The Contribution of Autorefractometry to the Diagnosis and Management of Refractive Errors in Patients Aged 6 to 18 Years Northern Benin in 2024
The aim is to evaluate the contribution of autorefractometry to the diagnosis and management of ametropia in subjects aged 6 to 18 years in Northern Benin in 2024. Methods: This was a descriptive and analytical cross-sectional study with prospective data collection over a period from May 20 to September 30, 2024, at the Regional Hospital based University Hospital Center in northern Benin. This study was conducted with the approval of the Local Ethics Committee for Biomedical Research at the University of Parakou (CLERB/UP) under number 1044/2025/CLERB-UP/P/SPµ/R/SA Results: Our results included 208 eyes from 104 individuals. The median age was 17 years, and there was a predominance of females with a sex ratio of 0.4. Before cycloplegia, hyperopia and astigmatism were the most common refractive errors, each accounting for 50.5%, followed by myopia (32.2%). After cycloplegia, hyperopic eyes accounted for 75.5% of cases. Astigmatic and myopic eyes accounted for 73.5% and 17.3%, respectively. The mean spherical equivalent at correction was 0.23 ± 1 D, compared to 0.61 ± 1 D on autorefraction under cycloplegia. This represents a highly significant decrease of 0.38 D (p-value = 0. Conclusion: Cycloplegic autorefraction is essential for the accurate diagnosis of refractive errors in children and adolescents, particularly for detecting latent hyperopia to prevent the development of amblyopia.
Introduction
Refractive errors (ametropia) encompass all situations where the eye’s optical system fails to focus the image of an object onto the retina [1]. In 2020, the World Health Organization (WHO) estimated that 88.4 million people worldwide live with visual impairment due to uncorrected refractive errors [2]. In children, the prognosis for visual impairment depends not only on the degree of refractive error but, above all, on the early intervention and quality of care [3]. Refractive errors constitute a growing global public health problem, particularly among children and adolescents. Thus, in order to improve the diagnostic accuracy of ametropias and to optimize the visual correction of patients aged 6 to 18 years, we conducted a study on the contribution of auto-refractometry in the diagnosis and management of ametropias in subjects aged 6 to 18 years in northern Benin in 2024.
Methods
This was a descriptive and analytical cross-sectional study with prospective data collection over a period from May 20 to September 30, 2024. It included patients aged 6 to 18 years who consulted at the ophthalmology department. Sampling was non-probability, with exhaustive recruitment of all subjects admitted for consultation during the study period who met the inclusion criteria.
Data were collected using an anonymous individual questionnaire through a semi-structured interview, supplemented by clinical examination and therapeutic data. For each patient aged 6 to 18 years seen for consultation, after gathering their complaints and medical history, uncorrected distance and near visual acuity was measured. They then underwent slit-lamp examination and fundus examination. Two successive automated refractions were subsequently performed: the first before any administration of cycloplegic eye drops, and the second 30 minutes after three instillations of one drop of 0.5% cyclopentolate alternating with tropicamide at five-minute intervals. Finally, a subjective refraction was performed for the patient’s optical correction. The collected data were analyzed using EPI Infos 7.2.2.6 software and then checked using Stata 15.0 for Windows. The significance threshold was set at p < 5%. This study received approval from the Local Ethics Committee for Biomedical Research of the University of Parakou (CLERB/ UP) under number 483/2024/CLERB-UP/P/SPµ/R/SA, and data confidentiality was maintained.
Results
The results were based on 208 eyes from 104 individuals included in the study.
