Post Pars Plana Vitrectomy Silicone Oil Related Endophthalmitis Caused by Citrobacter Koseri: A Case Report and Literature Review
Purpose: To present a rare case of a Citrobateri koseri endophthalmitis after pars plana vitrectomy silicone oil-filled eye. Case Report: A 64-year old male patient presented to our clinic for eye pain and decrease vision in the right eye. He had a history of diabetes mellitus, hypertension, and a cataract surgery in both eyes ten years before and surgery of retinal detachment in RE For a relapse of regmatogenous retinal detachment in RE a pars plana vitrectomy with silicone oil injection was performed. He received topical betamethasone, naphazoline and tetracycline 6 times a day. After one week the patient complained ocular pain and decreased vision. Examination revealed visual acuity deterioration, a severely injected conjunctiva. The cornea was edematous with Descemet’s membrane folds. The anterior chamber was hazy with cells and flare, and hypopyon was observed. A diagnosis of post vitrectomy endophthalmitis was made. Sampling of the aqueous fluid was obtained and he was empirically treated with intravitreal ceftazidime 2.0mg/0,1ml and sub-tenon injection of betamethasone (2mg). The microscopic examination of the aqueous fluid stained with Gram stain revealed the presence of numerous polymorphonuclear cells and of small gram-negative bacteria identified as C. koseri. The strain was susceptible to all the antibiotics tested. A high MIC value (16mg/L) was detected only for tetracycline. The therapy was changed to fortified ceftazidime 5%, fortified tobramycin 0.3%, atropine 1% and prednisone-eye drops administered every 2 hours along with systemic antibiotic (ceftriaxone 2g iv for 5days) and steroid treatment without any improvement. The patient underwent to a new pars plana vitrectomy, removal of the IOL, and silicone oil exchange. In this occasion silicon leakage from previous sclerotomy, pus filled vitreous cavity and some retinal hemorrhages were observed. Vancomycin and ceftazidime according to Endophthalmitis Vitrectomy Study protocol were injected in the vitreous cavity and previous topical and systemic therapy was continued, too. An improvement of visual acuity was obtained Conclusion: Among cases of culture positive endophthalmitis, Citrobacter spp. is very rare, and this is the first report of a silicone oil related endophthalmitis caused by this microorganism.
Introduction
Silicone oil (SO) is commonly used as retinal tamponade agent after pars plana vitrectomy surgery and it is used in the surgery of complex retinal detachment, proliferative retinopathy, and viral retinitis [1, 2]. It has been demonstrated that silicone oil exhibits in vitro activity against bacteria commonly causing endophthalmitis such as Klebsiella pneumoniae, Pseudomonas aeruginosa, Staphylococcus aureus, Staphylococcus epidermidis and Bacillus cereus [3]. It is not active on anaerobic bacteria such as Propionibacterium acnes [4]. Differences in the antimicrobial activity are found when conventional and heavy silicone oil was tested, the last one showing a better efficacy [5]. The 1000 cSt SO and 5000 cSt SO showed similar fungistatic activity [6]. For its antimicrobial activity, endophthalmitis associated with its use is very rare. All the previous mentioned bacteria are commonly responsible of endophthalmitis [7, 8].
Recently, there is an increasing report of endophthalmitis caused by an unusual microorganism such as Citrobacter koseri [9]. Citrobacter is a genus belonging to the family of Enterobacterales that include Gram-negative, facultative anaerobic rods. It is widespread throughout the environment and this may reflect fecal excretion by humans and animals. C. koseri is known to cause sepsis, meningitis, pneumonia, and urinary tract infection in hospitalized patients [10]. A PubMed research of English literature using “Citrobacter koseri” and “endophthalmitis” revealed a total of six publications in the period 2008-2020 one of which dealing of C. koseri endophthalmitis [9, 11, 12, 13, 14, 15]. We described the clinical course and treatment outcome in a patient who developed post pars plana vitrectomy endophthalmitis due to C. koseri.
Case Report
A 64-year-old male patient was admitted to the emergency of Ophthalmic Department because of ocular pain and decreased vision in right eye (RE). He had a history of diabetes mellitus and hypertension. He underwent to a cataract surgery in both eyes ten years before, and also to surgery for regmatogenous retinal detachment in RE.
