Association between Progesterone-Only Emergency Contraceptive Pill and Ectopic Pregnancy
Context: Ectopic pregnancy remains a significant cause of morbidity and mortality in the developing countries, where mortality rates are 10 times higher than in the developed countries. In Kenya, there is however no recent data on ectopic pregnancy. Objective: We sought to identify if using an emergency contraceptive pill predisposes to ectopic pregnancy and assess other risk factors for ectopic pregnancy at the Kenyatta National Hospital. Methods: We conducted a case-control study of 120 consecutively sampled women matched for age diagnosed with ectopic pregnancy. Data were analyzed using a statistical package for the social sciences (SPSS software) [version 18.0]. Multivariate logistic regression analysis was performed to calculate the odds ratios (OR) and the corresponding 95% confidence intervals (CI). Results: Of the 120 cases and 120 controls recruited, 27.5% of the cases and 2.5% of the controls had taken Levonogesterol emergency contraceptive (LNG-EC) pill during the menstrual cycle leading to the current pregnancy. Of the cases, 72.7% took the LNG-EC within 24hrs after coitus, while all the controls took the pill within 24-48 hrs. The risk of ectopic pregnancy (EP) increased 12-fold in women who had used LNG-EC (OR=12.44, 95% CI 3.1-49.84) after adjusting for other confounders. EP was associated with an early sexual debut (p= 0.039), and a history of subfertility/infertility (OR=6.87, 95% CI 2.14-22.03). Conclusions: Progesterone only emergency contraceptive pill is as a risk factor for ectopic pregnancy and should be included in the client information leaflet in the drug package insert.
Introduction
Ectopic pregnancy (EP) occurs when the blastocyst implants outside the endometrium of the uterus. More than 95% of ectopic pregnancies occur in the fallopian tube, while the remaining 5 % include cervical, ovarian, and primary abdominal pregnancies [1]. Tubal pregnancies occur in different locations in the tube, with the ampulla region being the commonest site, at 55%, isthmus at 25%, fimbria at 17%, and interstitial at 2% [1]. EP is the leading cause of first-trimester pregnancy-related maternal mortality in the developed world accounting for 4-10% of all maternal deaths in the United States of America [2]. Further, EP complicates 1-2% of all pregnancies [2]. In the developing world and Kenya in particular, unsafe abortion due to unwanted pregnancy is the leading cause of first-trimester maternal mortality [3].
In Kenya, at the Kenyatta National Hospital (KNH) in the year 2002, 5 patients were admitted every week because of EP [4]. EP also has significant implications on future fertility with only a third of patients reported to conceiving after salpingectomy following tubal pregnancy [5, 6]. A study at KNH reported that 5.9% of the patients had suffered repeat ectopic pregnancy [4]. For example, Miyoro et al. demonstrated that 56.6 % of patients treated for EP between 1991- 2000 had features suggestive of pelvic inflammatory disease (PID) [4].
Previous tubal damage from surgery and adhesions secondary to abdominal/pelvic surgery are known risk factors for ectopic pregnancy [1, 7]. Alteration in tubal motility due to certain contraceptive methods predisposes one to EP [7]. The use of progesterone-only contraceptive pills has a slightly increased risk of ectopic pregnancy, with reports of up to 4-6% EP rates [1, 7]. A systematic review published by the American College of Obstetricians and Gynaecologists (ACOG) however did not demonstrate an increased risk among women who had used progesterone- only emergency contraceptive pills reporting an ectopic pregnancy rate of 0.6%- 1.1%, which falls within the reported ectopic pregnancy rates of 0.8%- 2% [8, 9, 10, 11].
Emergency contraceptive (EC), also known as postcoital contraception prevents pregnancy after an unprotected sexual intercourse. Women seeking EC are typically younger than 25 years, have never been pregnant, and have used a form of contraceptive in the past [12]. The methods of emergency contraception available include intrauterine Contraceptive Devices (IUCD), combination Estrogen-Progesterone pills, progesterone-only emergency contraceptive (POEC) pills, and antiprogestins-progesterone receptor antagonists, and selective progesterone receptor modulators. The combination estrogen- progesterone pill also referred to as the YUZPE method consists of two doses of 100mcg ethinyl estradiol and 500mcg of levonorgesterol taken at 12-hour intervals. The POEC pill, marketed as “PLAN B” in the United States of America consists of 750mcg of levonorgesterol taken 12 hours apart. However, the POEC pill taken at 1.5mg at once is as effective as the interval dose and tends to promote adherence [13]. Moreover, LNG-EC reduces the risk of pregnancy following a single act of coitus in mid- cycle from 8% to 1.1 % [8].
