Morning Glory Syndrome: A Case Report
Introduction: Morning Glory Syndrome is a congenital anomaly of the papilla. It is uncommon, and can be isolated or associated with other ocular or general malformations. The aim of this observation was to report the first case of Morning Glory Syndrome in Côte d'Ivoire associated with hypertelorism and agenesis of the nasal pyramid. Observation: we present an 8-year-old male child with no particular history admitted in consultation for exotropia of the left eye that had been developing for 6 months. On examination, the left eye had a visual acuity reduced to a luminous perception and had a normal anterior segment. In the eye fundus, there was a large papilla excavated in the center, partly filled by a glial proliferation with a raised ring of pigments around the excavation and an abnormal disposition of the vessels, evoking Morning Glory Syndrome. The right eye was unremarkable. The examination of the oculomotricity revealed an intermittent exotropia of the left eye. In addition, there was hypertelorism, nystagmus in the left eye and agenesis of the nasal pyramid. Discussion: Morning Glory Syndrome is an uncommon congenital disorder characterized by a widely enlarged papilla, pink-orange in color, with a small glial tuft in the center. The retinal vessels are arranged radially in relation to the papilla. A pigmented ring surrounds the excavation. The incidence is not well known. It is generally unilateral. It is discovered in children most often on the occasion of visual impairment, nystagmus, strabismus and, more rarely, leukokoria. However, in some cases, the discovery may be fortuitous in case of systematic clinical examination in children or adults. Conclusion: This papillary anomaly requires the search for associated general and / or ocular malformations. Surveillance is necessary given retinal detachment risk. Early screening followed by a management in a better time of organic abnormalities of the optic nerve is also essential in order to avoid deep amblyopia.
Introduction
Morning Glory Syndrome is an uncommon congenital anomaly of the papilla. It is characterized by a strongly enlarged papilla, pink-orange in color, with a small glial tuft in the center. The retinal vessels are arranged radially relative to the papilla. A pigmented ring surrounds the excavation [1]. The anomaly is generally unilateral and associated with a deep amblyopia [1]. The diagnosis can be made from strabismus, amblyopia, nystagmus and more rarely in the presence of leukokoria [2]. Morning Glory Syndrome may be accompanied by other anomalies of the central nervous system, endocrine, renal, respiratory anomalies, or anomalies of elements of the acronym CHARGE. Children with Morning Glory Syndrome sometimes have median malformations of the face, including hypertelorism, and anomalies in the base of the nose [3]. The aim of this observation was to report a case of Glory Morning Syndrome associated with hypertelorism and agenesis of the nasal pyramid and to remind the importance of early screening of the organic anomalies of the optic nerve in order to avoid deep amblyopia by a management in a better time.
Observation
We present an 8-year-old male child with no particular history admitted in consultation for exotropia in the left eye, which has been developing for 6 months. On examination, the right eye was strictly normal. The left eye had a visual acuity reduced to a luminous perception. Its anterior segment was normal. The ocular tonus was 11mmHg. The examination of the eye fundus revealed a large papilla excavated in its center, partially filled by a glial proliferation with a raised ring of pigments around the excavation and an abnormal disposition of the vessels evoking a congenital malformation of the papilla in Morning Glory Syndrome. The peripheral retina and macula are normal. The study of refraction after instillation of cyclopentolate drops gave the following results: in the right eye, +1 D and in the left eye, (20-5) - 9.5 D. The examination of oculomotricity revealed an intermittent exotropia in the left eye. At the cover test, a fixation movement towards the temple was objectified. The study of corneal reflection has reported a nasal asymmetry. In addition, nystagmus in the left eye, hypertelorism and agenesis of the nasal pyramid were noted (Figure 1).

Figure 1: An 8-year-old child with hypertelorism and agenesis of the nasal pyramid. A review was carried out to specify the characteristics of this malformation and to search for other pathologies associated with it. Retinophotography confirmed a large papillary excavation surrounded by pigment rearrangement (Figure 2). To retinal angiography with fluorescein, the red-free clichés objectified the same results as those of Retinophotography. The retinal vessels originate from the periphery of the papilla after injection of fluorescein (Figure 3). The macula and the rest of the retina showed no anomaly.
