An Update on the Clinical Significance of Macroprolactinemia in Infertile Patients Presenting with Hyperprolactinemia: A Mini Review
Hyperprolactinemia is a frequent presentation in case of patients with infertility. As many as 15-20% of women having irregular cycles possess hyperprolactinemia. Repression of the hypothalamo-pituitary-ovarian(H-P-O)axis through hampering of liberation of pulsatile gonadotropin-releasing hormone in view of hyperprolactinemia is a frequent endocrine cause of infertility. Previously we had reviewed prolactinomas in infertility as well as how do we treat prolactinomas in infertility in 2003&2005& highlighted the structure of macroprolactin besides treatment aspect. 3 kinds of human Prolactin(Prl) are existent-namely monomeric Prl, dimeric Prl as well as macro-Prl. Macro-Prl alias big-big Prl possesses a molecular weight(MW) of >150 kDa in addition to is implicated for 5-10%of circulating Prl in healthy subjects. In case of major kind of circulating Prl is macro-Prl, a diagnosis of macroprolactinemia gets established of the patients having hyperprolactinemia 10- 46% possess macroprolactinemia. In view of the need of ruling out a pituitary prolactinoma on finding escalated quantities of Prl-routinely as reproductive endocrinology & Infertility specialists(REI) we have a tendency of getting an imaging either as a CTScan or magnetic resonance imaging(MRI) for the same. However with the major work of the group of Hattori N, in the last 2-3 decades it has been emphasized how we need to first confirm that we don’t have macro- Prl for avoidance of unindicated investigations in case of macroprolactinemia leading to escalated blood tests, imaging as well as dopamine agonists treatment which puts extra burden of cost& stress of a tumor on the patients in case of this benign disorder.
Introduction
Prolactin(Prl) gets secreted by the anterior pituitary as well as possesses kinds in the circulation [1, 2, 3]. Monomeric Prl possesses a molecular weight(MW) of 23 kDa in addition to is implicated for 89% of the full immunoreactive Prl, dimeric Prl possesses a MW of 48-56kDa as well as constitutes 5-10% along with macro-Prl possesses a MW>150 kDa in addition to is implicated for 5-10%of circulating Prl in healthy subjects [1, 2, 3, 4]. The basic kind of Prl in healthy subjects in addition to patients having Prolactinoma is monomeric Prl [2, 5, 6]. Dimeric Prl comprises of glycated monomers which generate clusters along with are benign clinically [7, 8]. Macro-Prl
comprises of antigen-antibody complexes of monomeric Prl as well as immunoglobulins, basically (IgG) [2, 9, 10]. Despite, lesser frequent, other non IgG kinds of macro- Prl are inclusive of complexes of monomeric Prl with IgA/ IgM, substantially glycated monomeric Prl or covalently bound monomeric Prl [2]. Routine Prl assays do not possess the capacity of differentiating these three3 kinds of Prl in the circulation [1].
Previously we had reviewed prolactinomas in infertility as well as how do we treat prolactinomas in infertility in 2003&2005 [11, 12]. Thus here we tried to emphasize in this minireview the recently appreciate significance of macroprolactinemia in being subjects implicated in biogeneration ofprolactinomas or any impact on fertility. Here we have tried to update how unnecessary imaging as well as dopamine agonists treatment can be avoided.
