Fitting RPG Progressive Bitoric Lenses after Bilateral Glaucoma Surgery
Glaucoma is a group of eye diseases which result in damage to the optic nerve and vision loss. Glaucoma can be divided in two groups’ open-angle and closed-angle. The importance in glaucoma disease is to treat it early because vision loss from this pathology, once it has occurred, is permanent. The main risk of factors for glaucoma includes increased pressure in the eye, a family history of the condition and high blood pressure . Generally, it is possible to treat glaucoma with laser and this treatment may be affective in both open-angle and closed-angle. A number of types of glaucoma surgeries may be used in people who do not sufficiently respond to other measure and treatment of closed-angle glaucoma is a medical emergency. After the laser treatment, if the ophthalmologist gives permission, it is possible to fit contact lenses to achieve better vision or correct patients with spectacles. This case report shows the fitting of rigid gas permeable progressive bitoric lenses after laser treatment because visual acuity achieved with spectacles was not good. Due to the intervention and patient needs, it was not possible to fit a scleral or hybrid lens.
Introduction
Glaucoma is an eye disease that damages the optic nerve causing vision loss. The most common type is open-angle glaucoma with less common types including closed-angle glaucoma and normal-tension glaucoma [1, 2, 3]. Open-angle glaucoma develops slowly over time and there is no pain and peripheral vision might begin to decrease followed by central vision resulting in blindness if not treated. Closed- angle glaucoma can present gradually or suddenly. The sudden presentation might involve severe eye pain, blurred vision, mid-dilated pupil, redness on the eye and nausea. The principal problem of glaucoma is that vision loss, once occurred, is permanent. Risk factors for glaucoma include increased pressure in the eye, a family history of the condition, and high blood pressure. For eye pressure, a value of greater than 21 mmHg or 2.8 kPa is often used with higher pressures leading to a greater risk. However, some may have high eye pressure for years and never develop damage [2, 4]. Conversely, optic nerve damage may occur with normal pressure, known as normal-tension glaucoma. The mechanism of open-angle glaucoma is believed to be slow exit of aqueous humor through the trabecular meshwork while in closed-angle glaucoma the iris blocks the trabecular meshwork. Diagnosis is by a dilated eye examination [2, 4, 5]. Often the optic nerve shows an abnormal amount of cupping. Open-angle glaucoma is painless and does not have acute attacks, thus the lack of clear symptoms make screening via regular eye check-up important. The only signs are gradually progressive visual field loss, and optic nerve changes (increased cup-to disc-ratio on funduscopic examination) [2, 4]. About 10% of people with closed angles present with acute angle closure characterized by sudden ocular pain, seeing halos around lights, red eye, very high intraocular pressure (>30mmHg), nausea and vomiting, suddenly decreased vision, and a fixed, mid-dilated pupil. It is also associated to an oval pupil in some cases [3, 5, 6]. Acute angle closure is an emergency. Opaque specks may occur in the lens in glaucoma, known as glaukomflecken. If treated early it is possible to slow or stop the progression of disease with medication, laser treatment, or surgery. The goal of these treatments is to decrease eye pressure. A number of different classes of glaucoma medication are available. Laser treatments may be effective in both open-angle and closed- angle glaucoma. A number of types of glaucoma surgeries may be used in people who do not respond sufficiently to other measures. Treatment of closed-angle glaucoma is a medical emergency [7, 8].