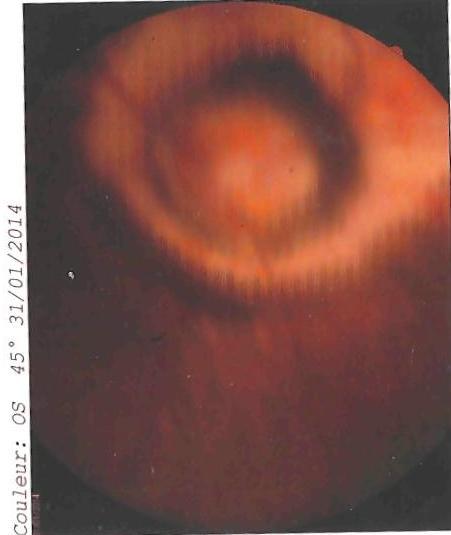
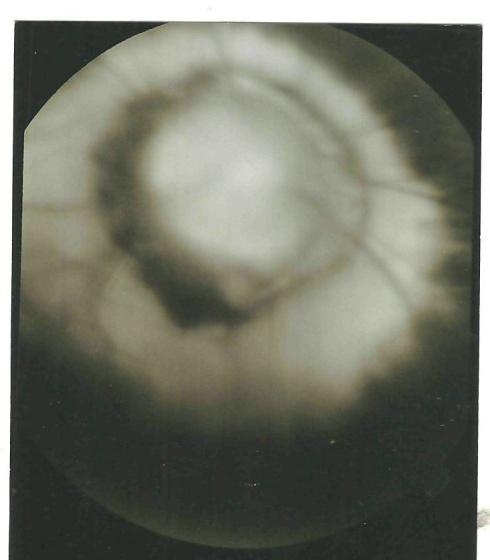
Figure 3: Large papilla, large pigmented ring, important excavation with abnormal disposition of the vessels evoking Morning Glory Syndrome to the retinal angiography with fluoresce in of the left eye. The orbito cerebral CT scan showed no other anomaly on the path of the optic nerve and the cerebral parenchyma. The optic chiasm was normal. At the end of this review, we concluded that it was Morning glory syndrome associated with hypertelorism and agenesis of the nasal pyramid.
Discussion
Morning Glory Syndrome is part of the group of congenital anomalies of the optic nerve. Its first description was made by Reis and then taken over by Handmann, hence the name "Handmann anomaly" until 1970 [4, 5]. It is Kindler who, the first named it after the English name of Morning Glory, because of a similarity of form [6]. This syndrome is uncommon. It is predominant in girls with a sex ratio of 2/1 [2, 7, 8]. Its incidence remains unknown [9]. Nevertheless, it occurs less frequently in the black population [3]. It is, as a general rule, unilateral [2, 7, 8]. However, bilateral cases have been described. Nagy observed two bilateral cases of Morning Glory Syndrome in a mother and her daughter [10]. De Laey also reported 4 bilateral cases [11]. Typically, Morning Glory Syndrome is characterized by a strongly enlarged papilla, orange-pink in color, with a small glial tuft in its center. The retinal vessels are numerous, fine, and arranged radially relative to the papilla. The papilla is surrounded by an irregularly pigmented excavation [1]. There are many clinical forms. Contractile forms have already been reported, where contraction movements of the papilla sometimes occur, causing a fleeting amaurosis [3, 7, 8]. Their movements could be explained by the presence of heterotopic tissue of smooth muscle fibers located in the choroid, at the origin of the contraction [7, 12]. In addition, the pulsatile nature was due to the flux and reflux of sub-arachnoid fluid that would be made possible by abnormal communication between the retinal and sub-arachnoid spaces [7]. Sugar also suggested the existence of a relationship between the mechanism and the variation of the venous pressure during respiration [13]. Other clinical forms with vascular anomalies have been described [7]. Yamana reported cases of macular aplasia in patients with Morning Glory Syndrome [14]. Its discovery usually occurs before amblyopia; strabismus and nystagmus. This was the case of our observation where the child was admitted for exotropia, nystagmus and vision loss in the left eye. Anomalies of refraction were often seen in the form of myopia, hyperopia and astigmatism. Our observation also showed the same anomalies of refraction except for hyperopia. Visual acuity is generally less or equal to 1/10 and not improvable [15]. In our case, the patient has a visual acuity restricted to a luminous perception. However acuities of 10/10 have been reported [16]. Loudot observed a visual acuity recovery of 7/10 after functional rehabilitation in a 2 ½-year-old child with Morning Glory Symptom with exotropia and unilateral severe amblyopia [3]. This implies that an attack treatment by occlusion is necessary in all cases of asymmetric or unilateral anomalies of the optic nerve, because a functional part is often associated with the organic part in organic amblyopia. The pathogenesis of Morning Glory Symptom is controversial. Schneider, first considered it as a particular form of coloboma where the colobomatous defect is central and due to an anomaly of closure of the embryonic fissure [7]. A pathological study by Mauschot showed the absence of a solution of continuity between the retinal pigment epithelium and the inner limit of the papilla, thus demonstrating that there is no neuroectodermal closure defect [12]. In his opinion, Morning Glory Syndrome is a mesodermal congenital lesion and not a coloboma of the optic nerve. In addition, Pollock suggested that Morning Glory Symptom is a primary mesenchymal anomaly resulting from the defective closure of the scleral posterior wall and the poor development of the cribriform plate [3]. As for Mohamed, it may sometimes be hereditary [16]. Thus Nagy described a case of Morning Glory Syndrome in a mother and her daughter [10]. Genetic predisposition remains uncertain [10]. Nevertheless, mutations in the PAX6 gene have been associated with Morning Glory Syndrome [8]. Morning Glory Syndrome is usually isolated [3]. However, it may be accompanied by basal encephalocele. Children with Morning Glory Syndrome also run the risk of developing respiratory, endocrine and neurological disorders. Sometimes, they present median transformations of the face, with hypertelorism and anomaly of the base of the nose, palate and anterior part of the base of the skull, sometimes even a hypothalamic-pituitary hernia. 1/3 of patients have no chiasma [3]. In 75% of cases, the transphenoidal encephalocele is accompanied by agenesis of corpus callosum [3]. Associations with Moya-Moya disease, CHARGE syndrome, sella turcica anomaly, trisomy 4q and some cases of type 2 neurofibromatosis have been reported [3, 7, 11, 17]. We present in our case an 8-year-old child with a unilateral Morning glory syndrome associated with hypertelorism and agenesis of the nasal pyramid. This association with the agenesis of the nasal pyramid could be the first case described in the literature, which makes our observation unique. The malformation could be complicated by retinal detachment in about 30% of cases. The pathogenesis of these detachments is controversial. Conventionally, these retinal detachments are considered to have a non-rhegmatogenic origin and more rarely a rhegmatogenic origin. Thus, the discovery of a case of Morning Glory Syndrome should be the subject of a regular monitoring, a multidisciplinary management, a complete clinical examination and a thorough morphological assessment.