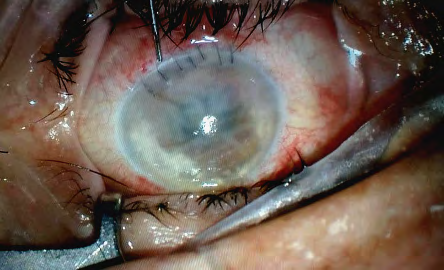
In September 2020 he had a relapse of regmatogenous retinal detachment in RE and a pars plana vitrectomy with silicone oil injection was performed. The retina was entirely reattached under 1000 cSt silicone oil. His visual acuity was 6/60. He received topical betamethasone, naphazoline and tetracycline 6 times a day. After one week the patient complained ocular pain and decreased vision. A visual acuity deterioration of hand movement for the RE was present. At slit lamp examination a severely injected conjunctiva was observed. The cornea was edematous with Descemet’s membrane folds and abundant keratic precipitates. The pupil was mid-dilated and fixed. The anterior chamber was hazy with cells and flare, and approximately 3.0 mm- height hypopyon was observed (Figure 1). The lens, vitreous and fundus were not well visualized. A diagnosis of post vitrectomy endophthalmitis was made. Sampling of the aqueous fluid was obtained by needle aspiration under topical anesthesia prior to antimicrobial therapy and sent to the Laboratory of Microbiology. Therefore, he was empirically treated with intravitreal ceftazidime 2.0 mg/0,1ml and sub- tenon injection of betamethasone (2mg).
The microscopic examination of the aqueous fluid stained with Gram stain revealed the presence of numerous polymorphonuclear cells and of small gram-negative bacteria. The sample was cultured on blood and chocolate agar, MacConckey agar and Brain Heart Infusion and incubated under aerobic conditions at 35°C. Culture on Sabauraud’ agar incubated at 30°C and culture on media for anaerobes incubated under anaerobic conditions were also performed. All plates were observed daily up to 10 days.
Colonies were identified as C. koseri by MALDI-TOF (BioMerieux, Florence, Italy). Susceptibility testing were performed by the automated system Vitek2 (BioMerieux, Florence, Italy). The strain was susceptible to the followed antibiotics: amikacin, amoxicillin/clavulanic acid, cefepime, cefotaxime, ceftazidime, ciprofloxacin, ertapenem, fosfomycin, gentamicin, levofloxacin, meropenem, tobramycin, moxifloxacin, and piperacillin/tazobactam. A high MIC value (16mg/L) was detected only for tetracycline.
Following laboratory results, fortified cefazidime 5% and fortified tobramycin 0.3%, atropine 1% and prednisone- eye drops were administered every 2 hours along with systemic antibiotic (ceftriaxone 2 g iv for 5 days) and steroid treatment. After 24 hours, a decrease in ocular pain was obtained, although the hypopyon of the anterior chamber increased slightly to 4 mm of height and corneal edema was worsened as well.
The patient underwent to a new pars plana vitrectomy, removal of the IOL, and silicone oil exchange under local anesthesia). During the surgery, silicon leakage from previous sclerotomy, pus filled vitreous cavity and some retinal hemorrhages were observed. The severe corneal edema did not allow a clear examination of the fundus. Therefore an intravitreal cocktail of vancomycin (1mg/01 ml) and ceftazidime 2.25 mg/0.1 ml according to Endophthalmitis Vitrectomy Study protocol was injected in the vitreous cavity. Previous topical and systemic therapy was continued, too.
On postoperative day 1 after vitrectomy, visual acuity was limited to light perception and intraocular pressure was normal. Slight lamp examination revealed a still edematous cornea, but no hypopyon. The posterior segment was not observed because of the presence of corneal edema. After one week, the visual acuity had improved to counting finger at 30 cm, corneal edema was decreased, and the optic disk was visible at fundus examination. After 6 weeks, the best corrected visual acuity was improved to 6/60, according to the Snellen chart examination, with refractive error sf +14 D.