Several case reports have been published of women who took the POEC with seemingly no other risk factors and ended up with an ectopic pregnancy [14]. They all recommended that an EP should be considered if menses are delayed after the use of POEC. In addition, to maximize efficacy, EC pills should be started as soon as possible following sexual intercourse. Earlier studies demonstrated that it is effective if started within 72 hours after intercourse [15, 16]. Studies that are more recent have however shown that the pill is effectively taken up to 5 days (120 hours) after intercourse [17, 18, 19]. The Kenya National guidelines for family planning providers has been modified allowing emergency contraception to used up to 120 hours post coitus [20].
In Kenya, there is no recent data on ectopic pregnancy, the last study having been conducted more than 10 years ago. Ectopic pregnancy remains one of the leading causes of morbidity and mortality from attendant complications. Future fertility following an ectopic pregnancy remains low and the risk of a repeat ectopic pregnancy is significant, therefore it is crucial to educate patients on the risk factors and signs of ectopic pregnancy for early intervention. Most of the documented cases of ectopic pregnancy with EC pills are based on case reports. Thus, the overall objective of this study was to determine the association between the use of the hormonal emergency contraceptive pill and ectopic pregnancy.
Methods
Study Design
This was a case-control study, matched for age, the cases being patients with a diagnosis of ectopic pregnancy and the controls being women with an intrauterine pregnancy irrespective of the gestational age. The study was conducted at the Kenyatta National Hospital (KNH) in Nairobi, Kenya.
Inclusion and Exclusion Criteria
Enrollment of patients was carried out in the acute gynecology ward 1D, antenatal clinics, and antenatal wards. Cases included women in the reproductive age admitted with a diagnosis of ectopic pregnancy and consented to participate in the study, while controls were pregnant women visiting a clinic, including those admitted in the antenatal wards, for antenatal care and consented to the study.
We excluded women with a previous ectopic pregnancy, very sick requiring intensive care / Renal Replacement
Therapy, patients who had their operation elsewhere and ere referred to KNH due to complications of ectopic pregnancy, and antenatal mothers who were very sick.
Ethics
This received ethical approval from the KNH-University of Nairobi Ethics and Research Committee (UoN ERC). Permission to conduct the study and access patients’ files was granted by the KNH Head of Department, Reproductive Health, KNH Reproductive Health Research Coordinator and KNH Research, and Programmes Coordinator.
Participants got appropriate health education, and those who required counseling following pregnancy loss were referred to the Patient Support Centre at the KNH.
Data Collection
Statistics
Data were analysed using a statistical package for the social sciences (SPSS) software (version 18.0). Descriptive univariate statistics was use to summarize the socio- demographic characteristics of women with confirmed tubal ectopic pregnancy and women with intrauterine pregnancy. Continuous variables including age were summarized using mean and standard deviation. For continuous variables showing evidence of skewed distribution median, range, and interquartile range were calculated. Categorical variables Age in years Level of formal education Primary 28(23.3) 18(15.1) 1 Secondary 43(35.8) 45(37.8) 0.61(0.30-1.27) 0.188 Tertiary 21(63.6) 1(33.3) 0.55(0.27-1.12) 0.098 Marital status Married 71(59.2) 98(82.4) 1 Single 39(32.5) 13(10.9) 4.14(2.06-8.32) <0.001 Separated 10(8.3) 8(6.7) 1.72(0.65-4.59) 0.275 such as frequency of emergency pill use, dose compliance, and dosing were summarized using univariate frequency distribution tables showing frequencies and percentages of women in each category.
We used bivariate analysis to identify risk factors associated with a tubal pregnancy and those factors associated with intrauterine pregnancy. The categorical risk factors including emergency contraceptive use were cross- tabulated with the type of pregnancy (tubal or intrauterine) and comparisons were done using the chi-square or Fisher’s exact test, as appropriate. T-test was used to compare means of continuous variables in the group with confirmed tubal or intrauterine pregnancy. Finally, logistic regression was used to conduct a multivariable analysis with the binary variable for tubal or intrauterine pregnancy as the outcome (dependent variable) and the risk factors showing significant associations with tubal pregnancy as the independent variables. Statistical significance was based on an alpha level of 0.05.
Results
We recruited 120 women with an index ectopic pregnancy. Each of the 120 cases of ectopic pregnancies were matched for age to control with intrauterine pregnancy (n=120). Adequate age matching was achieved with an average age of 26.9 years (SD 6.2) among cases compared to an average age of 26.7 (SD 6.2) among controls. The most frequent age groups were 25-29 years.