Hyperprolactinemia: Causes Along with Assessment
Hyperprolactinemia takes place physiologically at the time of pregnancy, lactation, stress, sleep, intercourse, nipple stimulation in addition to exercise [3, 5, 9]. Pathological reasons of hyperprolactinemia are inclusive of Prl secreting pituitary adenomas, hypothalamic tumors for instance craniopharyngiomas as well as infiltrating diseases (for instance sarcoidosis, histiocytosis), pituitary stalk injury, hypothyroidism, lesions on the chest wall (breast surgeries, herpes zoster) hepatorenal conditions, dopaminergic medicines (antipsychotics, prokinetic drugs), ectopic Prl generation (for instance renal cell carcinoma, ovarian teratomas), in addition to macroprolactinemia [2, 3, 5, 9]. The major kinds of Prl in the circulation are monomeric Prl [2] of the general population, 0.2-0.4% of females as well as 0.0-4.48% males are having hyperprolactinemia of which 10-46% are having macroprolactinemia [2, 3, 4, 6, 7, 9, 10, 13, 14, 15, 16, 17, 18]. Avoidance of severe exercise along with breast nipple stimulation is advocated for a minimum of 30’ prior to assessment of serum quantities of Prl [3]. Thereby need for reassessment of Prl quantities is there in case of escalated Prl quantities are encountered (Prl quantities greater than upper limit of normal (20-25ng/ml) based on the laboratory on 2 different times [3]. Thereby need for reassessment minimum onetime exists [5]. Nevertheless, in case of escalated Prl quantities greater than100ng/ml, one Prl determination is enough for making the diagnosis of Hyperprolactinemia [3] (Table 1).
| Serial number | Pituitary Diseases | Hypothalamic Diseases | Neurogenic | Others | Idiopathic | Medications |
|---|---|---|---|---|---|---|
| 1 | Empty Sella Syndrome | Pituitary stalk section | Breast nipple stimulation | Cirrhosis | Lesions | Phenothiazines |
| 2 | Prolactinomaas | Meningiomas | Chest wall lesions | Pseudocyesis | Reserpine | |
| 3 | Acromegaly | Dysgerminomas | Spinal cord lesions | Chronic renal failure | Metoclopramide | |
| 4 | Cushinge’s Disease | Vascular | Hypothyroidism | Tricyclic antidepressants | ||
| 5 | Lymphocytic | Other tumors | Adrenal Insufficiency | Haloperidol | ||
| 6 | Hypophysitis | sarcoidosis | Methyldopa | |||
| Neuraxis irradiation | monoamine oxidase inhibitors | |||||
| 8 | Non secreting Pituitary adenomas | Amoxepin | ||||
| 9 | Craniopharyngeomas | Cocaine | ||||
| 10 | Verapamil | |||||
| 11 | Fluoxetine |
Table 1: Causes of Hyperprolactinemia.
Structure of Macroprolactin (Macro- Prl)
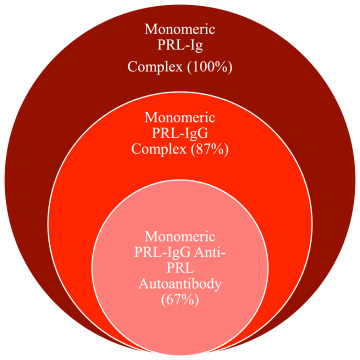
Macroprolactin is constituted of complexes of monomeric Prl as well as immunoglobulins of these maximum macro-Prl (87%) is comprised of monomeric Prl which forms complexes with IgG [3, 9, 19, 20]. Out of these kinds of Prl-IgG complexes maximum (67%) implicates anti Prl– autoantibodies (Figure1).
It has been posited regarding the presence of genetic susceptibility to post-translational modifications of monomeric Prl for instance, glycosylation as well as phosphorylation, stimulates the generation of auto antibodies to the newer epitopes [3, 22]. A significant positive association amongst titres of anti Prl –autoantibodies in addition to serum Prl quantities, which corroborates this posit with regards to anti Prl – autoantibodies are the etiological factors for macroprolactinemia [9, 14]. Furthermore, macro-Prl has been with isolated from the cord blood from the mother possessing macroprolactinemia pointing that passive transfer of Prl- IgG complexes takes place [14].
The negative feed back loop hypothalamic - anterior pituitary does not work normally in subjects having macroprolactinemia. Normally Prl possess the capacity of crossing blood brain barrier (BBB) followed by binding to Prl- receptors on the tubero infundibular cells of thehypothalamus, which liberate dopamine in addition to result in reduction of the escalated quantities of Prl liberated from the anterior pituitary [20]. Nevertheless, in view of Prl- IgG complexes having a MW>150 kDa do not possess the capacity of crossing the BBB for gaining accessibility to Prl- receptors on the tubero infundibular cells of the hypothalamus; thus escalated quantities of Prl found in macroprolactinemia do not possess the capacity of resulting in the down regulation of monomeric Prl secretion from the anterior pituitary [9, 13, 14, 20]. Instead in patients having macro- Prl in the form of the main kind of Prl in the circulation, monomeric Prl usually possess the capacity of sustenance of the normal Prl quantities [9, 14].