Socio-demographic characteristics
Age
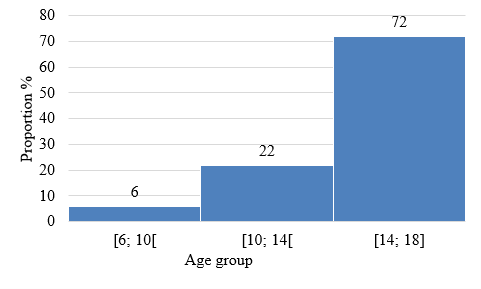
The mean age of the subjects studied was 15 ± 3 years, with a range of 6 to 18 years. The median age was 17 years. Patients aged between 14 and 18 years represented 72%. Figure 1 shows the age distribution of the subjects.
Sex
Female subjects represented 70% (N=73) of the participants; a sex ratio of 0.4.
Educational level
| Education Level | Number of Students | % |
|---|---|---|
| Primary | 6 | 6 |
| Secondary | 47 | 45 |
| Higher | 51 | 49 |
| Total | 104 | 100 |
Table 1: Distribution of subjects aged 6 to 18 years surveyed during consultations in 2024 according to their educational level T
Clinical Feature
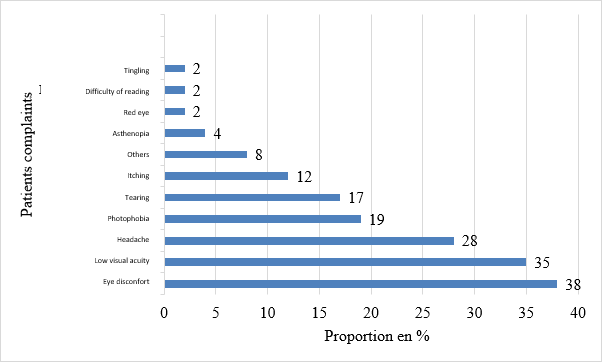
Complaints Eye pain, decreased vision, and headaches accounted for 38%, 35%, and 28% of patient-reported complaints, respectively. Figure 2 illustrates the distribution of subjects according to their complaints upon admission.
Visual Acuity
Twenty-nine percent (29%) had a slight to moderate decrease in distance visual acuity according to the WHO classification
| Number | % | |
|---|---|---|
| Far vision | ||
| < 1/20 | 0 | 0 |
| [1/20; 3/10] | 10 | 5 |
| [3/10; 8/10] | 51 | 24 |
| ≥ 8/10 | 147 | 71 |
| Near vision | ||
| N1,5 to N2 | 188 | 90 |
| N 3 to N14 | 20 | 10 |
| Total | 208 | 100 |
Table 2: Distribution of subjects aged 6 to 18 years surveyed in consultation at CHUD/BA in 2024 according to their uncorrected T
Hospital Frequency of Different Types of Refractive Errors in Subjects Aged 6 to 18 Years after Automatic Refraction without Cycloplegia and with Cycloplegia
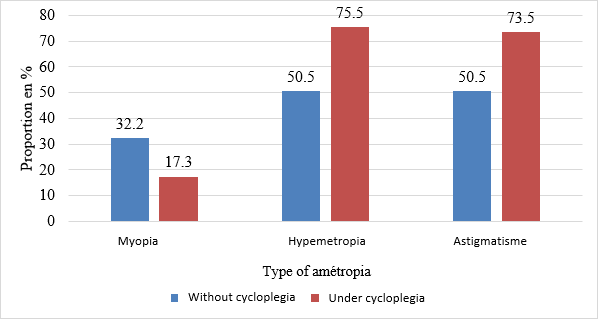
The frequency of refractive errors in our surveyed sample increased from 91% (n=189 eyes) without cycloplegia to
99% (n=206 eyes) with cycloplegia during autorefraction. Figure 3 shows the distribution of the different types of refractive errors before and after cycloplegia.
Influence of Cycloplegia on Patients’ Refractive Profile
Variation in the power of spherical refractive errors before and after cycloplegia
Spherical Power
Before cycloplegia, the average power of the spheres was -0.15 ± 5 D.
After cycloplegia, this average increased to +0.89 ± 1 D. This represents a highly significant increase of 1.04 D after cycloplegia (p-value = 0.005).
