Overview of a Screening Camp in Rural Area of Nepal-A Camp Report
Background: Organizing and participating in camps have been an integral part of health services, especially in developing countries like Nepal. Hospital service and specialist care are still out of reach of many people. Still many patients wait in free camps for the treatment of their diseases. Health Camp content is focused on improving or extending the efficacy of health care by embracing social networks, open standards, and the latest web and mobile technologies. With existing and limited resources too, with full community participation also we can serve the community and this is the main theme of organizing health camps. Methods: Two days health camp was conducted on October 21st and 22nd, 2019. The camp was organized at Nagre-Rajbash of Kavre District, Nepal. Examination procedures included visual acuity testing, anterior segment evaluation, retinoscopy and subjective refraction and Fundoscopy. Also, color vision testing, fluorescein staining and dilating procedures were performed in necessary patients. Results: Total number of patients seen in the camp was 252. There were 155 female patients and 97 male patients for eye examination. Most of the patients aged over 50. 122 cases had refractive error excluding presbyopia. Astigmatism was the most common refractive error followed by myopia. 25 cases had unilateral or bilateral mature cataracts, 82 cases had unilateral or bilateral immature cataracts, 26 cases had conjunctivitis (infective and allergic), and 31 cases had pterygium. Conclusion: Screening camps in rural area are very important community tools for early detection and proper referral and management of ocular morbidities. Making the community participate in such screening camps takes off a load of huge numbers of skilled and trained human resources in underdeveloped and developing countries like Nepal. Concerned authorities should keep this fact and advantage of screening camps on mind and always promote screening camps in rural areas where health facilities are difficultly achievable.
Raju Kaiti1*, Ranjila Shyangbo2 and Indra Prasad Sharma3
Keywords: Screening camps; Refractive error; Cataract; Vision Screening; Volunteers
Background
Organizing and participating in camps have been an integral part of health services, especially in developing countries like Nepal [1]. Hospital service and specialist care are still out of reach of many people. Still many patients wait in free camps for the treatment of their diseases. There are geographical, social, and economical hindrances for easy access to health services. Nepal is among the world’s poorest countries, ranking 148th out of 189, with a Human Development Index (HDI) score of 0.574 in 2019. Challenging geography, civil unrest and a lack of infrastructure complicate efforts to improve livelihoods, establish functioning markets and transport food [2]. Of the people living in Nepal, 25% are living below the poverty line, on 50 cents per day [3]. Frequent natural disasters like earthquakes and floods are especially devastating to families with few resources to protect themselves and recover. Unemployment and underemployment significantly contribute to poverty rates in Nepal. In 2016, the unemployment rate was around 3.4%. Lack of well-paying jobs is a major contributor to poverty [3].
Health Camp content is focused on improving or extending the efficacy of health care by embracing social networks, open standards, and the latest web and mobile technologies. With existing and limited resources too, with full community participation also we can serve the community and this is the main theme of organizing health camps.
Eye care service is no different story from other health services. Eye screening camps are the most demanded and mostly attended camps compared to other departments in combined camps. Many screening camps and surgical camps are arranged throughout the years in our country. Many patients get benefits from the medicines, spectacles and surgical procedures.
Methodology
A two days health camp was conducted on October 21st and 22nd, 2019. The camp was organized at Nagre-Rajbash of Kavre District, Nepal with the support of local club and local community (Figure 1).

Our Medical team consisted of two optometrists, two medical officers, one dental hygienist, two staff nurses, two pharmacists, one lab technician, one health assistant and one consultant Physician. All necessary medicines: lubricating, antibiotics (drops and ointments), anti-inflammatory, anti- allergic, mild steroids, anesthetic drops and mydriatics were arranged by the organizing group. Ophthalmoscope, retinoscope, handheld slit lamp, occluder, fixation target, torch light, fluorescein strip, trial set, vision charts (Snellen’s chart, Kay Picture chart and Sheridan Gardiner chart), and Ishihara chart were arranged for ocular examination.
Examination procedures included visual acuity testing (as per the co-operation level of the patient), anterior segment evaluation (with torch light and handheld slit lamp), retinoscopy and subjective refraction for near and distance and Fundoscopy (with an ophthalmoscope). Also, color vision testing, fluorescein staining and dilating procedures were performed in necessary patients. After examination, spectacles were prescribed and distributed as per necessity; required medications were prescribed and proper counseling and appropriate referrals were made for surgeries and further managements. Free surgeries were managed for the required patients in the nearby hospital, where we worked.