One more sequelae of the macro- Prl’s enhanced MW>150 kDa is diminished filtration from the glomeruli along with diminished renal clearance in contrast to monomeric Prl [2, 3, 14, 21]. This results in >serum quantities of macro- Prl, thereby hyperprolactinemia. The hyperprolactinemia secondary to macroprolactinemia is dependent on postponed clearance of macro- Prl instead of escalated generation of Prl [3].
Actual Hyperprolactinemia along with Macroprolactinemia Clinical Manifestation
The canonical symptoms correlated with monomeric Prl or actual hyperprolactinemia in case of women are irregularperiods, amenorrhea in addition to galactorrhea [4, 11]. Nevertheless, in men hyperprolactinemia is correlated with diminished libido, impaired erection as well as galactorrhea [11]. These actions take place from the hampering actions of Prl on liberation of pulsatile gonadotropin-releasing hormone from the hypothalamus hampering of kisspeptin neurons that express Prl receptors along with stimulatory actions on mammary cell proliferation [2]. Thirunavakkarasu K, et al. [1], illustrated that patients having macroprolactinemia possess the lesser capacity in contrast to patients with actual hyperprolactinemia to manifest irregularperiods as well as galactorrhea,14% vis a vis 46%; p<0.008 in addition to 5% vis a vis 30%; p=0.1 respectively. These observations of reduction in symptoms in case of patients having macroprolactinemia in contrast to actual hyperprolactinemia have been reproduced in other studies [4, 15, 18]. The blunted phenotype of patients having macroprolactinemia is dependent on the lesser bioavailability of macro- Prl in contrast to monomeric Prl [3]. Prl – autoantibodies as well as Prl receptors binding takes place in the akin sites of Prl molecules [9]. Thereby, it has been hypothesized that Prl–autoantibodies existent in patients having macroprolactinemia have competitive actions with Prl receptors with regards to binding of free Prl [9]. Furthermore, macro- Prl is generally restricted to vascular spaces in view of its greater MW, thereby, its incapacity of gaining accessibility to its target organs for instance pituitary along with hypothalamus [2, 3, 12, 20, 21]. It has been posited that lesser oligomenorrhea along with galactorrhea felt by patients having macroprolactinemia are in view of transitory disassociation of monomeric Prl from its immunoglobulins, thereby a short term escalation of monomeric Prl [2, 21].
Numerous patients having macroprolactinemia possess serum quantities of Prl lesser than100 ng/ml [3]. Nevertheless, remarkable variation of Prl quantities varying from 20-663ng/ml (average 61±66ng/ml) [3]. An overlap is existent amongst quantities of Prl in macroprolactinomas, microprolactinomas, drug stimulated hyperprolactinemia along with primary hypothyroidism [3]. Kalsi AK, etal. [18], illustrated no significant variation in the average quantities of Prl in case of patients having macroprolactinemia in addition to actual/true Hyperprolactinemia (137ng/ml vis a vis164 ng/ml p=0.054). With the acknowledgement regarding overlap of symptoms along with quantities of Prl correlated with actual/true monomeric hyperprolactinemia in addition to macroprolactinemia, accurate diagnosis estimation is not feasible dependent on symptoms or laboratory Prl quantities by themselves [2, 3, 6, 13, 16]. Additionally, a subset of patients might be having macroprolactinemia in addition to other reasons of Hyperprolactinemia [2, 3, 7]. In those patients having macroprolactinemia who illustrate neurological signs along with symptoms suggestive of an intracranial mass are having the requirement of further assessment with the utilization of pituitary imaging [3]. As many as 26% of patients having macroprolactinemia possess concurrent prolactinomas that are usually correlated with enhancement of monomeric Prl [14, 23].