Cases Control OR(95% CI) p-value
<19 years 5(4.2) 5(4.2) 1 20-24 years 30(25.0) 30(25.2) 1.00(0.26-3.81) 1 25-29 years 43(35.8) 42(35.3) 1.02(0.28-3.80) 0.972 30-34 years 31(25.8) 31(26.1) 1.00(0.26-3.80) 1 >=35 years 11(9.2) 11(9.2) 1.00(0.22-4.46) 1
- ˖SD (Standard Deviation); CI (Confidence Interval); OR (Odds Ratio)
Table 1: Demographic characteristics of ectopic pregnancy cases compared to controls.
Table 1 is the risk of ectopic pregnancy was higher in single women. Single women were approximately four times more likely to have an ectopic compared to married women (OR= 4.14, 95% CI 2.06-8.32, p < 0.001).
Obstetric and Gynaecologic History
Forty-four (36.7%) cases reported that the index pregnancy was planned and 72 (60.5%) controls similarly reported that the pregnancy was planned. Among these groups of planned pregnancies, 41 (93.2%) cases and 63 (87.5%) controls indicated that the pregnancies were timely.
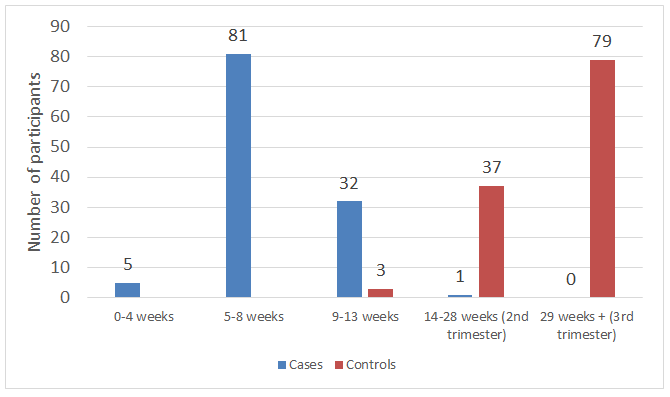
Figure 1 presents the gestational age of pregnancies according to case-control status. The modal gestational age among cases with ectopic pregnancies was 5-8 weeks, 81 (67.5%, 95% CI 58.3% - 75.8%) while among controls with intrauterine pregnancy, the modal gestation age was 29-42 weeks, 79 (65.8%, 95% CI 56.6% - 74.2%).
Cases Control OR (95% CI) p-value Parity
- ˖CI (Confidence Interval); OR (Odds Ratio)
Table 2: Parity: Cases as compared to Controls.
There was a significant association between parity and ectopic pregnancy with women of parity between 1 and 2 having a higher risk of ectopic (OR= 1.84, 95% CI 1.07-3.14, p= 0.027) compared to prim gravid women.
Emergency Contraceptive Pill Use
Used emergency pill in the index menstrual cycle Yes 33(27.5) 3(2.5) 14.71(4.37-49.55) <0.001 Timing of emergency pill use (n = 36) < 24 hours 24(72.7) 0(0.0) NA NA 24-48 hours 7(21.2) 3(100.0) NA 48-72 hours 2(6.1) 0(0.0) NA Do you know your fertile days? Yes 11(9.2) 7(5.9) 1 0.34 No 109(90.8) 112(94.1) 0.62(0.23-1.66) Frequency of emergency pill use in one month preceding index pregnancy
0 41(34.2) 57(47.9) 1 1 to 2 70(58.3) 53(44.5) 1.84(1.07-3.14) 0.027 3 to 4 7(5.8) 6(5.0) 1.62(0.51-5.18) 0.415 >=5 1(0.8) 2(1.7) 0.70(0.06-7.93) 0.77 Cases Control OR (95% CI) p-value No 86(71.7) 115(96.6) 1 Never used 101(84.2) 111(93.3) 1 Once 14(11.7) 6(5.0) 2.56(0.95-6.93) 0.063 Twice 3(2.5) 1(0.8) 3.30(0.34-32.21) 0.305 Three or more times 2(1.7) 1(0.8) 2.20(0.20-24.61) 0.523
- ˖CI (Confidence Interval); OR (Odds Ratio)
- The risk of ectopic pregnancy was 14 times higher in women reporting the use of the emergency pill in the index menstrual cycle compared to women who did not use the emergency pill during the period (OR = 14.71, 95% CI 4.37 –
- 49.55, p < 0.001) (Table 3).
