Reversible, Long-Action Reproductive Control with Frameless IUD for Intracesarean Insertion
Immediate post placental IUD insertion at the time of cesarean section provides a good opportunity to achieve long-term contraception with minimal discomfort to the patient. Return to fertility post-delivery is not always predictable as it can occur as soon as 3 weeks in nonlactating women and may not necessarily be accompanied by menses
Short Communication
Immediate post placental IUD insertion at the time of cesarean section provides a good opportunity to achieve long-term contraception with minimal discomfort to the patient. Return to fertility post-delivery is not always predictable as it can occur as soon as 3 weeks in non- lactating women and may not necessarily be accompanied by menses. According to the World Health Organization, contraception post-cesarean delivery is a necessity for at least 24 months, to allow the scar to heal as rupture of the uterus during the next pregnancy is often catastrophic [1]. Use of contraception as early as possible post-delivery would assure prevention of uterine rupture post-cesarean section allowing for the wound to heal as well as for the woman to fully recover from her pregnancy. Immediate IUD insertion has been found to be safe as no significant differences in postpartum hemorrhage, continuance of lochia was observed, and healing of uterus was found to be normal. No studies have shown any increase in the risk of infection or other complications either related to IUD insertion during cesarean section delivery [2]. Both copper IUDs and also levonorgestrel- releasing intrauterine system (LNG-IUS) can be used as the hormone released in the uterine cavity does not affect breast feeding [3]. According to a study conducted in Egypt, the levonorgestrel intrauterine system fitted at the time of elective cesarean was associated with significant reductions in the duration and amount of puerperal blood loss, as well as a high incidence of amenorrhea and lighter periods there after [4]. This may be important to help women recover more quickly from anemia after childbirth and avoid the break through bleeding and spotting episodes that often lead to removal of the LNG- IUS. All IUDs can be used for immediate insertion post- delivery. However, most reports mention higher expulsion rates varying from around 5% at 12 months to up to 50% and even higher if partial expulsions are included in the analysis [5, 6, 7, 8]. Çelen at al. conducted a study in two hundred forty-five women in Turkey with term pregnancies delivered by cesarean section. The participants were examined before hospital discharge and at 6 weeks postpartum. Expulsion occurred in 17.6% of women. Greater than one fourth of the participants discontinued IUD use due to spontaneous expulsion or other medical reasons [9]. A problem with conventional IUDs and the LNG-IUS is that even if the IUD is retained in the large involuting uterus, many IUDs displace from their original location. Misalignment and rotation was common with both LNG- IUS and copper IUD on ultrasound examination in an immediate postplacental study in cesarean patients conducted in Egypt. The devices were displaced in almost half of the women.4Displacement will likely cause discrepancy and embedment during involution of the uterus, particularly during prolonged lactation as hyper involution in these women is not uncommon [10]. Attempts to solve the expulsion problem of IUDs inserted postpartum has a long history [11]. To solve this problem, a new method to fix copper cylindersto the fundus of the postpartum uteruswas recently developed (Figure 1a). The procedure is simple and can be performed under 4 minutes with no discomfort to the patient and minimal surgical risk. The technique consists of the precise placement of the anchoring knot immediately below the serosa of the uterus, followed by fixing the knot in place with an absorbable suture. The IUD tail is looped in the cervical canal or is cut at the level of the cervix. To check IUD placement, a follow-up sonography can be performed to localize the stainless steel marker attached to the anchoring knot (Figure 1b). The anchor can also easily be removed by pulling on its lower end (tail). Unlike irreversible sterilization methods return of fertility is immediate. Ongoing studies confirm the efficacy of the technique and the high acceptability of the frameless IUD by women.
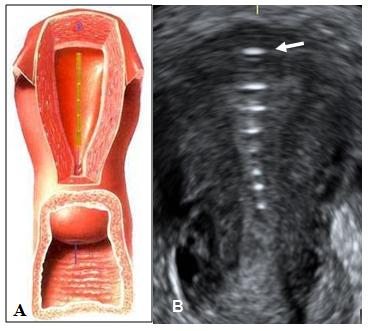
Figure 1: A) Frameless IUD attached to the fundus of the uterus. B) Coronal ultrasound of the IUD in situ at follow-up. The arrow shows the anchor marker which is highly visible and demonstrates proper anchoring. Frameless IUDs or IUS have many advantages as they fit in cavities of every size and shape and will adapt to the uterine cavities during involution of the postpartum uterus due to their small and flexible design (Figure 2a and Figure 2b).