Appropriately isolating the cause of hyperprolactinemia is of utmost significance in view of considerably significant variations in the form of management. For instance dopamine agonists as well as / surgery are utilized for prolactinomas treatment, Thyroid hormone needs to be supplemented in case of primary hypothyroidism in addition to omitting dopamine antagonists if it is secondary to drug stimulated Hyperprolactinemia [3]. Usually dopamine agonists portray the first line of treatment with regards to patients having Hyperprolactinemia [9,rev by us in 10,1]. Nevertheless, once delivered to patients having macroprolactinemia, there is a minimum reduction in quantities of Prl [9]. Moreover usually there is no requirement for treatment of macroprolactinemia [2, 3].
Establishment of Diagnosis of Macroprolactinemia
Immunoassays
The greatest hurdle in macroprolactinemia diagnosis is that immunoassays do not possess the capacity of discriminating monomeric Prl from dimeric Prl, macro-Prl, or Prl fragments [9, 23, 24]. This results in incorrect diagnosis of hyperprolactinemia, unessential imaging of pituitary in addition to without indication of dopamine agonists delivery be performed [7, 8, 10, 21, 25]. Thereby, it is imperative that once immunoassays determine escalation of Prl quantities screening for the existence of macro- Prl [21]. A study which implicated 6 immunoassays illustrated controversial Prl quantitiesin patients having macroprolactinemia [25]. Furthermore, an evaluation of the immunoassay pretended to be minimally reactive with macro- Prl crossreacted with macro- Prl in 50% of the patients having macroprolactinemia [10]. These studies highlighted that immunoassays do not possess the capacity of discriminating macro- Prl from monomeric Prl. Although Endocrine Society advocated that there is requirement for screening full lot of patients having hyperprolactinemia for macroprolactinemia, this practice has not been adopted at universal level [23, 25]. Recently Muhtaroglu S, etal. [19], observed that out of assessment of 5007 serum samples for Prl continuously, 900/ 5007(17.9%) possessed escalated quantities of Prl, with the providers asking for screening just in 171/900(19%) samples. Out of the 171 patients who had undergone screening for macro- Prl by utilization of polyethylene glycol (PEG) precipitation method, 31 had a diagnosis of macroprolactinemia [19].
PEG Precipitation Method
Precipitation of macro- Prl utilizing PEG refers to a simple, rapid, available, cheap strategy for screening for macro- Prl as well as can be contrasted with the gold Standard gel filtration chromatography [2, 7, 9, 21]. This PEG results in dehydration of proteins leading to reduction in solubilization followed by precipitation [24]. On exposure to PEG immunoglobulins are depleted of their solubility, that results in precipitation of Prl- IgG complexes in addition to reduction in quantities of Prl in the supernatant [3, 14, 20]. With regards to estimation of precipitation of free Prl with the PEG, a serum sample mixing is performed with 12.5- 25% PEG followed by centrifugation, while one more serum sample mixing is performed with water for estimation of full quantities of Prl [9, 14]. Subsequently assay of the Prl in the supernatant is carried out. The proportion of Prl which gets precipitated by PEG refers to macro- Prl, gets determined in the form of (full Prl- free Prl) / full Prl x 100 [9]. In case of proportion of Prl which gets precipitated by PEG is ≥ 60% suggesting recovery of monomeric Prl is ≤ 40%, a diagnosis of macroprolactinemia is made [1, 7, 9, 13, 14, 16]. The sensitivity as well as specificity of PEG precipitated Prl are 100% as well as 94% respectively [20]. Once ≤ 40% recovery of monomeric Prl is considered to be the cutoff, 3.3% of patients have a diagnosis of macroprolactinemia made in contrast to 8.8% of patients when utilization of cutoff of ≤ 60% is done [21]. PEG precipitation method utilization is done in the form of a screening strategy instead of diagnostic in view of absence of specificity for macro- Prl [2]. A restriction of this laboratory method is PEG results in precipitation of certain Prl- IgG complexes that results in lesser detection of monomeric Prl, specifically in patients having concurrent macroprolactinemia in addition to supraphysiological monomeric Prl [2, 21]. Simultaneous prolactinomas need to be suspicious in case monomeric Prl continues to be escalated although≤ 40% recovery takes place with PEG precipitation [5]. Additionally, PEG just partly results in precipitation of IgA leading to macroprolactinemia implicating IgA- Prl
complexes to get wrongly diagnosed [26, 27, 28, 29, 30]. In toto, it has been determined regarding PEG precipitation resulting in accurate diagnosis of macroprolactinemia in 80% of patients [5].