Discussion
Acute endophthalmitis is a medical emergence that may result in permanent vision loss. Several kinds of microorganisms may be involved in this disease. Most cases of endophthalmitis are exogenous (via trauma or surgery) but also endogenous following to bloodstream invasion by microorganisms arising from kidney abscess although in few patients only the blood cultures were positive. The microorganisms isolated from intra ocular fluids are coagulase-negative Staphylococci (70%), S. aureus (9%), Streptococci, Bacillus spp. whereas Gram-negative bacilli account for about 6% of isolates [16].
Endophthalmitis following pars plana vitrectomy (PPVE) is uncommon and the reported rates have been decreasing over the last decade. Indeed, its incidence varies from 0.02% to 0.09% of cases [17, 18]. Silicone oil is used in particular following surgery for complex retina detachments and it has antimicrobial properties [2]. Factors that may increase the incidence of post-PPVE include inadequate wound closure, postoperative hypotony, and vitreous incarceration at a sclerotomy site, aqueous intraocular tamponade, additional concomitant intraocular procedures, and surgeon learning curve. In addition, diabetes mellitus or other causes of immune deficiency and non-compliance with treatment may represent further risk factors [7].
A good proportion of PPVE cases may have a negative culture, possibly because they were due to acute inflammatory reactions to silicone oil or to previous antibiotic therapy. Among positive culture cases, Gram- positive organisms account for 75 to 90% of cases. Gram- negative bacteria accounted for about 6% of culture positive cases. Despite its rarity, endophthalmitis caused by Gram- negative bacteria is known to have a worse prognosis than that caused by Gram positive bacteria. These positive culture cases of endophthalmitis can present with variable clinical course, the diagnosis can be delayed due to confusion from post-operative inflammation, and for low index of suspicion.
In PPVE several Gram-negative bacteria have been isolated from aqueous and/or vitreous aspirate. A case series of silicone oil related endophthalmitis due to non- usual bacteria such as Burkolderia cepacia and the most known Pseudomonas aeruginosa have been reported [19, 20]. Recently, a severe case of Proteus vulgaris PPVE has been reported. The highly purulent abscess ended up with enucleation [21].
Citrobacter spp. is very rare cause of endophthalmitis, and the case described in this paper is the first report of a silicone oil related endophthalmitis caused by C. koseri. C. koseri is a facultative anaerobic, motile, Gram negative bacillus and belongs to the genus Citrobacter, within the family of Enterobacterales. It is commonly found in water, soil and occasional colonize the skin and gut of humans. Subjects susceptible to C. koseri infections are immunocompromised patients and neonates. C. koseri has caused frequent nosocomial outbreaks of neonatal meningitis. In several instances, the outbreaks have been accompanied by high rates of intestinal colonization by the organism in infants and by carriage of the bacteria on the hands of healthcare workers. Citrobacter spp could be found in various aquatic environments and even if there are not studies on this field, we can’t rule out that, as well as reported for other gram negative such as Klebsiella, Serratia, Pseudomonas, this microorganism could colonize antiseptic solutions, hand wash and lotions as well as topical anesthetic eye drops. Infection control measures to prevent person-to-person transmission such as hand washing are the most important measures to prevent Citrobacter infections also from environmental sources [10].
The pathogenesis of Citrobacter infections has not been fully characterized. Most C. koseri isolates produce hemolysins, are piliated, and are resistant to killing by pooled human sera. Tropism for the central nervous system may be due to specific outer membrane proteins. Citrobacter koseri also has the ability to enter macrophages, survive phago-lysosomal fusion, and replicate intracellularly [22]. Recently, several genes vital for pathogenicity and which may contribute to the high degree of for the brain have been detected in C. koseri clinical strains. This includes high pathogenicity island (HPI) genes, an aerobactin biosynthetic gene cluster, a methionine-salvage related gene cluster, ABC
transporters for D-allose, ABC transporters for branched- chain amino acid, and MPC. Through in vivo animals studies the HPI cluster have been demonstrated to be essential for C. koseri pathogenicity. On the other hand, date have shown that C. koseri had less resistance genes then other species which may explain why C. koseri is more susceptible to antibiotics [23].