Screening for glaucoma is usually performed as part of a standard eye examination performed by optometrists and ophthalmologists. Testing for glaucoma should include measurements of the intraocular pressure via tonometry anterior chamber angle examination or gonioscopy and examination of the optic nerve to look for any visible damage to it, or change in the cup-to-disc ratio and rim appearance and vascular change. A formal visual field test should be performed [9, 10, 11, 12, 3]. The retinal nerve fiber layer can be assessed with imaging techniques such as optical coherence tomography, scanning laser polarimetry, and/or scanning laser ophthalmoscopy [9, 12, 3]. Owing to the sensitivity of all methods of tonometry to corneal thickness, methods such as Goldmann tonometry should be augmented with pachymetry to measure the central corneal thickness (CCT). A thicker-than-average cornea can result in a pressure reading higher than the ‘true’ pressure whereas a thinner- than-average cornea can produce a pressure reading lower than the ‘true’ pressure. Because pressure measurement error can be caused by more than just CCT (i.e., corneal hydration, elastic properties, etc.), it is impossible to ‘adjust’ pressure measurements based only on CCT measurements. The frequency doubling illusion can also be used to detect glaucoma with the use of a frequency doubling technology perimeter [8, 9]. Examination for glaucoma also could be assessed with more attention given to sex, race, history of drug use, refraction, inheritance and family history. About 6 to 67 million people have glaucoma globally. The disease affects about 2 million people in the United States. It occurs more commonly among older people. Closed-angle glaucoma is more common in women. Glaucoma has been called the “silent thief of sight” because the loss of vision usually occurs slowly over a long period of time. Worldwide, glaucoma is the second-leading cause of blindness after cataracts [2, 5, 6].
Case Report
A young man 48 years old white male came into our clinic on March 2017 with an ophthalmologist prescription for fitting contact lenses after glaucoma surgery. He was the car seller of the chief’s clinics and also a friend of us; for this reason he came to our clinic. Before coming to our clinic, he went to another eye practice under ophthalmologist advice where he was fitted firstly with scleral lenses and suddenly with RGP lenses without success. The failure in scleral lenses may be caused by the sclera form at 12 o’clock near the limbus zone after the surgery. When the ophthalmologist permitted contact lenses wear, he went to the first clinic where scleral lenses were fitted. After this trial, he was fitted with corneal toric contact lenses but he was not too much in comfort and visual acuity achieved was not so good. For these reasons and other personal motivations, he decided to stop the fitting and dropped out. Due to the failure in booth fittings, he was equipped with spectacle lenses but the patient was unhappy in comfort and vision. Probably this discomfort in visual acuity was due to the fact that the patient used to wear rigid gas permeable contact lenses instead of spectacles in the past. Probably the limited visual range of the frame could be a problem for him. Unfortunately, when he came to our clinic he had only his spectacles because he returned all the lenses he had to the previous optometrist. Spectacle lenses were: RE +3.00 -6.00 180° and LE +1.50 -6.50 170° and visual acuity achieved with this correction was not superior to 20/32 maximum. He had two pair of spectacle lenses one for distance vision and one for near vision because he began also to develop presbyopia. First thing made when he came into our clinic was to perform a detailed anamnesis about his past history in wearing contact lenses, his glaucoma history, his familiarity with eye pressure and other eye problems but also speaking with him about his life, his work and his needs in order to found the best corrective system for him. Patient told to us that he was depressed because he was sure he never could wear contact lenses again and with spectacles lenses it was too much difficult work and drive cars. Due to this depression, he went also to psychological sessions because he was afraid to lose his work because he was a car seller and also he never could see his child grow up like a normal person. Speaking with him it was clear that he needed good visual acuity and it was decided to try again with RGP corneal lenses.
He told that between November and December 2016 he was operated with extreme urgency of acute closed-angle glaucoma, before on left eye and suddenly on right eye. In his family his father and his grandmother, on father side, suffered of high eye pressure but they never were operated. Since he was a teenager, he suffered of high eye pressure but he used eye drops to lower intraocular pressure. In particular, he used topic beta-adrenergic receptor antagonist, such as timolol to decrease aqueous humour production by the epithelium of the ciliary body. Patient was hypermetropic and astigmatic with a high level of astigmatism, booth corneal and lenticular. After the trabeculectomy surgery, he presented in booth eyes a bulge on the sclera very close to the limbus located at 12 o’clock. Perhaps scleral fitting failed due to the presence of the two bulges on both eyes that could create problems on the limbus clearance or on the periphery zone [3, 11]. Looking at ophthalmologist’s reports it was clear that patient did not loose too much vision and the optic nerve was saved in booth eyes.
