Addition of Growth Hormone to the Stimulation Protocol in Poor Responders-An Option for Increasing Pregnancy Rates in Failed IVF Cycles-A Short Communication
Recently Regan, et al. [1] reported response of granulosa cells (GC) receptor density for growth hormone(GH), FSH, Bone morphogenetic protein receptor 1B(BMPR1B), and LH in women of different age groups and ovarian reserve undergoing IVF.
Short Communication
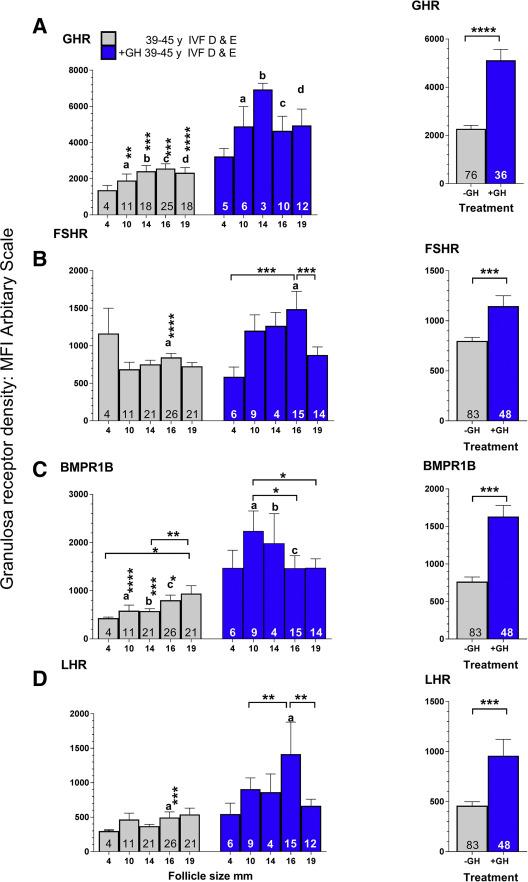
Recently Regan, et al. [1] reported response of granulosa cells (GC) receptor density for growth hormone(GH), FSH, Bone morphogenetic protein receptor 1B(BMPR1B), and LH in women of different age groups and ovarian reserve undergoing IVF. GH receptor density was found to be decreased in poor responders, and that GH receptor density increased with age in normal responders but not in poor responders. Their patients were in age group 39-45years with antral follicle counts (AFC’s) of <=8.GH therapy improved density of all 4 receptors. It has been known for over 4 decades that the GH effector, insulin like growth factor 1 (IGF 1) increases the action of FSH on increasing GC estrogen (E2) secretion [2]. The increased density of these GC receptors might partly explain the greater rates of pregnancy rates and delivery reported with the use of GH treatment of women having a low response to ovarian stimulation. This finding was shown in a very small number of individuals, who were not randomized to exposure to GH, though it matches the latest meta-analyses of randomized studies [3].
Further Regan, et al. [1] explained what were statistically significant differences comparing granulosa receptor density among follicles of different sizes, differentiated by female age and AFC. During carrying out Addition of Growth Hormone to the Stimulation Protocol in Poor Responders-An Option for Increasing Pregnancy Rates in Failed IVF Cycles-A Short Communication these comparisons issues concerning multiple testing or correlations among same patients were not considered. The Analysis of variance(ANOVA) approach followed by uncorrected Fischer test, suggested that 1st a global test to see if the discussion of GH receptor density differed between any 2 groups; and 2nd pairwise comparison among all pairs were conducted without penalizing the multiple testing. 8 groups of follicles were there in each figure they described as A-D, for which 28 comparisons were there. Using a p value of p.05 as significant would result in at-least one false positive finding/graph. If standard Bonferroni connection, the significance level needed would be divided by 28=>a p value of 0.002 as statistically significant/graph. With 12 categories in figure G, getting examined to get significance levels it needs to be divided by 66. Secondly accounting for correlations among follicles as if one takes for granted independence of all follicles, might introduce bias, in either direction. Eg are all follicles in group C of figure 1B was from one Patient, how we know that difference of those follicles from normal ovarian reserve was not because of the uniqueness of that patient. If repeated measure analysis is needed to correlate these findings. In the end neither of comparisons is clearly significant, that would invalidate a big chunk of the manuscript that describes and discusses those findings.