The following criteria were used to classify the refractive error [4]. a) Hypermetropia: If refractive error is of magnitude ≥+0.50 D. Hypermetropia was further classified into low hypermetropia (>+0.50D to <+ 3.0D), moderate hypermetropia (>+3.0 D to <+6.0D) and high hypermetropia (>+6.0D). b) Myopia: If refractive error is of magnitude ≥-0.50D. Myopia was further classified into low myopia (>-0.50D to <-3.0D), moderate myopia (>-3.0D to <-6.0D) and high myopia (>- 6.0D). c) Astigmatism: any cylindrical error ≥±0.5. Astigmatism was further classified into simple myopic astigmatism, simple hyperopic astigmatism, compound hypermetropic astigmatism, compound myopic astigmatism and mixed astigmatism.
Astigmatism was further classified as “with the rule” when myopic astigmatism had axis at 180±30 degrees or hypermetropic astigmatism had axis at 90±30 degrees and “against the rule” when myopic astigmatism had axis at 90±30 degrees or hypermetropic astigmatism had axis at 180±30 degrees. If the axis of astigmatism was within >30 to <60 or >120 to <150 degrees, it was considered as oblique astigmatism.
Visual impairment secondary to uncorrected refractive error was classified according to the presenting visual acuity which might be the uncorrected (visual acuity in uncorrected refractive error) and corrected (visual acuity with present correction in patients using spectacle). Visual impairment was further [5] classified as: a) NormalVision-20/10-20/25 b) Mild Visual Impairment- 20/28-20/60 c) Moderate Visual Impairment- 20/70 – 20/160 d) Severe Visual Impairment- 20/200- 20/400 e) Profound Visual Impairment – 20/500-20/1000 f) Near Total Visual Impairment - < 20/1000 g) Total Visual Impairment – No light Perception Visual acuity for the classification of visual impairment was taken of better eye with best correction. Data was entered and analyzed on SPSS 21 version.

Results
Total number of patients with ocular complaints was 252. There were 155 female patients and 97 male patients for eye examination. Most of the patients aged over 50. Pediatric patients were less in number than expected. There were 21 pediatric patients; 44 patients were of age more than 16 and less than 40 years; 187 patients were above 40 years. Most of the patients had refractive error as their ocular morbidity followed by cataract.

122 (244 eyes) cases had refractive error excluding presbyopia, for which they were prescribed and distributed spectacles. Astigmatism was the most prevalent refractive error (50.82%, N= 244) followed by myopia 43.44%, N=244). Among 187 presbyopic cases, 127 cases were in need of presbyopic corrections. 25 cases had unilateral or bilateral mature cataracts which needed surgery. They were counseled and referred for cataract surgery. 82 cases had unilateral or bilateral immature cataracts for which counseling was done and refractive correction was advised (Tables 3 & 4).
| Age Group | Number of Patients |
|---|---|
| Less than 16 years | 21 |
| 16-40 years | 44 |
| Greater than 40 years | 187 |
| Total | 252 |
Table 1: Distribution of patients as per age group.
| Refractive Error | No. of Eyes | Percentage |
|---|---|---|
| Myopia | 106 | 43.44 |
| Astigmatism | 124 | 50.82 |
| Hypermetropia | 14 | 5.74 |
| Total | 244 | 100 |
Table 2: Distribution of refractive error.
| Refractive Error Subtypes | No. of eyes | Percentage (N=244 eyes) |
|---|---|---|
| Mild Myopia | 52 | 21.31 |
| Moderate Myopia | 36 | 14.75 |
| High Myopia | 18 | 7.38 |
| Mild Hypermetropia | 8 | 3.28 |
| Moderate Hypermetropia | 5 | 2.05 |
| High Hypermetropia | 1 | 0.41 |
| Simple Myopic Astigmatism | 31 | 12.7 |
| Compound Myopic Astigmatism | 64 | 26.23 |
| Simple Hypermetropic Astigmatism | 8 | 3.28 |
| Compound Hypermetropic Astigmatism | 16 | 6.56 |
| Mixed Astigmatism | 5 | 2.05 |
Table 3: Distribution of subtypes of refractive error.
| No. of eyes | Percentage (N=124 eyes) | |
|---|---|---|
| With the Rule | 49 | 39.52 |
| Against the Rule | 59 | 47.58 |
| Oblique Astigmatism | 16 | 12.9 |
| Total | 124 | 100 |
Table 4: Distribution of astigmatism.
Mild form of myopia was the most common myopic subtype (21.31%, N=244 eyes) and compound myopic astigmatism was the most prevalent type of astigmatism (26.23%, N=244 eyes). Against the rule astigmatism was found in 47.58% (N=124 eyes).
