WHO Labour Care Guide: New Generation Partograph
WHO Labour Care Guide (LCG) aims to provide evidence-based, good quality and respectful maternity care during intrapartum period, regardless of the setting or available resources. On contrary to the conventional partograph, LCG is an innovative labour monitoring-to-decision tool which provides monitoring of labour progress and timely reminders on required interventions. Various available sections of LCG also facilitates early identification of potential complications and timely referral if required. The present manuscript provides a comprehensive insight on WHO LCG – its relevance, various sections and need for implementation in present scenario.
Mini Review
In early1990s, partogram was approved by World Health Organization (WHO) as a routine tool for displaying progress of labour and since then it has been used globally. Despite its global acceptance, the utilization and correct completion rates have been reported as low as 31 and 3%, respectively [1, 2]. In 2018, WHO revised the partogram in view of the recent evidence of the individual variation in progress of labour resulting in good perinatal outcomes, and the fact that many women do not undergo labour that corroborates with the average rate of Partogram. Globally, approximately 140 million births occur every year and the time of birth is crucial to survival of mothers & their infants. More than one-third of maternal deaths, half of stillbirths and a quarter of neonatal deaths result from complications during labour & childbirth, which are largely preventable. Thus, improving the quality of care around the time of birth has been identified as the most impactful strategy for reducing stillbirths, maternal and newborn deaths, as compared with antenatal or postpartum care strategies-2030 Agenda for Sustainable Development.
WHO published a consolidated set of recommendations on intrapartum care for a positive childbirth experience in Labour Care Guide (LCG) manual and discourages ineffective practices. The aim of the guideline is to improve the quality of essential intrapartum care with the ultimate goal of improving maternal, foetal and newborn outcomes. It has 26 new recommendations, 30 existing recommendations, it starts from labour onset through to the immediate postnatal period and can be applied to any health care setting [3].
Labour and childbirth should be individualized and woman-centred. No intervention should be implemented without a clear medical indication, and only interventions that serve an immediate purpose and proven to be beneficial should be promoted. Healthy pregnant women continue to be subjected to ineffective and potentially harmful routine labour interventions such as perineal shaving, enema, amniotomy, intravenous fluids, antispasmodics and antibiotics for uncomplicated vaginal births. Hence, WHO recommendation is a need of an hour because of overmedicalization of childbirth and increasing caesarean section rates.
Regarding labour progression, there is continuous debate on what is normal progress of labour and the validity of one of the most important components of the partograph, the alert and action lines, has been questioned [4]. Findings of several studies suggest that labour can indeed be slower than the limits proposed in the 1950s by Emmanuel Friedman [5] (Figure 1).
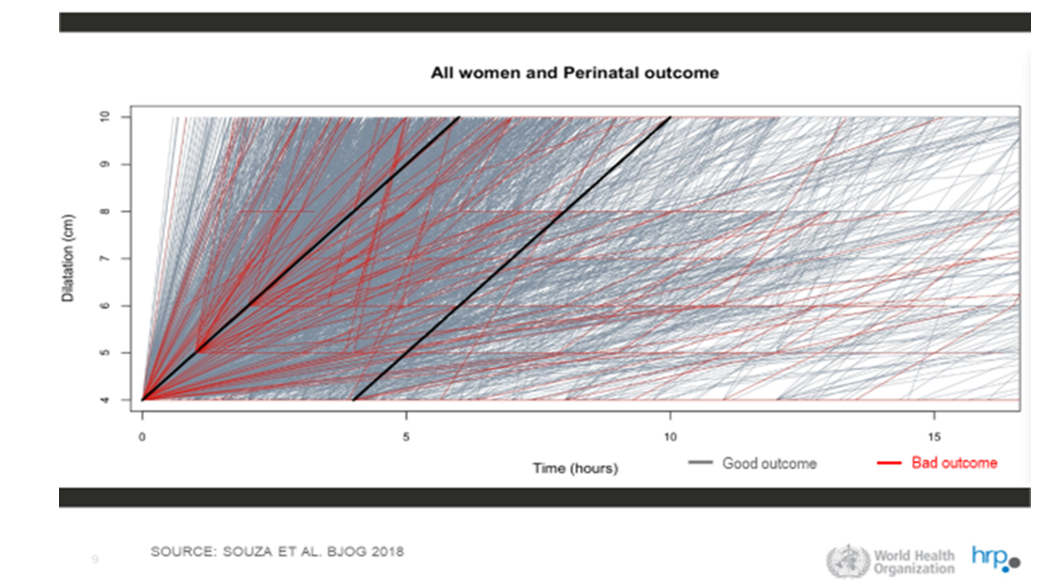
An expectation of a minimum cervical dilatation threshold of 1 cm/hour throughout the first stage of labour is unrealistic for most healthy nulliparous and parous women [6]. This cervical dilatation rate of 1cm/hr throughout active first stage is impractical fast for some women and therefore not recommended for identification of normal labour progression whereas slower than 1cm/hr cervical dilatation rate alone should not be a routine indication for obstetric intervention [7]. Labour may not naturally accelerate until a cervical dilatation threshold of 5cm is reached. Therefore, use of medical interventions to accelerate labour and birth such as oxytocin augmentation or caesarean section before this threshold is not recommended, provided that foetal and maternal conditions are reassuring. Documentation on LCG should be initiated when the woman enters active phase of first stage of labour i.e. 5cm or more cervical dilatation, regardless of parity and membranes. Alert and action lines are no longer used and second stage is included in new generation partograph-WHO LCG. Evidence-based alerts are defined to decide upon the further management plan.