In Myopic Subjects
The proportion of myopic subjects decreased from 32.2% before cycloplegia to 17.3% after cycloplegia, representing a highly significant decrease of 15% in diagnosed myopic patients (p-value = 0.000). Among myopic patients before and after cycloplegia (13.9%), the mean spherical power value increased by 0.04 D (from -1.22 ± 0.7 D to -1.18 ± 0.8 D) after cycloplegia, although this difference was not statistically significant (p-value = 0.7). The change in myopia prevalence before and after cycloplegia is illustrated in Table IV.
In Hyperopic Subjects
The proportion of hyperopic subjects before cycloplegia was 50.5%. This proportion increased to 75.5% under cycloplegia, representing a highly significant increase of 25% in the hyperopic population (p-value = 0.000). The mean spherical power in hyperopic subjects before and after cycloplegia (47.6%) increased significantly by 0.6 D, from 1.02 ± 1 D to 1.62 ± 1 D (p-value = 0.000). Variation in the Power of Cylindrical Ametropia Before and After Cycloplegia The mean cylindrical power before and after cycloplegia was -0.42 ± 0.8 D and -0.56 ± 0.8 D, respectively, representing a highly significant decrease of -0.14 D (p-value = 0.000). The prevalence of astigmatism, which was 50.5% without cycloplegia, increased significantly by 24% after cycloplegia (p-value = 0.000). The mean power in astigmatic patients before and after cycloplegia (42.3%) decreased by a non- significant amount of 0.04 D, from -0.90 ± 1 D to -0.94 ± 1 D after cycloplegia (p-value = 0.45). Change in Spherical Equivalent Before and After Cycloplegia The spherical equivalent was -0.36 ±5 D before cycloplegia and +0.61 ±1 D after cycloplegia. It therefore increased by 0.97 D, a highly significant increase (p-value = 0.009).
In myopic patients before and after cycloplegia (13.9%), the mean spherical equivalent decreased from -1.54 ±1 D to -1.60 ±1 D after cycloplegia. This decrease of 0.06 D was not significant (p-value = 0.65). In hyperopic patients before and after cycloplegia (47.6%), the mean spherical equivalent was 0.81 ±1 D and 1.37 ±1 D before and after cycloplegia, respectively. This represents a highly significant increase of 0.57 D (p-value = 0.000).
In astigmatic patients before and after cycloplegia, this difference of 1.45 D was not significant, ranging from -0.93 ±8 D to 0.52 ±2 D after cycloplegia (p-value = 0.09)
Variation in Spherical Power with Optical Correction
The mean spherical power with optical correction was 0.34 ±1 D compared to 0.89 ±1 D with autorefraction under cycloplegia. This represents a highly significant decrease of 0.55 D (p-value = 0.000). In myopic patients (after cycloplegia), this mean power was -1.20 ±0.8 D with optical correction, a non-significant decrease of 0.14 D compared to -1.06 ±0.7 D measured under cycloplegia (p-value = 0.19). In hyperopic patients, the mean spherical power was 0.76 ±0.65 D with correction, a highly significant decrease of 0.66 D compared to 1.42 ±1 D measured under cycloplegia (p-value = 0.000).
Comparison of Optical Correction Results with those of Autorefraction under Cycloplegia
Variation in Spherical Power with Optical Correction
The mean spherical power with optical correction was 0.34 ±1 D compared to 0.89 ±1 D with autorefraction under cycloplegia. This represents a highly significant decrease of 0.55 D (p-value = 0.000). In myopic patients (after cycloplegia), this mean power was -1.20 ±0.8 D with optical correction, a non-significant decrease of 0.14 D compared to -1.06 ±0.7 D measured under cycloplegia (p-value = 0.19). In hyperopic patients the mean spherical power was 0.76 ±0.65 D at correction, a very significant decrease of 0.66 D compared to 1.42 ±1 D measured under cycloplegia (p-value=0.000).