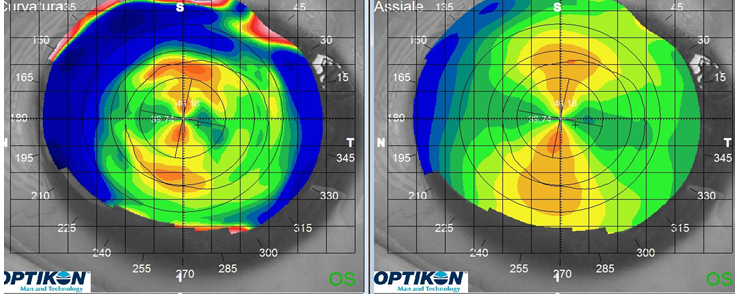
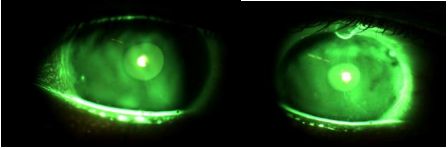
After the anamnesis eyes were controlled in the slit lamp in order to avoid problems when fitting lenses. With the diffuse technique, it was checked the external part of the eyes like eyelids, eyelashes and conjunctiva. It was also used sodium fluorescein to control if there were corneal staining, erosion and/or other problems [12]. At the end of the control it was decided to begin the fitting. It was made a refractive exam to understand why with spectacle lenses visual acuity achieved was not better than 20/32. Using the pinhole it was understood that spectacle lenses were under corrected, probably to balance the binocular vision and having spectacle lenses less thickness in the center. A new refraction was performed and best visual acuity was achieved with the following correction: RE +3.00 -9.00 180° and LE +1.50 -6.75 172°. Patient was under corrected of 3.00 dioptres in astigmatism on the right eye. In addition, patient began to develop presbyopia and need +1.50 additions in booth eyes to achieve good near visual acuity. Patient used to wear corneal rigid gas permeable contact lenses since he was young due to the high astigmatism level and he was not happy to wear glasses because the visual acuity achieved was lower compared to that he could obtain with contact lenses. After having checked visual acuity and the state of booth eyes and corneas new topographies were made in order to compare with the previous one coming from the first eye care practice. Comparing the two different topographies it was immediately clear that there were no problems and corneal parameters normal while he presented high corneal astigmatism. Speaking with the patient it was decided not fit soft contact lenses due to high the level of his astigmatism. Hybrid contact lenses could not be a good solution because the soft skirt curve could be not stable because of the two bulges presented in the limbus area at 12 o’clock. If soft skirts were lifted, air bubbles could enter penalizing visual acuity and creating discomfort for the user. Corneal parameters were in the range of regular cornea but the refractive astigmatism was composed of booth corneal and lenticular. Considering that lenticular astigmatism was more than 0.75/1.00 diopters in booth eyes, bitoric contact lenses could be the best solution for the patient. Parameters with first topography were RE: 8.37mm / 40.32dt @180° and 7.18mm / 47.00dt @90° and for LE: 8.20mm / 41.15dt @170° and 7.06mm / 47.80dt @ 80°. Topographies made into our clinic presented similar corneal parameters. Doing basic calculation about astigmatism it was possible to notice a huge quantity of corneal astigmatism in booth eyes but also an important component of lenticular astigmatism: RE -6.00/ -6.50 of corneal astigmatism and -2.00 of lenticular astigmatism and for RE -6.00 of corneal astigmatism and -1.75 of lenticular astigmatism (Figures 1-3).