Conclusion
Morning Glory Syndrome is an uncommon congenital anomaly of the papilla. Its diagnosis requires the search for other associated malformations. Surveillance is necessary given retinal detachment risk. Early diagnosis followed by a management of organic congenital abnormalities of the optic nerve, is essential in order to avoid deep amblyopia.
References
-
Plant GT, Kermode AG, Turano G, Moseley IF, Miller DH, et al. (1992) symptomatic retrochiasmal lesions in multiple sclerosis: clinical features, visual evoked potentials, and magnetic resonance imaging. Neurology 42(1): 68-76.
-
Loudot C, Fogliarini C, Baeteman C, Mancini J, Girard N, et al. (2007) Rehabilitation on functional amblyopia in Morning Glory Syndrome. J Fr Ophtalmol 30(10): 998-1001.
-
Pollock S (1987) The Morning glory disc anomaly: contractile movement, classification, and embryogenesis. Doc Ophtalmol 65(4): 439-460.
-
Reis W (1908) Eine wenig bekannte typische Missbildung am Sehnerveneintrit: umschriebene Grubenbildung auf der Papille n.optici. Z Augenheilkd 19: 505-528.
-
Kindler P (1970) Morning glory syndrome: unusual congenital optic disc anomaly. Am J Ophthalmol 69(3): 376-384.
-
Handmann M (1929) Erbliche, vermutlich angeborene, zentral gliose Entartung des Sehnerven mit besonderer Beteiligungder Zentralgefasse. Klin Monatsbl Augenheilkd 83: 145-52.
-
Schneider C, Cayrol D, Arnaud B, Schmitt Bernard CF (2002) Forme Clinique de l’anomalie papillaire en fleur de liseron ou Morning glory syndrome. J Fr Ophtalmol 25(2): 178-181.
-
Ahmet A, Gulengul A, Sevda AK, Osman OO, Suat FA (2014) Unilateral morning glory optic disc anomaly in a case with Down syndrome. BMC Ophtalmology 14: 48-53.
-
Rashida S, Memuna B (2010) Morning glory syndrome. DJO 21: 45-47.
-
Nagy V, Kettesy B, Toth K, Vamosi P, Damjanovich J, et al. (2002) Morning glory syndrome-a clinical study of two case. Klin monbl Augenheikd 219(11): 801-805.
-
De Laey JJ, Ryckaert S, Leys A (1985) the Morning glory syndrome. Ophtalmique Paediatr Genet 5(1-2): 117-124.
-
Muchot WA (1990) Morning glory syndrome: a histopathological study. Br J Ophtalmol 74(1): 56-58.
-
Sugar HS, Beckman H (1969) Peripapillary staphyloma with respiratory pulsation. Am J Ophthalmol 68(5): 895-897.
-
Yamana T, Nishimura M, Ueda K, Chijiiwa T (1983) Macular involvement in Morning glory syndrome. Jpn J Ophthalmol 27(1): 201-209.
-
Brodsky MC (1994) Congénital optic disk anomalies. Surv Ophtalmol 39(2): 89-112.
-
Mohand MS, Bouazizt, Juvespan M (2002) Morning glory syndrome: à propos d'une observation. J Fr Ophtalmol 90-99.
-
Ping F, Qi Z, Jing L, Peiquan Z (2013) Clinical characteristics and treatment of 22 eyes of morning glory syndrome associated with persistent hyperplastic primary vitreous. Br J Ophthalmol 97(10): 1262-1267.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report