Variation in Cylindrical Power with Optical Correction
With optical correction, the mean cylindrical power (-0.22 ±0.48 D) significantly increased by 0.33 D compared to that (-0.55 ±0.84 D) measured under cycloplegia (p-value = 0.000). In astigmatic patients, this mean was -0.28 ±0.53 D with correction instead of -0.75 ±0.90 D under cycloplegia. This represents a significant increase of 0.44 D (p-value = 0.000).
Change in Spherical Equivalent with Optical Correction
The mean spherical equivalent with correction was 0.23 ±1 D instead of 0.61 ±1 D with autorefraction under cycloplegia. This represents a highly significant decrease of 0.38 D (p-value = 0.000). In myopic patients, under cycloplegia, this mean equivalent (-1.45 ±1 D) increased slightly by 0.06 D with optical correction (p-value = 0.74). In hyperopic patients, there was a highly significant decrease of 0.48 D, varying from 1.19 ±1 D under cycloplegia to 0.70 ±0.75 D with correction. The same was true for astigmatic patients, with a difference of 0.34 D between the value under cycloplegia (0.53 ± 1.5 D) and that under correction (0.18 ± 1 D), with a p-value of 0.000.
In astigmatic patients, the mean spherical equivalent under correction was 0.18 ± 1 D instead of 0.53 ± 1.5 D during autorefraction under cycloplegia. This represented a highly significant decrease of 0.34 D, with a p-value of 0.000.
Comparison of Visual Acuity after Final Optical Correction to that Measured before Correction
Ranging from 1 to 11/10, distance visual acuity at admission without optical correction improved from an average of 8 ± 3/10 to 10 ± 1/10 after final correction, representing an average improvement of 2/10. After final correction, more than 90% of patients had a visual acuity of at least 8/10. Figure 6 shows the change in distance visual acuity at admission and after optical correction.
Factors Influencing the Variation of the Spherical Equivalent between the Measurement under Cycloplegia and the Final Optical Correction
In multivariate analysis, after introducing the singularly significant variables at 20% (age, sex, education level and family history of wearing corrective lenses), the final 5% model is presented in Table VII as follows.
Discussion
The mean age in our study was 15 ± 3 years, with a range of 6 to 18 years. This result is close to that of Zhou, et al. [4] in China, who reported a mean age of 15.23 ± 1.77 years, and Vonor, et al. [5] in Togo, who found 12.7 ± 2.9 years. However, it differs from that of Assavedo, et al. [6], who reported a mean of 9.2 ± 2 years, and from that of Czepita, et al. [7] (11 ± 3 years). This difference is due to the diversity of the study settings.
Visual impairment and headaches accounted for 63% of the complaints reported by the subjects in our series. These results were similar to those of Gbe, et al. in Côte d’Ivoire [8] and Ayed, et al. in Tunisia [9] reported 61% and 60% respectively for decreased vision and headaches. The eye pain was reported with 38% in this study, this condition is related to the subjects with strong accommodative power [10]. Hashemi, et al. also reported that eye pain was common among university students [11]. These include Assavedo, et al. [6] and Assoumou, et al. [12], who reported itching (36%) and tearing (32%) as the main complaints, respectively.
The majority of subjects (71%) in this study had good distance visual acuity ≥8/10 according to the WHO classification [13]. Paluku, et al. (81%) then Kouassi, et al. have reported 78% [14, 15]. This explains why visual acuity is not the only indicator for diagnosing refractive error. Good visual acuity does not mean the absence of refractive error. Many individuals may have apparently normal visual acuity (≥ 8/10) while suffering from mild or moderate refractive error. The prevalence of refractive errors in subjects aged 6 to 18 years at the northern benin was 91% after autorefractometry without cycloplegia. This is significantly higher than the 19% and 21% found by Assavedo, et al. in Parakou [6] and Kouassi, et al. in Côte d’Ivoire [15], respectively. This large difference can be explained by the fact that in our study, all included subjects underwent a complete ophthalmological examination, including automatic refraction regardless of visual acuity, whereas in these two other studies, only children with visual acuity ≤ 7/10 in at least one eye underwent a complete examination.
