Superior Oblique Palsy
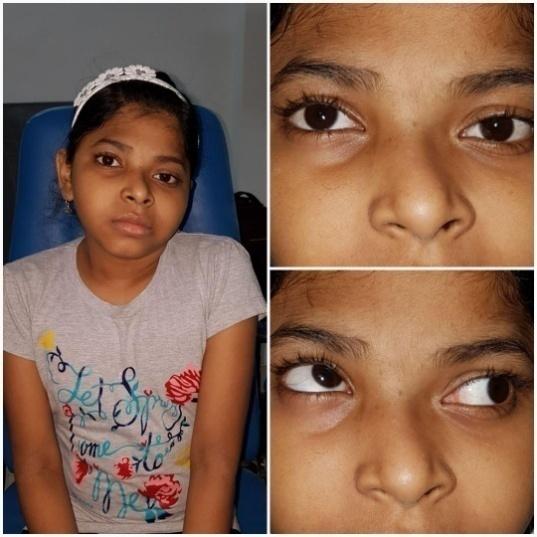
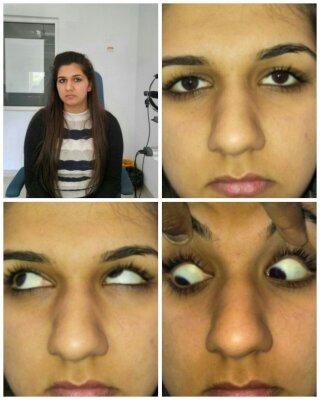
Superior Oblique muscle is innervated by the trochlear nerve. It can be congenital or acquired (traumatic, inflammatory, infectious or following sinus surgery). Damage to trochlear nerve can occur in the dorsal midbrain, cavernous sinus, superior orbital fissure and the orbit. Superior oblique is an intorter, depressor and abductor. Palsy of the muscle causes hypertropia, excyclotropia, esotropia and abnormal head postures including head tilt and face turn to the contralateral side. Facial asymmetry (shallowing of the mid facial region between the lateral canthus and the edge of the mouth) is a characteristic sign of congenital superior oblique palsy
Mini Review
Superior Oblique muscle is innervated by the trochlear nerve. It can be congenital or acquired (traumatic, inflammatory, infectious or following sinus surgery). Damage to trochlear nerve can occur in the dorsal midbrain, cavernous sinus, superior orbital fissure and the orbit. Superior oblique is an intorter, depressor and abductor. Palsy of the muscle causes hypertropia, excyclotropia, esotropia and abnormal head postures including head tilt and face turn to the contralateral side. Facial asymmetry (shallowing of the mid facial region between the lateral canthus and the edge of the mouth) is a characteristic sign of congenital superior oblique palsy. The diagnosis of SO palsy can be confirmed by a positive Park-Bielschowsky 3-step test. V pattern esotropia with chin down position suggests the possibility of a bilateral SO palsy and is confirmed by the presence of a large excyclotorsion (>15 PD) on fundus examination. Double Maddox rod is used to check the degree of cyclo- deviation while alternate prism cover test measures the degree of hyper deviation. Abnormalities in version movements include ipsilateral SO underaction, ipsilateral IO overaction and contralateral SO overaction (due to ipsilateral SR restriction). Inhibitional palsy of the contralateral superior rectus can also be seen [1, 2, 3, 4, 5]. Differential diagnosis of SO palsy include skew deviation, primary inferior oblique overaction, thyroid orbitopathy and brown syndrome. Knapp classified SOP according to a grading system based on the gaze position or positions of greatest vertical misalignment: Class I: Hypertropia worse on adduction and upgaze Class II: Hypertropia worse on adduction and downgaze Class III: Hypertropia worse on abduction Class IV: Hypertropia worse on abduction and downgaze Class V: Hypertropia worse on downgaze abduction/adduction Class VI: Bilateral SO palsy Class VII: Traumatic palsy combined with Brown's syndrome
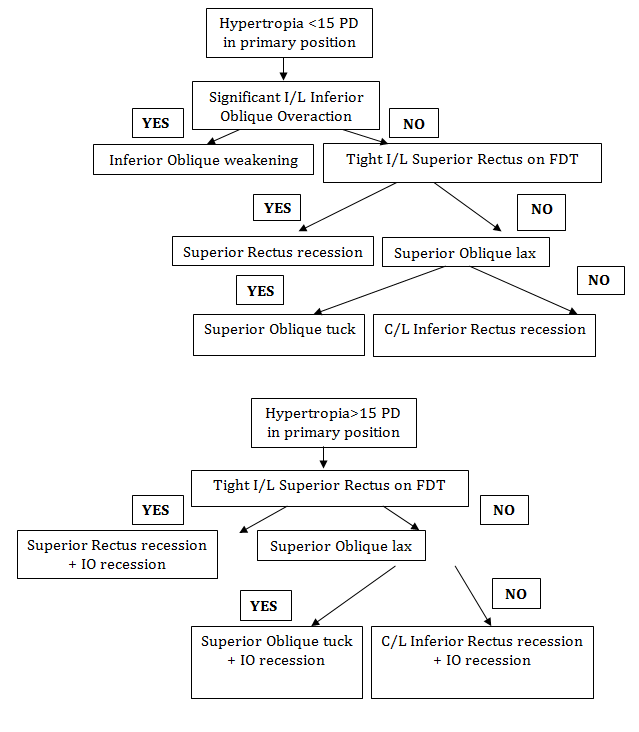
Management
Non surgical management-Prisms can be given to patients with small hyperdeviations.


References
-
Robb RM (1990) Idiopathic superior oblique palsies in children. J Pediatr Ophthalmol Strabismus 27(2): 66-9.
-
Phillips PH, Hunter DG (1999) Evaluation of ocular torsion and principles of management. Clinical Strabismus Management, Rosenbaum AL, Santiago AP (Eds.), WB Saunders, 52-72.
-
Plager DA (1999) Superior oblique palsy and superior oblique myokmia. Clinical Strabismus Management: Principles and Surgical Techniques 5: 219-229.
-
Sharma P (2013) Strabismus Simplified, 2nd (Edn.), CBS Publishers New Delhi.
-
Knapp P, Moore S (1976) Diagnosis and Surgical options in Superior oblique surgery. Int Ophthalmol Clin 16(3): 137-149.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report