
-
Buisf R (1999) Induction of labour: indication and obstetric outcome in a tertiary referral hospital. NZ Med J 112(1091): 251-253.
-
Abdul MA, Ibrahim UN, Yusuf MD, Musa H (2007) Efficacy and safety of Misoprostol in induction of labour in a Nigerian tertiary hospital. West Afr J Med 26(3): 213-216.
-
Orhue AAE (1997) Induction of labour. Trop J Obstet Gynaecol 141(1).
-
Ibrahim IA, Jeremiah I (2012) Prevalence and determinant of Caesarean section in Teaching Hospital in the Niger Delta. Afr J Health & Env 18(2): 22-29.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’