Other Methodologies
Gel filtration chromatography portrays the gold standard for estimating macro- Prl; nevertheless, it is cost prohibitive in addition to takes up a lot of time [2, 3, 7, 9, 13, 25]. Thereby this methodology gets utilized just for corroborating the diagnosis of macroprolactinemia by separation of Prl dependent on molecular size [9]. Other methodologies for corroborating the diagnosis of macroprolactinemia are protein A/G column in addition to I125- Prl binding regions [9]. Protein A/G column implicates binding of Protein A to the Fc part of the immunoglobulin in the Prl -immunoglobulin complex, while Protein G binding takes place just with IgG, the commonest immunoglobulin in macro- Prl [9]. Despite this event possesses the capacity of isolating Prl- IgG complexes with dependence, being cost prohibitive, is not having the capacity of isolating the subset of immunoglobulins apart from IgG [9]. I125- Prl binding implicates a serum sample mixing to start with I125- Prl, followed by with PEG with subsequent centrifugation [9, 14]. Determination of the gamma radioactivity of the sediment is performed, which possesses the capacity of isolating the existence of anti Prl – autoantibodies [9]. Despite I125- Prl binding possesses the capacity of estimating a subset of Prl- IgG complexes, those having anti Prl – autoantibodies, this does not possess the capacity of estimating all macro- Prl [9]. Moreover, this event takes up a lot of time in addition to has requirement of availability of radioisotope laboratory [9].
Repercussions of Macroprolactinemia
Thirunavakkarasu K, etal. [1], illustrated that 183/1167(ie 15.7%) patients having presentation with infertility possessed hyperprolactinemia. Whereas 5.8% patients having polycystic ovary syndrome (PCOS) were observed to have macroprolactinemia [30]. Women having macroprolactinemia possess the capacity of having a pregnancy, propagation via normal pregnancies, delivering healthy neonates, lactate in addition to go through postpartum period without any kind of the treatment for Hyperprolactinemia [9, 14]. It is imperative to discriminate macroprolactinemia from actual/true hyperprolactinemia for avoidance of unnecessary imaging as well as deliver dopamine agonist treatment in a patient basically having macroprolactinemia [31].
Long term follow up studies have illustrated that macroprolactinemia is continuous, however no propagation of symptoms take place [2, 9, 15]. A prospective cohort study of 51 patients with macroprolactinemia found that for an average 9.9 yrs illustrated persistence of macroprolactinemia on follow up with no propagation of symptoms [4]. Moreover, of these 29/43 patients had spontaneous conception at the time of follow up [4]. Hattori N, et al. [17], observed on following 27 women having macroprolactinemia for 4 yrs as well as at the time of study period, both total along with free Prl did not alter significantly. A further study by Hattori N, et al. [32], illustrated that following for 4.4yrs(2- 17yrs)range,ratios of PEG precipited Prl, IgG bound Prl, monomeric Prl continued tobe having stability [32].This point that although macroprolactin is heterogenous in case of macro- Prl with IgG as well as nonIgG bound monomers of Prl, constitution of macroprolactin continues to have stability with time [32]. Prospective follow up studies point that macroprolactinemia portrays a benign disorder with no requirement of imaging or any dopamine agonist treatment. Nevertheless, for making the diagnosis of macroprolactin it becomes imperative to screen serum samples in case of hyperprolactinemia for macroprolactin.