- Among controls, all three women who took the pill reported using it between 24 and 48 hours of coitus, while the majority (72.7%) of the cases used the pill within 24
- Cases
- Control p-value (Fisher’s exact)
- <19 years
- 2(6.1)
- 1(33.3)
- 0.185
- 20-24 years
- 14(42.4)
- 0(0.0)
- 25-29 years
- 8(24.2)
- 1(33.3)
- 30-34 years
- 7(21.2)
- 1(33.3)
- >=35 years
- 2(6.1)
- Age in years
- Level of formal education
- Primary
- 3(9.1)
- 0(0.0)
- 0.428
- Secondary
- 9(27.3)
- 2(66.7)
- Tertiary
- 21(63.7)
- 1(33.3)
- 0
- 17(51.5)
- 1(33.3)
- 0.3
- 1 to 2
- 14(42.4)
- 1(33.3)
- 3 to 4
- 1(3.0)
- 1(33.3)
- 5
- 1(3.0)
- 0(0.0)
- Parity
Table 3: Emergency contraceptive pill use among cases of ectopic pregnancy and controls.
- The characteristics of emergency pill users are presented in Table 4. In the ectopic pregnancy group, 42.4% of emergency pill users were aged between 20 and 24 years while among the three users with intrauterine pregnancies, a single participant was found in each of the following age
- Cases
- Control p-value (Fisher’s exact)
- Knowledge of fertile days
- Yes
- 6(18.2)
- 1(33.3)
- 0.488
- No
- 27(81.8)
- 2(66.7)
- Emergency pills swallowed
- Both at once
- 26(78.8)
- 3(100.0)
- 1
- Swallowed at Interval
- 7(21.2)
- 0(0.0)
- Instructed how to take drugs
- Yes
- 11(33.3)
- 3(100.0)
- 0.051
- No
- 22(66.7)
- 0(0.0)
- Emergency pill use in the preceding month
- Not used
- 22(66.7)
- 2(66.7)
- 1
- Used at least once
- 11(33.3)
- 1(33.3)
- Follicular
- 4(12.1)
- 1(33.3)
- 0.603
- Ovulatory
- 4(12.1)
- 0(0.0)
- Secretory
- 24(72.7)
- 2(66.7)
- The phase of the cycle during which the pill was taken
- < 24 hours
- 24(72.7)
- 0(0.0)
- 0.034
- 24-48 hours
- 7(21.2)
- 3(100.0)
- 48-72 hours
- 2(6.1)
- 0(0.0)
- The duration between coitus and taking a pill
Table 4: Knowledge and administration of oral emergency contraceptives in emergency pill users.
Table 5 shows the level of knowledge of emergency pill users according to case-control status. Six (18.2%) cases and 1 (33.3%) control knew the fertile days; 33.3% and all three controls were given instructions on how to take pills and 78.8% of cases and all three controls swallowed both pills at once. Two-thirds of cases (66.7%) and two of the controls reported having taken emergency pills in the preceding Age at sexual debut History of inability to conceive (> 6 months after discontinuing contraceptive) No 94(78.3) 112(94.1) 1 Long-term contraception (1 year before conception) month. Twenty-four (72.7%) controls took the pill within 24 hours of coitus and the three controls took the pill between 24 and 48 hours after coitus. Most women in both groups (n = 24 cases, n = 3 controls) took the emergency pill during the secretory phase of the menstrual cycle. All the study participants who took the emergency pill (n=33 cases, n= 3 controls) obtained the pill from a chemist.
Cases Control OR (95% CI) p-value <15 years 9(7.5) 2(1.7) 7.87(1.10-56.12) 0.039
16-19 years 69(57.5) 60(50.4) 2.01(0.56-7.21) 0.283
20-24 years 38(31.7) 50(42.0) 1.33(0.36-4.87) 0.667
>=25 years 4(3.3) 7(5.9) 1 Yes 21(17.5) 5(4.2) 5.00(1.82-13.78) 0.002
None 82(68.3) 80(67.2) 1
Pills 20(16.7) 13(10.9) 1.50(0.70-3.22) 0.297
IUCD 3(2.5) 4(3.4) 0.73(0.16-3.37) 0.689
Implant 3(2.5) 7(5.9) 0.42(0.10-1.67) 0.218
Injectable 12(10.0) 14(11.8) 0.84(0.36-1.92) 0.673
Timely pregnancy Yes 41(34.2) 63(52.9) 1
No 79(65.8) 56(47.1) 2.17(1.29-3.65) 0.004
- ˖SD (Standard Deviation); CI (Confidence Interval); OR (Odds Ratio)
Table 5: Other risk factors associated with ectopic pregnancy.