26 cases had conjunctivitis (infective and allergic) and medications were prescribed for them. 31 cases had pterygium; 3 cases were counseled and referred for pterygium excision and rest of cases were counseled and managed with medications. There were also cases of receded NPC (Near Point of Convergence), 12 cases of receded NPC were counseled and taught pencil push up exercise (as a home-based convergence therapy). There was one case of alternate exotropia. These cases were called for detail orthoptic evaluation as suspected Convergence Insufficiency. 2 glaucoma suspects were referred for further evaluation to the hospital. Many corneal problems, including corneal ulcers, opacities and dystrophies were examined. Necessary medications and proper counseling with referrals were made according to the cases. 3 cases didn’t have any significant ocular findings. Few cases were dilated to look for any diabetic and hypertensive changes in fundus. There was a case of disc pallor and few cases of diabetic retinopathies, which were referred to tertiary eye care centres. 2 cases of chronic dacryocystitis were counseled and posted for DCR surgery. 2 amblyopic cases were also counseled and referred for further evaluation and management ( Figure 4).
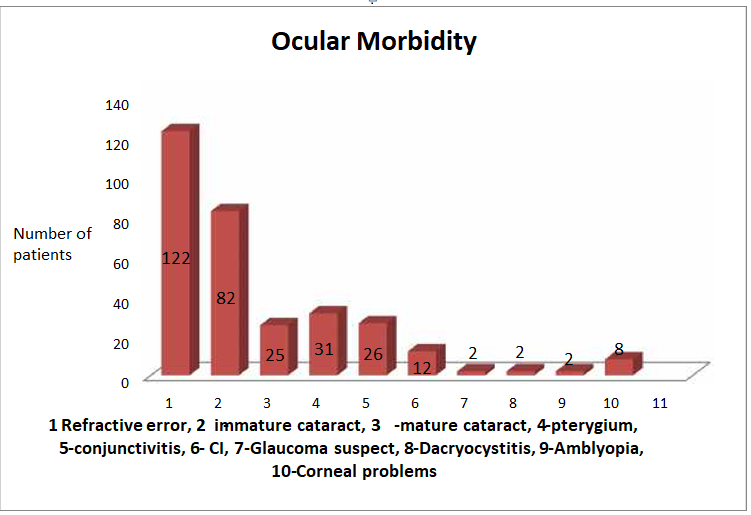
This bar diagram shows the ocular morbidity pattern found in the camp (Figure 5). Some of the patients had more than one diagnosis, so the number of patients shown here exceeds the total number of patients seen in the camp.
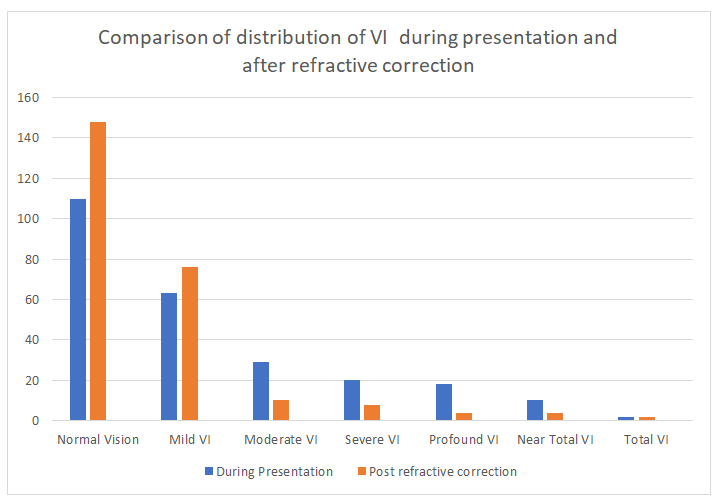
Above bar diagram clarifies the importance of refractive correction. After refractive correction, the bar of normal vision improved from 110 to 148, number of people increased from 65 to 76 in mild Visual Impairment group. It also shows subsequent reduction in number of patients in moderate, severe, profound and near total VI. Total of 31 cases were referred for surgeries. 25 cases for cataract, 3 for pterygium, 2 for Dacryocystorhinostomy (DCR) and one Oculoplasty case. All these cases will be examined in tertiary eye hospital for preoperative evaluations and will be posted for surgeries. Short lectures with demonstrations on ocular first aids, ocular hygiene procedures and DO’s and DON’Ts for the eyes were also conducted after the screening camp. We trained 10 school students on visual acuity testing and provided them with Snellen’s charts. They will take visual acuity and record them. Patients and students with reduced visual acuity will be sorted and referred for further management.