Clinical Recommendations
In view of the greater prevalence of hyperprolactinemia amongst couples with presentation of female factor infertility in addition to 11.5% incidence of macroprolactinemia amongst such patient population, there is requirement of routinely screening on noticing a patient with continuous Hyperprolactinemia [1]. This is in agreement with that is what are the endocrine society clinical practice guidelines to evaluate for macroprolactinemia in case of patients having Hyperprolactinemia which is asymptomatic [23]. On observation of escalated Prl there is requirement of repeating it minimum once in the fasting status with reflex testing for macro- Prl. Reflex testing for macro- Prl in case of all serum samples having escalated quantities of Prl needs to be started over all laboratories instead of provider started screening for macro- Prl. This would escalate the safety, the way a study by Muhtaroglu S, etal. [19], illustrated that 77% of serum samples having quantities of Prl greater than reference range got ignored with regards to screening for macro- Prl on leaving to the provider for asking for macro- Prl evaluation. In general total screening for macro- Prl has been greater implemented in Europe in contrast to North America [7]. At present macroprolactinemia diagnosis is necessary in view of patients referred to as possessing so termed idiopathic hyperprolactinemia generally undergo repeated CT Scan in addition to magnetic resonance imaging (MRI) for placement of a microadenoma in the pituitary along with treatment with the dopamine agonist treatment as well as rarely unindicated surgical evaluation [8, 14]. Thereby reflex testing for macro- Prl is advocated for all repeated serum samples with the quantities of Prl greater than upper limit of normal for that laboratory (Figure 2).
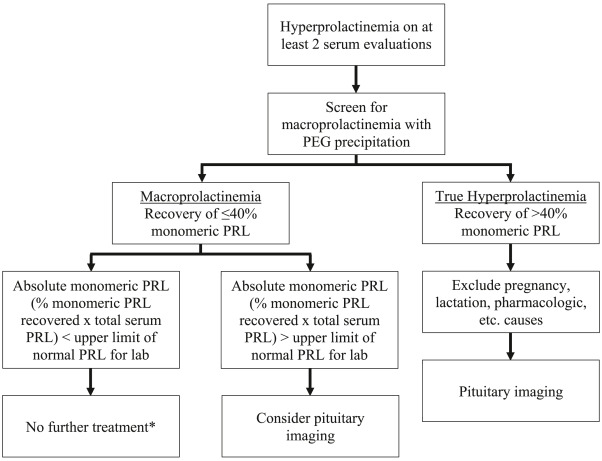
Patients having hyperprolactinemia in addition to mainly macro- Prl no requirement of imaging or any dopamine agonist treatment exists [2]. Nevertheless, in case absolute monomeric Prl continues to be greater than upper limit of normal for that laboratory subsequent to PEG precipitation, it is advocated to take into account an imaging of pituitary for assessment of a simultaneous pituitary adenoma. Although to start with escalated cost regarding reflex testing for macro- Prl, routinely screening of all women having hyperprolactinemia has a justification from point of view of economy in view of it leading to reduction in health care expenses of imaging along with dopamine agonists treatment [2, 6, 7]. Evaluation of expenses implicating 1793 patients having escalated quantities of Prl(≥ 30ng/ml) of which 63.5% had got the diagnosis of actual/true Hyperprolactinemia whereas 35.6% had macroprolactinemia, illustrated that persistence of unindicated investigations in case of macroprolactinemia leading to escalated blood tests, imaging as well as dopamine agonists treatment puts extra burden [6]. Chutpiboonwat P, et al. [33], evaluation the properties of the Thai patients having macroprolactinemia. They conducted a crossectional study, in 56 hyperprolactinemic patients (51 female along with 5 male) with the assessment of their sera with regards to macroprolactin. Subsequent to of polyethylene glycol(PEG) precipitation, a recovery rate of 40% of serum prolactinpointed to presence of macroprolactinemia. Their study displayed 19.64%(11/56) of patients with Hyperprolactinemia were observed to be having basically macroprolactin. All their patients having macroprolactinemia were females out of which 8 had a diagnosis of idiopathic Hyperprolactinemia in addition to got unnecessary dopamine agonists treatment. Intriguingly, neuroradiological aberrations existed in three patients having macroprolactinemia, two patients having prolactinomas along with a case with stalk effect hyperprolactinemia. Thereby practically one fifth of their patients having hyperprolactinemia possessed macroprolactinemia. This pointed to diagnostic algorithm of all patients with hyperprolactinemia needs the inclusive of PEG precipitation [33].