Other risk factors for ectopic pregnancy not related to emergency pill use were analyzed and are presented in Table 6. Among these risk factors, ectopic pregnancy was significantly associated with: early sexual debut (p = 0.039), history of inability to conceive immediately after discontinuing contraception (p = 0.002), unplanned (p < History of pelvic surgery Yes 20(16.7) 27(22.7) 1 Previous treatment for STI Yes 30(25.0) 12(10.1) 3.01(1.45-6.21) 0.003 History of tuboplasty Yes 4(3.3) 2(1.7) 1
0.001), and untimely pregnancies (p = 0.004). The risk of ectopic increased 7 times in women reporting sexual debut before 15 years of age compared to debut after 25 years (OR = 7.87, 95% CI 1.10-56.12). Prior history of inability to conceive before the index pregnancy increased the risk of ectopic pregnancy 5 times (OR = 5.0, 95% CI 1.82-13.87).
Cases Control OR (95% CI) p-value No 100(83.3) 92(77.3) 1.47(0.77-2.79) 0.243
No 89(74.2) 107(89.9) 1
No 116(96.7) 116(97.5) 0.50(0.09-2.78) 0.429
- ˖SD (Standard Deviation); CI (Confidence Interval); OR (Odds Ratio)
Table 6: Reproductive health treatment interventions in ectopic pregnancy cases and controls.
The impact of various reproductive health treatment interventions on the risk of ectopic pregnancy is presented in Table 7. Previous STI treatment was significantly associated with ectopic pregnancy risk (p = 0.003), but the history of pelvic surgery (p = 0.243) and tuboplasty (p = 0.429) was not associated with ectopic pregnancy. The risk of ectopic pregnancy increased threefold in women who had previously received STI treatment (OR = 3.01, 95% CI 1.45-6.21).
Odds Ratio p-value 95% CI
Married 1
Marital status
Single 4.53 0.004 1.6 12.6
Other 0.76 0.676 0.2 2.8
Primary 1
Level of education
Secondary 0.44 0.09 0.2 1.14
College 0.41 0.089 0.2 1.15
University 1.05 0.942 0.3 4.01
Primigravid 1
Parity
Risk factors associated with EP
Para 1-2 3.85 0.001 1.7 8.67
Para 3-4 1.99 0.363 0.5 8.83
Para 5 and above 0.23 0.474 0 13.2
History of use of the emergency pill in the index pregnancy 12.44 <0.001 3.1 49.9 Age at sexual debut 0.66 0.124 0.4 1.12 Unplanned pregnancy 1.61 0.539 0.4 7.4 Untimely pregnancy 0.95 0.944 0.2 4.3 Inability to conceive 6.87 0.001 2.1 22 Previous STI treatment 3.09 0.013 1.3 7.48
- ˖SD (Standard Deviation); CI (Confidence Interval); OR (Odds Ratio)
Table 7: Adjusted odds ratio of the risk of ectopic pregnancy from logistic regression.
Multivariable regression analysis was conducted using a logistic regression model to determine the independent predictors of the risk of ectopic pregnancy. The results of the regression analysis are presented in Table 8.
The independent predictors of ectopic pregnancy were: history of emergency pill use in index pregnancy (p < 0.001), inability to conceive after discontinuing contraception (p = 0.001), and previous STI treatment (p = 0.013). After adjusting for the confounding effect of marital status, education level, parity, age at sexual debut, and planning for index pregnancy, the risk of ectopic pregnancy increased 12- fold in women who had used emergency contraception (OR = 12.44, 95% CI 3.10–49.87). The risk of ectopic pregnancy also increase 3 times and 6 times, in women with a history of STI treatment (OR = 3.09, 95% CI 1.27-7.48) and inability to conceive (OR = 6.87, 2.14-22.03), respectively.