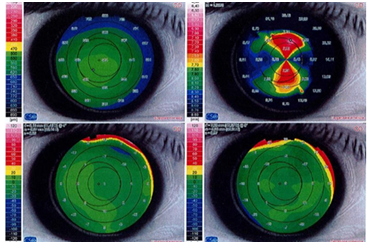
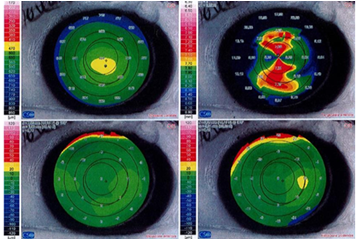
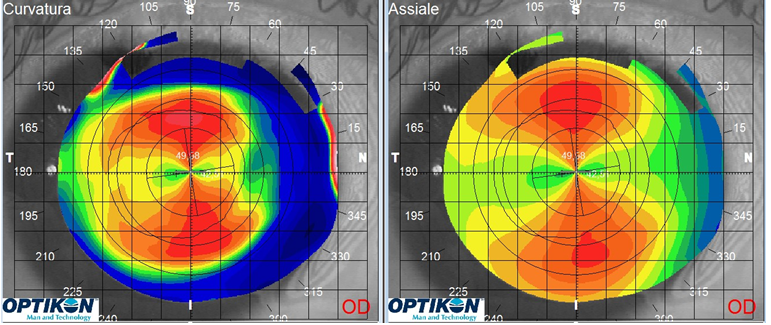
Corneal parameters were similar and booth showed huge quantity of corneal and lenticular astigmatism. The comparison between the two topographies and the analysis of the astigmatism component made by the proportion between refractive astigmatism and corneal astigmatism showed that the patient needed biotic contact lenses. Unfortunately there was not the trial set of bitoric lenses for this reason the fitting began with a back toric compensated contact lens and afterwards added a front toric compensation. Following the fitting rules first lenses tried were RE 8.30 7.80 9.10 +3.00 and LE 8.20 7.70 9.10 +3.00. Right lens was good but too much flat on the flat radius and correct on the opposite; general movement was much and due to this difference between flat and steep radius, lens tilted a little causing general discomfort. Left lens was good but flat in booth radius, movement was much and this lens tilted too. It was decided to steep the fitting in booth eyes in order to reduce lens movement, tilting and improve pattern fluo; lenses tried were RE 8.20 7.70 9.10 +3.00 and LE 8.10 7.70 9.10 +3.00. Now right lens was correct in the flat radius but with too much fluo pattern on the steep radius, left lens was perfect in the flat radius and a little be steep in the opposite. Comfort was improved and tilting was almost completely gone. The fitting was good and the patient was happy with these lenses visual acuity achieved was higher than that obtained in the past. With an over refraction in RE -1.00 - 4.25 3° and LE -1.25 -3.75 177° he achieved 20/22 in binocular vision. To improve fluo pattern, lenses ordered were RE 8.25 7.80 9.10 +1.75 -4.25 3° and LE 8.10 7.75 9.10 +1.00 -3.50 1°. Changes on the flat radius required power adjustment; on the other hand changes on the steep radius did not affect the lens power for this reason. It was decided to order bitoric contact lenses with a high DK material in order to help the oxygen transmissibility through the lenses.
Material used had a DK of 163, with plasma treatment, to improve comfort and wettability; for the moment, lenses were not made progressive because first goal was to have a good far vision and a good fitting. Addition was made subsequently [13].
Follow up #1
At the end of March patient came back into to clinic and we dispatched his lenses the lenses. Lenses were controlled in the slit lamp to check centration and fluorescein pattern. In particular, fitting was checked with the diffuse illumination from low to medium magnification and using fluorescein liquid with the blue cobalt filter and yellow barrier filter. There was not RGP adherence because lens design, diameter, radius, edge and thickness were good. Lenses were not blocked or decentred and tilting was definitely gone. Patient was in comfort and visual acuity was 20/20. In the slit lamp laser marks also were controlled and they were correctly positioned on the flat eye radius. Lenses were dispatched to the patient and a second appointment was fixed the week after. As a system care it was dispatched a multipurpose solution to disinfect and store the lenses with a protein removal weekly use; it was also revised the instruction for lens insertion end removal [14].