Second stage of labour is the period between full cervical dilatation and birth of baby, during which the woman has an involuntary urge to bear down, as a result of expulsive uterine contractions. Women should be informed that the duration of second stage varies from one woman to another. In first labours, birth is usually completed within 3 hours whereas in subsequent labours, it takes usually 2 hours to complete.
How it is different from old partogram
Active phase defined as starting from 5 cm of cervical dilatation as compared to 4cm, evidence-based time limits at each cm of cervical dilatation and not fixed 1 cm/hour ‘alert’ line and ‘action’ lines, and intensified monitoring in second stage. It also adds explicit recording of labour companionship, pain relief, oral fluid intake and posture in addition. Further, it records only duration and frequency of uterine contractions, intensity is removed due to subjective variation. It also requires deviations to be highlighted by putting a red circle and the corresponding response to be recorded by the provider.
Structure of Labour Care Guide
It has 7 sections Section 1: Identifying information & labour characteristics at admission Section 2: Supportive care Section 3: Care of the baby Section 4: Care of the woman Section 5: Labour progress Section 6: Medication Section 7: Shared decision making For all observations, there is a horizontal time axis for documentation of the corresponding time of observation and a vertical reference values axis for determination of any deviation from normal observations. Time should be recorded using 12- or 24- hour format, depending on local practice. The reference “Alert” column presents thresholds for abnormal labour observations which require further assessment and action by health care provider. If labour observations do not meet any of the criteria in the “Alert” column, labour progression and care should be regarded as normal, and no medical intervention is warranted.
The Labour Care Guide creates positive feedback and decision-making loop, as health personnel are encouraged to regularly:
- Assess: Assess the well-being of woman and her baby, and progress of labour.
- Record: Document labour observations.
- Check Reference Threshold: Compare labour observations with reference values in the “Alert” column.
- Plan: Decide whether and what interventions are required, in consultation with the woman, and document accordingly (Figure 2).

Thus, this LCG tool is intended as a resource to ensure evidence-based quality care, with a special emphasis on ensuring safety, avoiding unnecessary interventions, and providing supportive care.
References
-
WHO (2021) WHO Labour Care Guide: User’s Manual. World Health Organization, Geneva, Switzerland.
-
Hofmeyr GJ, Bernitz S, Bonet M, Bucagu M, Dao B, et al. (2021) WHO next-generation partograph: revolutionary steps towards individualised labour care. BJOG 128(10): 1658-1662.
-
WHO (2018) WHO Recommendations: Intrapartum Care for a Positive Childbirth Experience. World Health Organization, Geneva, Switzerland.
-
Bonet M, Oladapo OT, Souza JP, Gülmezoglu AM (2019) Diagnostic accuracy of the partograph alert and action lines to predict adverse birth outcomes: a systematic review. BJOG 126(13): 1524-1533.
-
Zhang J, Duan T (2017) The physiologic pattern of normal labour progression. BJOG 125(8): 955.
-
Oladapo OT, Diaz V, Bonet M, Abalos E, Thwin SS, et al. (2018) Cervical dilatation patterns of ‘low-risk’ women with spontaneous labour and normal perinatal outcomes: a systematic review. BJOG 125(8): 944-954.
-
Abalos E, Chamillard M, Díaz V, Pasquale J, Souza JP, et al. (2020) Progression of the first stage of spontaneous labour. Best Pract Res Clin Obstet Gynaecol 67: 19-32.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’