Few cases of C. koseri endophthalmitis have been reported. Chen KJ, et al. [15] described six cases of endophthalmitis caused by Citrobacter spp. of which two cases were caused by C. koseri. Final visual acuity was limited to no light perception in five eyes among six cases [15]. The same author reported a case of diffuse retinal vasculitis due to C. koseri in post-traumatic endophthalmitis with intraocular metal fragment have been described [13].
Another case of late-onset C. koseri infectious endophtalmitis has been reported and the source of the infection was through the exposed suture material and the bacterium may have penetrated into the eye along the exposed suture material. Thus, it is emphasized that any exposed suture material after secondary intraocular implantation or other surgical procedures must be regarded as a possible source of microorganisms causing endophthalmitis [12].
Cases of endogenous C. koseri endophthalmitis arising from renal abscess with secondary hematogenous spread to the eyes are reported. The microorganism was isolated from blood confirming an hematogenous seeding of the bacterium [9, 11, 14]. The majority of C. koseri endophthalmitis (five of six cases) are reported from South East Asian area and only one from England, Europe [9].
Like other virulent Gram-negative organism, endophthalmitis caused by Citrobacter spp can be associated with a poor visual outcome in spite of maximal treatment. Intravitreal antibiotics injection might result in a good visual outcome. Visual outcome after treatment of PPVE are varied in the literature. In general, the outcomes are worse than after cataract surgery, perhaps due to the underlying retinal pathology and associated poor visual potential. Although good visual outcomes have been reported in few patients, most large studies show poor post-treatment visual gain as in our patient. The type of gauge transconjunctival PPV does not appear to increase the occurrence of infections. There are reports of bacteria such as B. cepacia causing PPVE being the silicon oil identified to be the source of the infection and in one of the six cases presented by Chen, et al. Citrobacter freundii was isolated from corneal storage media [15].
In our case the source of C. koseri is not known. The sensitivity to all antibiotics tested except tetracycline suggests that the origin of the strain was not nosocomial.
In addition, the resistance to tetracycline may explain the failure obtained with the first topical empiric therapy with tetracycline used. Although the European Centre for Disease Control and Clinical Laboratory Standards Institute does not report Enterobacterales break points for tetracycline, the MIC of our the strain is very high (16mg/L ) suggesting that the strain was resistant.
We may assume that the bacteria have colonized the skin patient or the eye before his admission to the hospital. To the best of our knowledge, this is the first report of C. koseri causing post pars plana vitrectomy endophthalmitis. C. koseri endophthalmitis is often associated with a poor visual outcome as was the case of our patient even if the bacterium was susceptible to almost all antibiotics tested, and the therapy was begun with promptness.
Conclusion
The emergence of this rare organism as an increasingly pathogen is alarming and continuous surveillance is required on institutional level. C. koseri should be considered in the etiology of postpars plana endophthalmitis in particular in patients with risk factors such as diabetes. Early management may improve the final visual outcome, preventing the evisceration.
Ethical Standards
This study was approved by Ethical Committee of Azienda Ospedaliero-Universitaria ‘Consorziale Policlinico, Bari (No. 5877).
References
-
Lappas A, Dietlein TS, Rosentreter A, Foerster AM, Hedergott AM, et al. (2018) Vision Loss after Silicone Oil Surgery. Klin Monbl Augenheilkd 235(6): 725-729.
-
Russo A, Morescalchi F, Donati S, Gambicorti E, Azzolini C, et al. (2018) Heavy and standard silicone oil: intraocular inflammation. Int Ophthalmol 38(2): 855-867.
-
Ornek N, Apan T, Ornek K, Gunay F (2014) Antimicrobial effectiveness of silicone oil, heavy silicone oil and perfluorodecaline against Bacillus cereus. Int Ophthalmol 34(4): 859-863.
-
Arici C, Aras C, Tokman HB, Torun MM (2016) An in Vitro Experimental Study on the Antimicrobial Activity of Silicone Oil against Anaerobic Bacteria. Ocul Immunol Inflamm 24(2): 173-177.
-
Ornek N, Apan T, Ogurel R, Ornek K (2014) Comparison of the antimicrobial effect of heavy silicone oil and conventional silicone oil against endophthalmitis- causing agents. Indian J Ophthalmol 62(4): 388-391.