Discussion
The objective of this study was to find out if the use of emergency contraceptive pills increases the risk of ectopic pregnancy. A significant association was noted from the study, with 27.5% of patients with EP reporting to have taken LNG-EC in the index menstrual cycle compared to 2.5% of the controls, which gave a twelve-fold increase in the risk of EP if LNG-EC fails. This increase though higher is in keeping with a recently published multicenter case-control study done in China between 2011 and 2013 which reported a three-fold increase in EP after the failure of EC [14]. Farkas, et al. in their study of the effect of oral ovulation inhibition contraceptives and postinor on steroid hormones reported an ectopic pregnancy rate of 6.4% following the failure of LNG-EC [21]. A systematic review by Cleland et al. however showed no increase in the risk of EP after the use of LNG-EC, reporting that the rate of ectopic pregnancy was 0.8%, which falls within the general population rates of 1-2% [2]. Most of the studies used in the systematic review however did not use EP as their endpoint. Two epidemiological studies reported higher rates of EP following the failure of LNG-EC. In Hong Kong in 2008, a failure rate of 1.8% with an ectopic pregnancy rate of 2.8% was reported [22], and Gainer et al. reported an ectopic pregnancy rate of 4.1% after the failure of LNG- EC [23]. There was no statistical significance between ectopic pregnancy and the level of education in this study. A recent study done in China however found that EP occurred more often in women with lower level education compared to those with tertiary education [14]. A study done in Italy did not show any association between education level and the occurrence of EP [24]. In this study, single women were four times more likely to have an EP compared to married women. This is most likely due to the possibility of high-risk sexual behavior and multiple sexual partners among single women. Miyoro found no statistical significance with marital status [4]. A study in China similarly did not show any statistical significance between marital status and the risk of EP [14].
There was a significant association between parity and EP, with women para 1-2 being at a higher risk of EP compared to nulliparous women. From this study, 92.5% of all cases had parity equal to or less than 2, with 34% being nulliparous. This is in keeping with other studies which have reported that most patients with EP tend to be of low parity. Miyoro reported that 77.2% of the cases had parity equal to or less than 2 [4]. Parazzini et al. reported similar association in Italy [24]. The majority (42.4%) of the LNG-EC users was aged 20-24 years, nulliparous (51.5%), and had college- level education (45.5%). This is in keeping with the ACOG practice bulletin report of May 2010 [17], which described EC users as being below 25 years and having never been pregnant. A study was done in Hong Kong between 2006 and 2008 to describe the characteristics of EC users [22], however reported a mean age of 30 years, with 65.5% being nulliparous.
Only 18.2% of the cases who took the pill knew their fertile days. Seventy two percent (72.2%) of the cases took the pill within 24 hours of unprotected coitus and all the 3 controls took the pill within 24-48% hours. The majority of the cases (78.8%) and all the controls swallowed both pills at once and most women (n=24 cases and n=3 controls) swallowed the pill in the secretory phase. From this study therefore, the majority of the women knew the correct timing and dosing of use of LNG-EC and used it correctly compared to a study done among Kenyatta University students by Nyawande, et al. in 2005, where despite significant knowledge of the fertile days (81%), only 52% knew how the correct timing [25]. This increase in knowledge of the timing could be attributed to a robust media campaign carried out by population services international to educate women of reproductive age on the correct use of the emergency pill over the last few years.
The most effective period of action of POEC has been described as the pre-ovulatory follicular phase with reports of delay of ovulation by up to 5 days by 100% [25, 26, 27], majority of the cases who took the pill (n=24) in this study and all the controls (n=3) took the pill in the secretory phase. Pulkinen and Talo [28, 29] described the myoelectrical activity of the fallopian tube and reported that progesterone inhibits tubal motility post-fertilization and could cause a delay in ovum transport resulting in EP.
Other risk factors for EP were also assessed. From this study, early age at sexual debut increased the risk of EP. The risk increased sevenfold in women who report their first sexual contact before their 15th birthday compared to those who had their first contact at 25 years and above. Sixty two percent (62.5%) of the cases had their sexual debut before their 20th birthday compared to 51.2% of the controls. A recent study in China showed a fourteen-fold increase in the risk of EP in patients who had their sexual debut before 18 years [14]. This is explained by the immaturity of the vaginal epithelium in younger people making them more susceptible to ascending infections with long-term sequelae.
Patients who conceived after a period of infertility/ subfertility were five times more likely to have an EP from this study. Twenty one percent (21%) of the cases reported a period of inability to conceive for at least 6 months after stopping the use of the contraceptive method versus 5% of the controls. Parazzini et al., in an Italian case-control study, reported a three times higher risk of EP among the cases [24]. The cause of infertility would most likely be implicated in the etiology of the EP.