Follow up #2
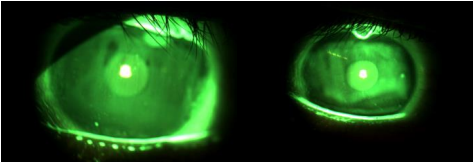
First week of April patient came back again to have a control. Patient’s eyes were controlled in the slit lamp as routine first of all it was made an overall view with low magnification. Starting with the lids closed, the lid margins and lashes were examined for signs of blepharitis or sties. Secondly, with open eyes it was checked upper and lower lid margins to avoid Meibomian gland dysfunction and lid wiper epitheliopathy. It was examined the bulbar conjunctiva and the limbus zone at 12 o’clock in booth eyes to control if lenses movement caused problems at the two bulges. The second part of the control was focused to verify cornea and limbus zone without lenses and using sodium fluorescein. Limbal area was clear without blood vessels, hypoxia, mechanical irritation and solution allergy. With the direct illumination, using the parallelepiped and high magnification, it was checked if corneal staining was present in booth eyes [14]. There were no signs of mechanical damages and no hypoxia, also there were not punctuate diffuse spots. Staining at 3 and 9 o’clock, that is very common in RGP lenses wearers, was not present on booth eyes. For these reasons it was decided the lenses parameters were correct. Visual acuity was the same at the lenses dispensing appointment. It was decided to reorder the lenses with the addition to achieve also near vision and patient was very happy to try this solution. Speaking with the patient and asking for more details about his life style and work it was decided to use a centre distance geometry. The only problem showed the control was reduced lens wettability in booth lenses; the direct illumination showed some hydrophobic spots just after the blink. It was revised the care regimen composed by disinfecting multipurpose solution and protein removal once a week; it was also adding a soap specified in proteins deposits removal. It was decided that in the near future, if this problem should remain, the best solution was to change lens material with a lower DK.
For the moment lenses where reordered with the same high DK material, lenses were RE 8.25 7.80 9.10 +2.00 -4.25 3° ADD +1.50 and LE 8.10 7.75 9.10 +1.00 -3.50 1°ADD +1.50 (Figures 5 & 6).
Follow up #3
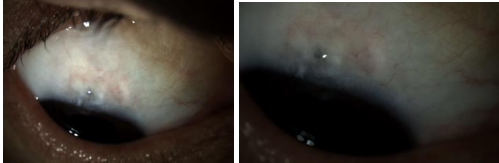
After ten days approximately patient came back to our clinic in order to return old lenses and new lenses were dispensed. In the slit lamp it was checked again cornea and limbus state in order to avoid general staining, mechanical damages and inferior epithelial arcuate lesion like smile stain in both eyes. There were no punctuating diffuse spots or other problems in right and left eyes. Lens movement did not cause damages near and on the two bulges presented at 12 o’clock after the surgery. The control with the direct illumination showed that there was still reduced wettability in booth lenses but now on the lenses were also increased areas of hydrophobicity. Comparing to the hydrophobic zones presented at the follow up number two, now the situation was a little is worse. These hydrophobic zones caused some times a penalty in visual acuity because spots were just in front of the optic zones [14]. Finally, it was decided to change lenses material and going from Z material of Menicon, DK 163 to Menicon EX material, and DK 64 without plasma treatment. Lenses were the same in parameters and powers but they were made in EX material was used (Figures 7 & 8).