Conclusion
The full patient numbers of patients presenting in the form of hyperprolactinemia need screening regarding macroprolactinemia. Reflex testing for macro- Prl in cases of hyperprolactinemia might be wrongly diagnosed, unindicated imaging as well as incorrect treatment in addition to considerable degree of stress for patients along with their providers [27]. Being simple, associated with the gold standard Gel filtration chromatography along with substantially greater sensitivity as well as specificity, PEG precipitation method is a considerably good method for isolating patients having macroprolactinemia who have continuously escalated quantities of prolactin [15].
References
-
Thirunavakkarasu K, Dutta P, Sridhar S, Dhaliwal L, Prashad GRV, et al. (2013) Macroprolactinemia in hyperprolactinemic infertile women. Endocrine 44: 750- 755.
-
Kasum M, Oreskovic S, Cehic S, Sunj M, Lila A, et al. (2017) Laboratoryand Clinical significance of macroprolactinemia in women with macroprolactinemia hyperprolactinemia. Taiwan J Obstet Gynaecol 56: 719- 724.
-
Vilar L, Flesceriu M, Bronstein MD (2014) Challenges and pitfalls in the diagnosis of macroprolactinemia. Arq Bras Endocrinol Metab 58(1): 9-22.
-
Wallace IR, Satti N, Courtney CH, Leslie H, Bell PM, et al. (2010) Ten year Clinical follow up of a cohort of 51 patients with macroprolactinemia establishes it as a benign variant. J Clin Endocrinol Metab 95(7): 3268- 3271.
-
Vilar L, Vilar CF, Lyra R, Freitas MDC (2019) Pitfalls in the diagnostic evaluation of hyperprolactinemia. Neuroendocrinology 109(1): 7-19.
-
Soares PCD, Souza SCDAL, Vieira JGH, Ferraz MB (2019) The effects of identifying macroprolactinemia on health care utilization and cost in patients with elevated serum prolactin levels. Value in Health 12(6): 930-934.
-
Sampson SL, HamrahianAH, Ezzat S (2015) American Association of Clinical Endocrinologists, American College of Endocrinology disease state Clinical review: Clinical relevance of macroprolactin in the absence or presence of true hyperprolactinemia. Endocrin Pract 21(12): 1427-1435.
-
Nguyen KQN, Langevin RH, McPhaulMJ, Hashim JA (2021) Circulating macroprolactin exhibits molecular heterogeneity and is not exclusively an antibody complex. ClinChim Acta 514: 90-95.
-
Shimatsu A, Hattori N (2012) Macroprolactinemia: diagnostic, clinical and pathogenic significance. Clin Dev Immunol 2012: 167132.
-
Hattori N, Aisaka K, Shimatsu A (2016) A possible cause of the variable detectability of macroprolactin by different immunoassay systems. Clin Chem Lab Med 54(4): 603-608.
-
Kochar KK, Virk SPS (2003) Prolactinomasin infertility. The Reviews in Gynaecological Practice 3(4): 180-187.
-
Kochar KK, Allahabadia GN, Singh M (2005) How do we treat prolactinomas in infertility. In: Allahbadia GN, et al. (Eds.), Gynaecological Endoscopy & Infertility. 1st(Edn.), Jaypee Brothers Medical Publishers, 10: 85-96.
-
Can M, Guven B, Atmaca H, Ackgoz S, Mungan G, et al. (2011) Clinical characterization of patients with macroprolactinemia and monomeric hyperprolactinemia. Kahosiung J Med Sci 27: 173-176.
-
Hattori N (2003) Macroprolactinemia: a new cause of hyperprolactinemia. J Pharmacol Sci 92(3): 171-177.
-
Bagatani SR, Lhullier FL, MallmannES, Spitzer PM (2013) Macroprolactinemia in women with hyperprolactinemia: a 10-yearfollow up. Neuroendocrinol Lett 34(3): 207- 211.