![Figure 2: A) Hysteroscopic view of the frameless copper IUD. B) Hysteroscopic view of the frameless LNG-IUS. Note the compatibility of the devices with the uterine cavity. Anchoring of frameless design IUDs, which lack conventional cross arms, to the fundal wall of the uterus has been medically and commercially available throughout Europe for many years in the form of GyneFix® (Control Research, Belgium). Multiple clinical trials demonstrated the anchoring technique to bea valid concept [12]. Upon insertion of the device, the copper ions are released from the outside as well as from the inside of the copper cylinders, generating high copper ion release. The copper ions will spread throughout the genital tract and fallopian tubes, preventing fertilization and ectopic pregnancy. The 10-year frameless IUD was found to be as effective as tubal sterilization [12]. Due to its long duration of action it could be positioned as a reversible alternative to tubal sterilization which is particularly interesting in postpartum women.](/fulltextimages/395/fig_2.jpeg)
Figure 2: A) Hysteroscopic view of the frameless copper IUD. B) Hysteroscopic view of the frameless LNG-IUS. Note the compatibility of the devices with the uterine cavity. Anchoring of frameless design IUDs, which lack conventional cross arms, to the fundal wall of the uterus has been medically and commercially available throughout Europe for many years in the form of GyneFix® (Control Research, Belgium). Multiple clinical trials demonstrated the anchoring technique to bea valid concept [12]. Upon insertion of the device, the copper ions are released from the outside as well as from the inside of the copper cylinders, generating high copper ion release. The copper ions will spread throughout the genital tract and fallopian tubes, preventing fertilization and ectopic pregnancy. The 10-year frameless IUD was found to be as effective as tubal sterilization [12]. Due to its long duration of action it could be positioned as a reversible alternative to tubal sterilization which is particularly interesting in postpartum women.
Conflict of Interest
Dirk Wildemeersch has conducted research in the field of non-hormonal and hormonal, framed and frameless intrauterine devices, including in nulliparous and adolescent women, for 30 years. Norman Goldstuck conducted research in intrauterine device use, including adolescents, for over 30 years.
References
-
Bujold E, Gauthier RJ (2010) Risk of Uterine Rupture Associated with an Inter delivery Interval Between 18 and 24 Months. Obstet Gynecol 115(5): 1003-1006. B
-
Zhang H, Fang G, Zhou C (2004) Study on GyneFix PP IUD insertion during cesarean section. Chinese Journal of Family Planning 12(8): 481-482.
-
Bahamondes L, Bahamondes MV, Modesto W, Tilley IB, Magalhães A, et al. (2013) Effect of hormonal contraceptives during breastfeeding on infant's milk ingestion and growth. Fertil Steril 100(2): 445-450.
-
Elsedeek MSE (2015) Five-year follow-up of two types of contraceptive device fitted during elective cesarean delivery. Int J Gynaecol Obstet 130(2): 179- 182.
-
Kapp N, Curtis KM (2009) Intrauterine device insertion during the postpartum period: a systematic review. Contraception 80(4): 327-336.
-
Chi IC, Wilkens LR, Rogers S (1985) Expulsions in immediate postpartum insertions of Lippes Loop D and Copper T IUDs and their counterpart Delta devices--an epidemiological analysis. Contraception 32(2): 119-134.
-
Goldstuck ND, Steyn PS (2013) Intrauterine contraception after cesarean section and during lactation: a systematic review. Int J Womens Health 5: 811-818.
-
Thiery M, Van Kets H, Van der Pas H (1985) Immediate postplacental IUD insertion: The expulsion problem. Contraception 31(4): 331-349.
-
Çelen S, Sucak A, Yıldız, Danışman N (2011) Immediate postplacental insertion of an intrauterine contraceptive device during cesarean section. Contraception 84(3): 240-243.
-
El-Minawi MF, Foda MS (1971) Postpartum lactation amenorrhea: endometrial pattern and reproductive ability. Am J Obstet Gynecol 111(1): 17-21.
-
Wildemeersch D, Goldstuck ND, Hasskamp T (2016) Current status of frameless anchored IUD for immediate intracesarean insertion. Dev Period Med 20(1): 7-15.
-
Wildemeersch D, Pett A, Jandi S, Hasskamp T, Rowe P, et al. (2013) Precision intrauterine contraception may significantly increase continuation of use: a review of long-term clinical experience with frameless copper-releasing intrauterine contraception devices. Int J Women’s Health 5: 215- 225.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’