Hyperopia and astigmatism were the most frequent refractive errors, each accounting for 50% of cases. Contrary to the results of other studies [8, 12, 14, 16] where astigmatism was the most prevalent refractive error, our proportions were closer to those of Assavedo, et al. [6], who found hyperopia (42%) to be the most common, followed by astigmatism (39%).
In our series, myopia was present in 32% of cases before cycloplegia. After cycloplegia, 13% of the eyes that were myopic remained so, and the prevalence increased to 17%, representing a highly significant decrease of 15% in myopic eyes. This decrease was also noted by Wane, et al. [17] in Senegal, where the proportion of myopic individuals decreased from 62% before cycloplegia to 30% after cycloplegia. Our results differ from those of Mvogo, et al. [18] in Cameroon, who noted no cases of myopia after cycloplegia in a study of 110 eyes. This difference could be explained, on the one hand, by the sample size and, on the other hand, by the older age of the participants in their study population (35 to 45 years). The frequency of hyperopia increased from 50% before cycloplegia to 75% after cycloplegia. Wane, et al. [17] also showed in their study that the frequency of hyperopia increased from 34% to 68% after cycloplegia.
The majority of subjects therefore had latent hyperopia that became apparent after cycloplegia.
In our study, the frequency of astigmatism was estimated at 50% before cycloplegia; This frequency increased to 73% after cycloplegia. This could still be explained by the role of accommodation in masking refractive errors in children. However, Kouassi, et al. [15] found a contradictory result, with the frequency of astigmatism decreasing from 40% to 16% after cycloplegia; similarly, Jeddi, et al. [19] found no difference. These discrepancies could be explained by methodological differences and the characteristics of the populations studied in each study. Furthermore, race-related factors are among the reasons for the difference in the prevalence of astigmatism worldwide [20].
This study also allowed us to confirm that cycloplegia causes significant in the spherical equivalent, with a mean difference of 0.97 D. This result is consistent with those of Fang Gu, et al. [21] and Jeddi, et al. [19], who reported mean differences of 0.92 D and 0.79 D, respectively.
Conclusion
Our results confirm the high prevalence of refractive errors, particularly hyperopia and astigmatism, in subjects aged 6 to 18 years. Autorefractometry has proven to be a valuable tool for the initial screening of refractive errors. However, our results clearly demonstrate the need to supplement this examination with cycloplegia, particularly in young children and adolescents. Appropriate optical correction, based on measurements taken after cycloplegia, led to a significant improvement in visual acuity in the majority of subjects. This observation underscores the importance of early and appropriate management of refractive errors to prevent vision problems and optimize visual comfort and well-being in children.
References
-
Paluku Kasomo J, Kahindo Kahatane A, Kanyere Mutuho C, Mumbere Muhesi T (2022) Fréquence des amétropies aux cliniques universitaires du graben en République Démocratique du Congo. kisMed 12(2): 556‑563.
-
WHO (2026) Blindness and vision impairment. World Health Organization.
-
Sow AS, Ndiaye JM, Wane AM, Kane H, Ka AM, et al. (2019) Ametropia among senegalese children in a hospital setting. J Fr Ophtalmol 42(9): 959‑961.
-
Zhou Y, Chen X, Huang X, Li L, Zhu Y, et al. (2024) Prevalence and association of uncorrected refractive error among Chinese adolescents: a cross-sectional study. BMC Public Health 24(1): 2904.
-
Vonor K, Ayena KD, Dzidzinyo K, Amedome KM, Santos M, et al. (2014) Severe ametropia in children in Lomé (Togo). Me´decine et Sante´Tropicales 24(2): 219‑220.