-
Isik S, Berker D, Tutuncu YA, Ozuguz U, Gokay F, et al. (2012) Clinical and radiological findings in macroprolactinemia. Endocrine 41: 327-333.
-
Hattori N, Adachi T, Ishihara T, Shimatsu A (2012) The natural history of hyperprolactinemia. Eur J Endocrinol 166: 625-629.
-
Kalsi AK, Halder A, Jain M, Chaturvedi PK, Sharma JB, et al. (2019) Prevalence and reproductive manifestations of macroprolactinemia. Endocrine 63: 332-340.
-
Muhtaroglu S, Keti DB, Hacloglu A (2019) Macroprolactin: an overlooked reason for hyperprolactinemia. J Lab Med 43: 163-168.
-
Yang W, Guo Z, Zhou Y, Du J, Liu H, et al. (2021) Optimization of a screening method for macroprolactinemia. J Chromatogr B 1175: 122723.
-
Koniares K, Benadiva C, Engmann L, Nulsen J, Grow D, et al. (2023) Macroprolactinemia: a mini review and update on Clinical Practice. Fertil Steril Rep 4(3): 245- 250.
-
Sostanic M, Bokulic A, Marijanevic D, Zec I (2019) Optimizing laboratory defined macroprolactin algorithm. Biochem Medica 29(2): 020706.
-
Melmed S, Casaneuva FF, Hoffman AR, Kleinberg DL, Montori VM, et al. (2011) Diagnosis and treatment of Hyperprolactinemia: An endocrine Society Clinical Practice Guidelines. J Clin Endocrinol Metab 96(2): 273- 288.
-
Melmed S, Koenig R, Rosen C, Richard GAA, Goldfine AB (2019) Williams Textbook of Endocrinology. 14th(Edn.), Elsevier, Netherlands.
-
Beltran L, Fahie-Wilson MN, McKenna TJ, Kavanagh L, Smith TP, et al. (2008) Serum totalprolactin and monomeric prolactin reference intervals determined by precipitation with polyethylene glycol: evaluation and validation on common immunoassays platforms. Clin Chem 54(10): 1673-1681.
-
Leslie H, Courtney CH, Bell PM, Hadden DR, McCance DR, et al. (2001) Laboratory and clinicalexperience in 55patients with macroprolactinemia identified by a simple polyethylene glycolprecipitation method. J Clin Endocrinol Metab 86(6): 2743-2746.
-
Fahie-Wilson M, Smith TP (2013) Determination of prolactin: The macroprolactin problem. Best Pract Res Clin Obstet Gynaecol 27(5): 725-742.
-
Overgaard M, Pedersen SM (2017) Serum prolactin revisited: reference intervals and polyethylene glycol precipitation-based methods for discrimination between hyperprolactinemia and macroprolactinemia. Clin Chem Lab Med 55(11): 1744-1753.
-
Hu Y, Ni J, Zhang B, Cheng W, Zhang H, et al. (2021) Establishment of reference intervals of monomeric prolactin to identify macroprolactinemia in Chinese patients with increased total prolactin. BMC Endocrin Disord 21(1): 197.
-
Ke X, Wang L, Duan L, Yang H, Jia Y, et al. (2023) Comparison of PEG precipitation and ultra filtration treatment for macroprolactin in Chinese patients with hyperprolactinemia. Clin Chimica Acta 544: 117358.
-
Hayashida SAY, Marcondes JAM, Soares JM, Rocha MP, Barcellos CRG, et al. (2014) Evaluation of macroprolactinemia in 259 women under investigation for Polycystic ovary syndrome. Clin Endocrinol 80: 616- 618.
-
Hattori N, Ishihara T, Saiki Y, Shimatsu A (2010) Macroprolactinemia in patients with hyperprolactinemia:composition of macroprolactin and stability the longterm follow up. Clin Endocrinol 73: 792-797.
-
Chutpiboonwat P, Yenpinyosuk K, Sridama V, Kunjan S, Klaimukh K, et al. (2020) Macroprolactinemia in patients with hyperprolactinemia: An experience from a single tertiary centre. Pan Afr Med J 36: 8.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’