There was no association between the previous use of IUCD and other long-term methods of family planning. This is in keeping with the findings of Miyoro et al. in 2002 in the same facility where he reported no association between IUCD and ectopic pregnancy [4]. Only one (0.8%) patient recruited during the study period conceived with an IUCD in situ and the pregnancy was an EP. The study done in China reported that previous use of IUCD was not significantly associated with EP. However, in the case of contraceptive failure with an IUCD in situ, the risk of EP was 21.08 higher than with no contraceptive method at the time of conception [14]. One patient (0.8%) conceived while on the mini pill during the entire study period. The resulting pregnancy was an EP. Progesterone-only pills have been reported to slightly increase the risk of EP up to 4-6% [1, 7], however from this study there was no significant association.
Sexually transmitted infections have a well-documented role in the causation of EP. The risk in this study increased three-fold with 25% of cases reporting a history of treatment for an STI compared to 10.1% of the control group. Miyoro, et al. in their study reported that 56.6% of the cases had features suggestive of PID [4]. Parazzini, et al. in an Italian study reported a six-fold increase in the risk of EP in patients who had been treated for an STI/PID [24], double what was reported in our study. Nathalie et al. in a review of several African studies concluded that PID resulting from STIs was the single most important risk factor for the development of EP in African developing countries [30]. The widespread use of antibiotics in the treatment of STIs allows some degree of patency to be maintained in the fallopian tubes resulting in EP.
This study did not show any association between EP and a history of previous abdominal pelvic surgery as reported in other studies. 20% of the cases and 27 % of the controls had a previous abdominopelvic surgery with the majority having undergone a caesarean section.
An Italian study reported an 8-fold increase in ectopic pregnancy among patients with an EP compared to the controls [24]. Our study however had a highly selected group in terms of previous caesarean section among the control. This is because KNH does not attend to low-risk antenatal mothers, who tend to receive antenatal care in smaller facilities within the county. Women with previous caesarean sections are usually referred for antenatal care and delivery to KNH which could explain the higher number of women with previous surgery in the control group compared to those in the cases.
There was no association between the previous history of tuboplasty and the risk of EP. However, only 3.3% of the cases and 1.7% of the controls had undergone tuboplasty making it difficult to draw any statistical association. This could be due to the low success rates of tuboplasty. Other studies have shown significant association in patients who had previous tuboplasty or reversal of tubal ligation who eventually conceived [24].
Limitations
Cases
The main limitation of this study was the recall of when the emergency pill was taken regarding their menstrual cycle. The majority of the participants however were noted to have recorded the dates of their last menstrual period and the dates they had unprotected coitus on their phone calendars.
Controls
The main limitation among the controls was the lack of an obstetric ultrasound hence could not be recruited into the study.
Conclusions and Recommendations
Conclusions
- Failed progesterone only emergency contraceptive increases the risk of ectopic pregnancy.
- Early sexual debut, infertility/subfertility, and previous sexually transmitted infections treatment are significant risk factors for ectopic pregnancy.
Recommendations
- Progesterone only emergency contraceptive should be recognized as a risk factor for EP and included in the client information leaflet in the drug packaging.
- Client education at the point of sale using information, education, and communication materials and advice on when to seek medical attention.
Acknowledgments
- We would like to acknowledge the following people for:
- Concept and design: xxx
- Collection and assembly of data: xxx
- Data analysis and interpretation: xxx
- Manuscript writing: xxx
- Final approval of manuscript: xxx
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Competing and conflicting Interests
The authors do not disclose any conflict of interest.
References
-
DeCherney AH, Nathan L, Murphy T, Laufer N (2006) Current Diagnosis and Treatment Obstetrics & Gynaecology. 10th(Edn.), McGraw-Hill Medical, New York, USA.
-
Andrea AC, Carrie KS, Connie LB, Suzanne Z, Cynthia JB, et al. (2011) Trends in Ectopic Pregnancy Mortality in the United States, 1980-2007. Obstet Gynecol 117(4): 837-843.
-
World Health Organization (2006) The preventable pandemic.
-
Miyoro SO (2002) Risk Factors and Seasonal Patterns of Ectopic Pregnancy at Kenyatta National Hospital. University of Nairobi, Kenya.
-
Ogunniyi SO, Faleyimu BL (1989) Fertility after an ectopic pregnancy in an African population. Int J Gynecol Obstet 30(3): 245-248.
-
Ville Y, Leruez M, Glowaczower E, Robertson JN, Ward ME, et al. (1991) The role of Chlamydia trachomatis and Neisseria gonorrhea in the etiology of ectopic pregnancy in Gabon. J Gynecol Obstet Biol Reprod 98(12): 1260- 1266.
-
Cunningham FG, Gant NF, Leveno KJ (2001) Ectopic pregnancy. In: Williams Obstetrics. 21st(Edn.), McGraw- Hill, New York, USA, pp: 884-905.