Follow up #4
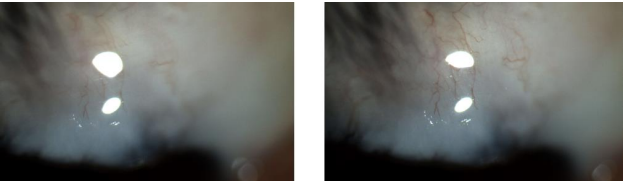
End April patient came back to our clinic and final lenses were dispatched. Lid, eye lid, cornea and limbus zones were controlled another time with the slit lamp showing no problems in central and peripheral staining. Lens movement did not cause damages near and on the two bulges presented at 12 o’clock after the surgery. Old lenses were returned to us and checked with the microscope it was clear that wettability was not good and booth surfaces presented huge hydrophobic zones. New lenses dispatched were: RE 8.25 7.80 9.10 +2.00 -4.25 3° ADD +1.50 and LE 8.10 7.75 9.10 +1.00 -3.50 1°ADD +1.50, booth on Menicon EX material [15, 16]. Excluding material problems, patient achieved good visual acuity and was very happy with this solution (Figures 9 & 10).

Follow up #5
At the begging of May final lenses were dispatched to the patient. Cornea, limbus zones and the other eye parts were controlled without showing problems. Also the two bulges were controlled in order to avoid problems caused by lens movement. It was explained another time the care system composed by a multipurpose solution to use every day, protein remover weekly use and the soap at need.
Discussion
In this fitting it was important to work step by step, first of all to define patient’s needs and second found the best geometry that can achieve good visual acuity and ocular health after the surgery intervention. In this fitting it was important to understand patient’s needs considering that his refraction, to achieve good visual acuity, was high and wear spectacles can penalise the vision. The finally geometry used was a bitoric lens with front cylinder for the correction of the corneal astigmatism and internal astigmatism and a back toric design to compensate the corneal astigmatism and stabilize the lens [11]. This geometry was used because it provided lens stability on corneal astigmatism equal or greater than 2.25 D and total correction of refractive astigmatism working with the following rule: CA ≥ 2.25 Dt and IA ≥ 1.00 Dt. In particular the fitting began with a back toric compensation lens because the diagnostic set of bitoric lenses was not used in the clinic. The geometry used to try lenses and verify fluo pattern in our clinic was a back toric compensation with a front surface cylinder to compensate only the back surface astigmatism, afterwards it was made an over cylindrical refraction with the lenses on the eyes in order to confirm the real need of bitoric lenses [11, 14]. It was decided to work with a 9.10mm diameter instead of the standard 9.60mm; it was decided to use a smaller diameter to avoid problems in the bulge’s area present in booth eyes. Standard diameter of 9.60mm could create problems during the lens movement considering the presence of the two bulges. Principal problems that should come out could be instable vision, because lenses could rebound like a flipper and staining in the bulge’s area on the limbus zones. To have an instable vision for the patient was a serious problem for his work considering that he was a car seller and he needed good and stable vision after every blink. When a toric lens design is used, it is very important to stabilise the lens after the blink and the correct meridian to avoid unstable and/or double vision especially when a bitoric lens is fitted. In the design fitted, the flattest meridian axis is indicated by two marks, not necessarily placed on the horizontal meridian [11]. When the correct fluo pattern was achieved, lenses were ordered also in progressive version because the lab could produce bitoric progressive lenses in consideration of the fact that the patient was developing presbyopia; the geometry fitted was a distance vision in the centre with a progression zone and finally near vision. First lens material was Menicon Z with a hyper DK gas permeable material that could offer comfort, wettability and long term eye health also crisp vision during the wear. In the market, this material offered one of the highest levels of oxygen permeability into the world of GP materials [15]. Technical material data were: UV filter, DK of 163 x 10-11 (cm3/sec) x (mlO2/ (mlxmmHg)) (ISO polarography method) and refractive index 1.437 [15]. Unfortunately, this material caused problems of wettability that created unstable vision and uncomfortable lenses during the days. Patient presented also problems in tear film probably caused by the surgery and contact lenses could interfere with the normal tear film structure and function, increasing tear film evaporation. For this reason, it was decided to change lens material decreasing DK from 163 to 64 [15, 16, 17]. Like a care system, it was recommended a daily solution for RGP lenses with natural polymer as polylysine, vitamin C glucoside and hyaluronic acid. To guarantee comfort and lens disinfection it was recommended a weekly system to remove proteins. This solution removes proteins from the surface of the lens by simply soaking them in the mixture for only 30 minutes [18]. This system is strong and rapid in disinfection against the entire organism likely to contaminate lenses, including bacteria moulds, yeasts, viruses and ancanthamoeba. At lens removal, eye drops with a concentration of sodium ialuronate equal to 0.30% was recommended [18]. Every three months when patient came to our clinic to buy stock solutions a quickly control was always made to avoid corneal staining, lens print and other problems. Now patient is happy with his lenses and he uses spectacles only when he is at home. Thanks to fitting his father, it was possible to make also an eye check to his son, 8 year old, and it was discovered that he was hypermetropic and astigmatic, for this reason he was fitted with soft toric contact lenses made to order but to achieve better visual acuity he will be fitted in the next future with RGP. Every year the family goes to an ophthalmologist for control.