J Gynecol
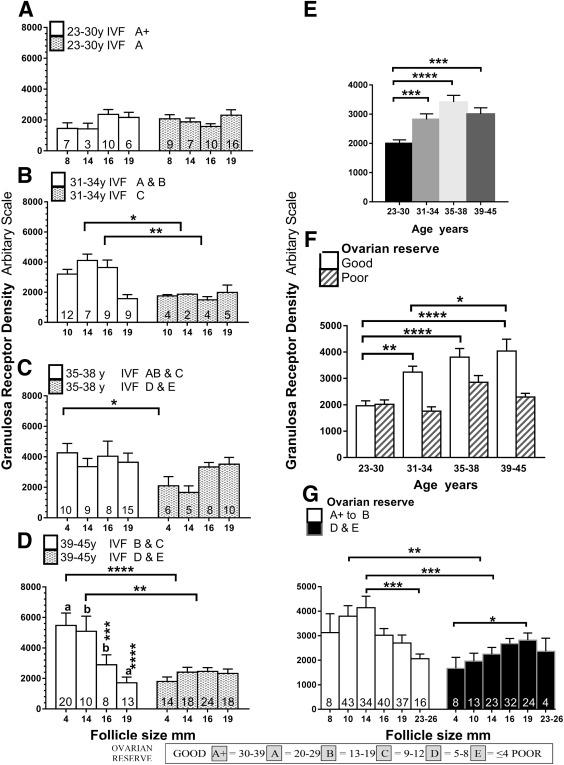
Despite mention of ANOVA in the methods section, the results of this were not given. One is left to presume that ANOVA was likely significant for 1B/A+B versus C,
1D/B+C versus D+E and 1F/and 1G for both groups. But In the absence of these calculations being described it can’t be stated definitely. There are chances that a two Kulvinder Kochar Kaur, et al. Addition of Growth Hormone to the Stimulation Protocol in Poor Responders-An Option for Increasing Pregnancy Rates in Failed IVF Cycles-A Short Communication. J Gynecol 2019, 4(1): 000170.
way ANOVA for the data in figure 1F would confirm the conclusion given by Regan, et al. [1] that GH receptor density was lower in individuals with poor ovarian reserve. Thus author’s confirmation is needed regarding which ANOVA results were significant.
No increase In serum E2 (which reflects GC numbers ,health and response to FSH)in the GH treated patients receiving 10units every alternate day, while a marked and significant increase was noted in Tesarik, et al. [4] study, where a daily 8units GH dose was used.
Unfortunately different studies have used varying dose regimens. Logically it seems following the regimen of Tesarik, et al. [4] would be of benefit, where a dramatic improvement of delivery rate was found in very low prognosis women. Regan, et al. [1] report that giving less Kulvinder Kochar Kaur, et al. Addition of Growth Hormone to the Stimulation Protocol in Poor Responders-An Option for Increasing Pregnancy Rates in Failed IVF Cycles-A Short Communication. J Gynecol 2019, 4(1): 000170.
dose in the final days of follicle maturation or since they had small number of subjects might have affected their results.
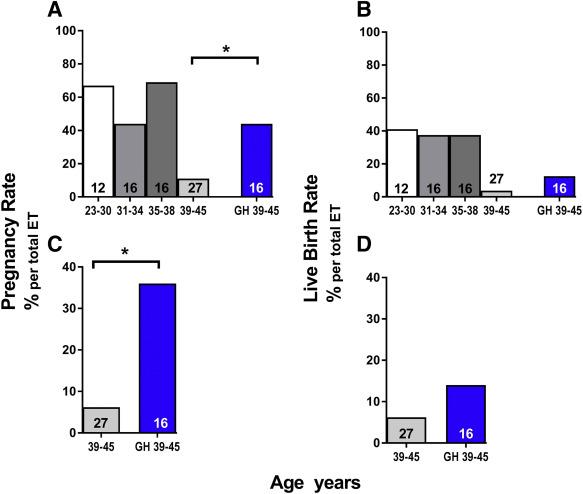
In the most recent meta-analysis carried out by Li, et al. [3] on the use of GH along with gonadotropins in poor responders, with a risk ratio for delivery was 91% greater, with a lower 95% Confidence limit of 29%. With an absolute difference of 13.2% (28%-14.8%), the total number needed to treat was 7.6. The cost for GH being 1500$/patient, total cost of 11,400$/cycle, is very cost effective (at the 14.8% control delivery rate, 6.8 cycles would be needed /delivery, at 15,000 $/cycle reaching a total cost of 102,000$). Even with29% greater delivery rate, GH use remains cost effective, and in countries where costs are lower usually both for GH and IVF. In Tesarik’s study [4], which was a randomized study of very low prognosis women, averaging 42 years, with a mean of approximately 3 failed cycles, the delivery rate increased almost 5 fold.