-
Cleland K, Raymong E, Trussell J, Cheng L, Zhu H, et al. (2010) Ectopic pregnancy and Emergency Contraceptive Pills: a systematic review. Obstet Gynecolo 115(6): 1263- 1266.
-
Gu XY, Yie TF (2002) Clinical study of the effect of Multiload 375SL and Levonogesterol for emergency contraception. Chin J Fam Plan 12: 740-742.
-
Cheng L, Che Y, Gülmezoglu AM (2012) Intervention for Emergency Contraception. Cochrane Database Syst Rev 8: CD001324.
-
Han X, Weng L, Jin X (1999) A comparative study of mifepristone with levonogesterol for emergency contraception. Chin J Pract Gynecol Obstet 6: 294-295.
-
American College of Obstetricians and Gynaecologists (2010) Vaginal Birth after Previous Cesarean Delivery. Practice Bulletin pp: 112.
-
Arowojolu AO, Okewole IA, Adekunle AO (2002) Comparative evaluation of the effectiveness and safety of two regimens of levonogestrol for emergency contraception in Nigerian. Contraception 66(4): 269- 273.
-
Li C, Zhao WH, Meng CX, Ping H, Qin GJ, et al. (2014) Contraceptive use and the Risk of Ectopic Pregnancy: A Multi-centre Case- Control Study. PLoS One 9(12): e115031.
-
(1998) Randomised Control Trial on Levonogesterol versus YUZPE method of Combined Oral Contraceptive for emergency contraception. Taskforce on postovulatory methods of fertility regulation. Lancet 352(9126): 428- 433.
-
Yuzpe AA, Thurlow HJ, Ramzy I, Leyshon JI (1974) Post coital contraception- a pilot study. J Reprod Med 13(2): 53-58.
-
Trussel J, Ellertson C, Hertzen HV, Bigrigg A, Webb A, et al. (2003) Estimating the effectiveness of emergency contraceptive pills. Contraception 67(4): 259-265.
-
Rodrigues I, Grou F, Joly J (2001) Effectiveness of emergency contraceptive pills between 72-120 hrs after unprotected sexual intercourse. Am J Obstet Gynecol 184(4): 531-537.
-
Hertzen HV, Piaggio G, Ding J, Chen J, Song S, et al. (2002) Low dose mifepristone and two regimen Levonogesterol for emergency contraception: A WHO Randomised Trial. WHO research group on Postovulatory Methods of Fertility regulation. Lancet 360(9348): 1803-1810.
-
Ministry of Health Kenya (2010) National Family Planning Guidelines for Service Providers. 6th(Edn.), pp: 216.
-
Farkas M (1992) The effect of oral ovulation inhibition (mono, Bi-, and Triphase) contraceptives and postinor on steroid hormones. Acta pharma Hung 62(1-2): 17-30.
-
Sue Lo, Pc Ho (2012) The Profile of Women seeking Emergency Contraception from the Family Planning Service. Hong Kong Med J 18(4): 299-303.
-
Gainer E, Mercy C, Ulmann A (2001) Levonogesterol Only Emergency contraception: Real- World Tolerance and Efficacy. Contraception 64(1): 17-21.
-
Parazzini F, Tozzi L, Ferraroni M, Bocciolone L, Fedele L, et al. (1992) Risk factors for ectopic pregnancy: an Italian case control study. Obstet Gynecolo 80(5): 821-826.
-
Muller AL, Llados CM, Croxaho HB (2003) Postcoital treatment with levonogesterol does not disrupt post fertilization events in the rat. Contraception 67(5): 415- 419.
-
Croxaho HB, Devoto L, Durand M, Ezcura E, Larrea F, et al. (2001) Mechanism of action of hormonal preparation for emergency contraception: a review of the litearature. Contraception 63(3): 111-121.
-
Hapangama D, Glassier AF, Baird DT (2001) The effects of peri-ovulatory administration of levonogesterol on menstrual cycle. Contraception 63(3): 123-129.
-
Hodgson BJ, Talo A (1978) Spike burst in rabbit oviduct: effects of estrogen and progesterone. Am J Physiology 234(4): 439-443.
-
Pulkkinen MO, Talo A (1987) Tubal physiologic consideration in ectopic pregnancy. Clin Obstet Gynecol 30(1): 164-172.
-
Goyaux N, Leke R, Keita N, Thonneau P (2003) Ectopic pregnancy in African developing countries. Acta Obstet Gynecol Scand 82(4): 305-312.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’