Discussion
Under developed and developing countries lack skilful manpower and thus can’t reach all people around the country. Basically, people in rural areas suffer a lot. Nepal is not an exception1. Like in many other screening camps, the participation was as expected. Still the village areas of developing countries like Nepal wait for screening camps to get free medicines, spectacles and surgeries. They don’t have enough health centres and medical personnel. Looking at the prevalence of refractive error (uncorrected), we can easily conclude how they are living. They can’t even get a near add which merely costs about 200 NRs. Astigmatism (50.82%, N=244 eyes) was the most common type of refractive error followed by myopia (43.44%, N=244 eyes). This finding was similar to the study done by Kaiti R, et al [4].
The number of mature cataracts in that small community is also alarming. Here, refractive error and cataract together constitute more than 80% of treatable and curable visual impairment. This highlights the importance of screening camps. Community participation is a must for mass screening with limited resources [6]. Vision screening and eye examinations create frequent and early opportunities to diagnose a myriad of conditions [6]. Programs like little optometrist program are introduced in Nepal to make the community participate for their own ocular health [1]. School students, teachers and even locals can be made aware, responsible and trained for ocular examination and their proper referral and management. There are about 123.7 million people with visual impairment secondary to uncorrected refractive errors that can affect their learning development [7, 8]. Many research works and practical evidences have shown that these visual deficits can be identified through visual acuity testing. Timely identification and affordable treatments to correct vision can improve the quality of life of the population [9]. Many studies suggest that vision screening of children is beneficial [10, 11]. The inclusion of visual health in a school’s curriculum can contribute to the development of a healthy school environment, promote good vision habits and permit the detection of eye problems, facilitating the integration of boys and girls with visual disability into the classroom [12]. Some studies also confirmed that trained schoolteachers are a valid resource for the identification of vision deficits in school children [9].
Conclusion
Screening camps in rural areas are very important community tools for early detection and proper referral and management of ocular morbidities. Making the community participate in such screening camps take off load of huge numbers of skilled and trained human resources in underdeveloped and developing countries like Nepal. Concerned authorities should keep this fact and advantage of screening camps on mind and always promote screening camps in rural areas where health facilities are difficultly achievable. Refractive error, being the most common ocular morbidity can easily be detected and managed accordingly with minimum effort. Prevalence of visual impairment can be reduced to great extent with mere refractive correction and this can easily be done with screening camps.
References
-
Kaiti R (2017) Uncorrected Refractive Error and Associated Childhood Visual Impairment – Any new steps for prevention?. Ophthalmology and Vision Science 1(4): 167-170.
-
(2020) Newsletter-World Food Programme. cited on 2nd April, 2020.
-
Vickie Epson (2018) 10 Facts about Poverty in Nepal. The Borgen Project. cited on 2nd April, 2020.
-
Kaiti R, Pradhan A, Dahal HN, Shrestha P (2018) Pattern and Prevalence of Refractive Error and Secondary Visual Impairment in Patients Attending a Tertiary Hospital in Dhulikhel, Nepal. Kathmandu Univ Med J 62(2): 114- 119.
-
(2007) Guidelines AOCP. Care of the patient with Visual Impairment (Low Vision Rehabilitation). N. Lindbergh Blvd, St. Louis, USA: American Academy of Optometry. cited on 2nd April, 2020.
-
Shyangbo R, Kaiti R (2020) Importance of Vision Screening in Children of Developing Countries Like Nepal. EC Ophthalmology 11(4): 54-56.
-
(2018) Visual impairment and blindness. Fact sheet no. 282. cited on 2nd April, 2020.
-
Davidson S, Quinn GE (2011) The impact of pediatric vision disorders in adulthood. Pediatrics. 127(2): 334- 339.
-
Arteaga SL, Gonzalez DG, Bascaran C, Nunez RH, Morales MCP, et al. (2016) Visual health screening by schoolteachers in remote communities of Peru: implementation research, Bull World Health Organ 94(9): 652-659.
-
Baltussen R, Naus J, Limburg H (2009) Cost-effectiveness of screening and correcting refractive errors in school children in Africa, Asia, America and Europe. Health Policy 89(2): 201-215.
-
Mathers M, Keyes M, Wright M (2010) A review of the evidence on the effectiveness of children’s vision screening. Child Care Health Dev 36(6): 756-780.
-
Sharma A, Congdon N, Patel M, Gilbert C (2012) School- based approaches to the correction of refractive error in children. Surv Ophthalmol 57(3): 272-283.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report