Conclusion
This case report demonstrates the role of patient history, clinical observation and listening to patient needs. Patient history was important because his familiarity with glaucoma and high eye pressure were the cause of his glaucoma surgery. In addition, it was important to find a design that could achieve good visual acuity at all distance and ocular health for his cornea and sclera. This case was not complex in terms of fitting, because cornea is regular, but it is interesting for the design used and for the results obtained. At the end optometrist can be a guide for his patient and must always find the best and healthy solution for him. Finally, it is important to follow a patient with glaucoma or high eye pressure because this pathology, being silent, is the second- leading cause of blindness after cataracts all over the world.
References
-
Facts about Glaucoma (2016) National Eye Institute.
-
Mantravadi AV, Vadhar N (2015) Glaucoma Primary care, Elsevier Science Direct 42(3): 437-449.
-
Harper D (1960) Glaucoma Online Etymology Dictionary.
-
Ferri FF (2010) Ferri’s differential diagnosis: a practical guide to the differential diagnosis of symptoms, signs, and clinical disorders.
-
Resnikoff S, Pascolini D, Etyaale D, Kocur I, Pararajasegaram R, et al. (2004) Global data on visual impairment in the year 2002. Bulletin of the World Health Organization 82(11): 844-851.
-
Leffler CT, Schwartz SG, Giliberti FM, Young MT, Bermudez D (2015) What was Glaucoma Called Before the 20th Century? Ophthalmology and Eye Diseases 7: 21-33.
-
Arthur J, Sit MD (2006) many types of glaucoma, one kind of damage to optic nerve.
-
“Glaucoma – National Institutes of Health” (2011) Nihseniorhealth.gov.
-
Parikh RS, Parikh SR, Nevins S, Arun E, Thomas R (2008) Practical approach to medical management of glaucoma. Indian J Ophthalmol 56(3): 223-230.
-
A handbook of Contact Lens Management (2011) The vision care institute of Johnson and Johnson Vision Care, part of Johnson and Johnson Medical Ltd, Ian Davies, Allan Kruse.
-
Efron N (1998) Grading scales for contact lens complications. Opthalmic Physiol 18(2): 182-186.
-
www.menicon.com/corporate/menicon-worldwide/
-
Efron N, Morgan PB, Katsara SS (2001) Validation of grading scales for contact lenses complications. Opthalmic Physiol Opt 21(1): 17-29.
-
www.davidthomas.com/assets/MeniconZBTCBT.PDF
-
www.menicon.com/corporate/menicon-worldwide/
-
www.menicon.com/ifu/pdfs/RDHMPI005/IFU_ RDHMPI005_it.pdf
-
www.menicon.com/consumer/lens-care/gp/progent/
-
www.menicon.com/consumer/lens-care/gp/menicare- pure/.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report