The question then arises why so much reluctance is there in offering this adjunctive treatment to the most difficult couples? One reason might be “off label’’, although US food and drug administration (FDA) criteria for GH in adults includes GH deficiency. Follicular fluid (FF) GH and IGF 1 concentrations have been reported to be significantly lower in women having IVF who failed to get pregnant and FF IGF1, the effector of GH action, is decreased by one half in poor responders (p<0.0001) [5, 6]. Both IVF success and systemic GH and IGF1 reduced with age. In Tesarik’s [4] study use of GH in women with very low prognosis, treated subjects on controls had Kulvinder Kochar Kaur, et al. Addition of Growth Hormone to the Stimulation Protocol in Poor Responders-An Option for Increasing Pregnancy Rates in Failed IVF Cycles-A Short Communication. J Gynecol 2019, 4(1): 000170.
FFGH levels which were markedly lower in women undergoing IVF who failed to conceive. Using 8units GH/day from D7 of stimulation till oocyte retrieval, FFGH levels increased markedly, but not fully to the levels in their previous study using unselected women who became pregnant [3]. The current study adds to the supporting evidence by giving a mechanism by which improved outcomes can be achieved. Thus these findings suggest that deficiency of GH exists in poor responders, which gives a lower prognosis for women undergoing IVF as does the study by O’bedkova, et al. [7], that puts its use within US federal guidelines. Even otherwise a lot of adjunctive therapies get used in reproductive endocrinology like leuprolide acetate, cabergoline and metformin which are ‘’off label’’ drugs. Use of GH for such a short time, no reported or anticipated risk of DM is there without an actual diagnosis of DM.
Thus basically reason behind underuse of GH is mainly due to conservatism of lot of clinicians of starting any newer approaches of treatment. These doctors need to consider if they would not have incorporated Gn RH agonists how much poorer IVF success rate they would have found. Considering the results of most meta-analysis, that practically doubled delivery rates, what a big loss it is for their poor responders if they remain reluctant to use it.
Further this research stimulates further whether FF deficiency of GH is mainly due to decreased ovarian production or reduced systemic input to the follicle? One major source of GH is pituitary release during sleep. Is it possible that disturbed sleep secondary to anxiety and depression that is common in infertile women, a factor that contributes to this? Hence we need to study is it a significant mediator of the effects of those mental problems that decrease IVF success. If it is follicular in origin, to find the mechanism, so that we can reverse it without any pharmacological intervention.
Thus all practitioners need to be aware how this option might help in those poor responders where all options have failed and give addition of GH in their stimulation protocol to maximize the results.
References
-
Regan SLP, Knight PG, Yovich JL, Arfuso F, Dharmarajan A (2018) Growth hormone during in vitro fertilization in older women modulates the density of receptors in granulosa cells, with improved pregnancy outcomes. Fertil Steril 110(7): 1298-1310.
-
Adashi EY, Resnick CE, D'Ercole AJ, Svoboda ME, Van Wyk JJ (1985) Insulin like growth factors as intraovarian regulators of granulosa cells growth and function. Endocrine Rev 6: 400-420.
-
Li XL, Wang L, Lv F, Huang XM, Wang LP, et al. (2017) The influence of different growth hormone addition protocols to poor ovarian responders on clinical outcomes in controlled ovarian stimulation cycles: A systematic review and meta-analysos. Medicine (Baltimore) 96(12): e6443.
-
Tesarik J, Hazout A, Mendoza C (2005) Improvement of deliver and live birth rates after ICSI in women aged>40years by ovarian costimulation with growth hormoe. Hum Reprod 20(9): 2536-2541.
-
Mendoza C, Ruiz-Requena E, Ortega E, Cremades N, Martinez F, et al. (2005) Follicular fluid markers of developmental potential. Hum Reprod 17(4): 1017- 1022.
-
Bahceci M, Ulug U, Turan E, Akman MA (2007) Comparisons of follicular levels of se Insulin like sex steroids, gonadotropins and Insulin like growth factors (IGF-1)and epidermal growth factor (EGF) in poor responders and norm responder patients undergoing ovarian stimulati0: with GnRH antagonist. Eur J Obster Gynecol 130: 93-98.
-
O’bedkova K, Kogan I, Krikheli I, Dzhem likhanova L, Muller V, et al. (2017) Growth hormone co-treatment in IVF/ICSI cycles in poor responders. Gynaecrinol 33(S1): 15-17. Kulvinder Kochar Kaur, et al. Addition of Growth Hormone to the Stimulation Protocol in Poor Responders-An Option for Increasing Pregnancy Rates in Failed IVF Cycles-A Short Communication. J Gynecol 2019, 4(1): 000170.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’