-
Dave VP, Joseph J, Jayabhasker P, Pappuru RR, Pathengay A, et al. (2019) Does ophthalmic-grade silicone oil possesses antimicrobial properties? J Ophthal Inflamm Infect 9(1): 20.
-
Dave VP, Pathengay A, Basu S, Gupta N, Basu S, et al. (2016) Endophthalmitis After Pars Plana Vitrectomy: Clinical Features, Risk Factors, and Management Outcomes. Asia Pac J Ophthalmol (Phila) 5(3):192-195.
-
Bhende M, Raman R, Jain M, Shah PK, Sharma T, et al. (2018) Incidence, microbiology, and outcomes of endophthalmitis after 111,876 pars plana vitrectomies at a single, tertiary eye care hospital. PLoS One 13(1): e0191173.
-
He Cong En J, Miah M, Sunkel-Laing B, Emmanuel J (2014) Endogenous endophthalmitis caused by Citrobacter koseri originating from a renal abscess. BMJ Case Rep.
-
Doran TI (1999) The role of Citrobacter in clinical disease of children: review. Clin Infect Dis 28(2): 384-394.
-
Wong DHT, Liu CCH, Tong JMK, Luk WK, Li KKW (2020) Citrobacter endogenous endophthalmitis: a case report and review of the literature. Retin Cases Brief Rep 14(2): 187-191.
-
Kang HM, Chung EJ (2011) Late-onset Citrobacter koseri endophthalmitis with suture exposure after secondary intraocular lens implantation. Korean J Ophthalmol 25(4): 285-288.
-
Chen KJ (2010) Diffuse retinal vasculitis in Citrobacter koseri traumatic endophthalmitis with intraocular foreign body. J Trauma 68(2): 504.
-
Chiu CH, Peng MY, Wang YC, Chang FY (2009) Endogenous endophthalmitis caused by Citrobacter koseri. Am J Med Sci 338(6): 509-510.
-
Chen KJ, Sun MH, Hwang YS, Chen TL, Lai CC, et al. (2008) Endophthalmitis caused by Citrobacter species. Ocul Immunol Inflamm 16(4):147-153.
-
Durand ML (2013) Endophthalmitis. Clin Microbiol Infect 19(3): 227-234.
-
Dave VP, Pathengay A, Schwartz SG, Flynn HW Jr (2014) Endophthalmitis following pars plana vitrectomy: a literature review of incidence, causative organisms, and treatment outcomes. Clin Ophthalmol 8: 2183-2188.
-
Wu L, Berrocal MH, Arevalo JF, Carpentier C, Rodriguez FJ, et al. (2011) Endophthalmitis after pars plana vitrectomy: results of the Pan American Collaborative Retina Study Group. Retina 31(4): 673-678.
-
Okonkwo ON, Hassan AO, Oderinlo O, Gyasi ME (2018) Burkholderia cepacia, a cause of post pars plana vitrectomy silicone oil related endophthalmitis: clinico- pathological presentation and outcome of management. Int J Retina Vitreous 4: 35.
-
Kannan NB, Sen S, Mishra C, Lalitha P, Rameshkumar G, et al. (2021) Ten-year trends in the incidence, clinical profile and outcomes of acute-onset endophthalmitis following combined pars plana vitrectomy and sutureless, glueless and flapless scleral fixation of intraocular lenses. Int Ophthalmol.
-
Al Kharashi AS, Al Kharshi AS, Al Faky YH (2017) Endophthalmitis Due to Proteus vulgaris after Pars Plana Vitrectomy with Devastating Outcome. Middle East Afr J Ophthalmol 24(2): 116-118.
-
Rogers L, Power K, Gaora PO, Fanning S (2016) Escherichia coli and Other Enterobacteriaceae: Occurrence and Detection. Encyclopedia of Food and Health 545-551.
-
Yuan C, Yin Z, Wang J, Qian C, Wei Y, et al. (2019) Comparative Genomic Analysis of Citrobacter and Key Genes Essential for the Pathogenicity of Citrobacter koseri. Front Microbiol 10: 2774.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report