-
Assavedo CRA, Issifou Alfa Bio A, Hada S (2021) Prevalence and Associated Factors of Ametropia among Schoolchildren Aged at Least 6 Years in North Benin. Acta Scientific Ophthalmology 4(10): 34‑41.
-
Czepita D, Mojsa A, Ustianowska M, Czepita M, Lachowicz E (2007) Role of gender in the occurrence of refractive errors. Ann Acad Med Stetin 53(2): 5‑7.
-
Gbe K, Kouassi L, Coulibaly F, Boni S, Ouattara A, et al. (2014) Vices de réfraction chez des enfants dans une consultation privée à Abidjan: à propos de 635 cas. Revue SOAO 1: 40‑43.
-
Ayed T, Sokkah M, Charfi O, El Matri L (2002) Epidemiologic study of refractive errors in schoolchildren in socioeconomically deprived regions in Tunisia. J Fr Ophtalmol 25(7): 712‑717.
-
Jin CC, Pei RX, Du B, Liu GH, Jin N, et al. (2021) Lag of accommodation predicts clinically significant change of spherical equivalents after cycloplegia. Int J Ophthalmol 14(7): 1052‑1058.
-
Hashemi H, Nabovati P, Khabazkhoob M, Yekta A, Emamian MH, et al. (2024) Comparison of the accommodative amplitude measured with and without the use of a specialised accommodative rule in children. BMJ Open Ophth 9(1).
-
Assoumou P, Kapinga Bulanda F, Mba Aki T, Oyieye A, Mve Mengome E (2018) Ametropia in primary schools in the Estuary Province of Gabon. Journal of the Gabonese Medical Society 16(45): 6‑10.
-
Kodjikian L, Scherrer J, Iliev M, Halberstadt M, Garweg J (2007) 063 Étude de la fonction visuelle au cours de la toxoplasmose oculaire. Journal Français d’Ophtalmologie 30: 2S168.
-
Paluku Kasomo J, Kahindo Kahatane A, Kanyere Mutuho C, Mumbere Muhesi T (2022) Fréquence des amétropies aux cliniques universitaires du graben en République Démocratique du Congo. kisMed 12(2): 556‑563.
-
Kouassi LJ, Gbe K, Coulibaly F, Ouffoue Y, Fanny A (2018) Evaluation de la réfraction en milieu scolaire 1: 23‑26.
-
Sounouvou I, Tchabi S, Doutetien C, Sonon F, Yehouessi L, Bassabi SK (2008) A study of refractive errors in a primary school in Cotonou, Benin. J Fr Ophtalmol 31(8): 771‑775.
-
Wane AM, Ndoye Roth PA, Ba EA, Iraqui K, Demedeiros ME, et al. (2007) Les variations de la réfraction sous cyclopentolate chez le mélanoderme sénégalais. Journal Français d’Ophtalmologie 30(S2): 2S209.
-
Mvogo SRE, Dohvoma VA, Fangwa JSN, Tsimi CM, Zoua MEA, et al. (2019) Age de début de la presbytie chez le sujet noir camerounais. Pan African Medical Journal 32(1).
-
Jeddi A, Ben Hadj Alouane W, Hammoud M, Malouch N, et al. (2002) Full optical correction after cycloplegia in headache. J Fr Ophtalmol 25(3): 270‑273.
-
Mahjoob M, Heydarian S, Nejati J, Ansari-Moghaddam A, Ravandeh N (2016) Prevalence of refractive errors among primary school children in a tropical area, Southeastern Iran. Asian Pacific Journal of Tropical Biomedicine 6(2): 181‑184.
-
Gu F, Gao HM, Zheng X, Gu L, Huang J, et al. (2022) Effect of Cycloplegia on Refractive Error Measure in Chinese School Students. Ophthalmic Epidemiol 29(6): 629‑639.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report