Brief Review of Pharmacotherapy for Pulmonary Arterial Hypertension
Pulmonary arterial hypertension affects the distal pulmonary vasculature causing intimal, medial, adventitial fibrosis, thickening and periadventitial changes leading to progressive increase in pulmonary vascular resistance and pulmonary arterial pressure [1]. Pulmonary hypertension (PH) is defined as mean pulmonary artery pressure equal to or greater than 25 mm Hg at rest.
Introduction
Pulmonary arterial hypertension affects the distal pulmonary vasculature causing intimal, medial, adventitial fibrosis, thickening and periadventitial changes leading to progressive increase in pulmonary vascular resistance and pulmonary arterial pressure [1]. Pulmonary hypertension (PH) is defined as mean pulmonary artery pressure equal to or greater than 25 mm Hg at rest. PH is classified into five major groups by the World Health Organization (WHO) based on their etiologies most recently by the 5th World symposium on Pulmonary hypertension in 2013 [2]. WHO Group I contains Pulmonary arterial hypertension (PAH) which acan be idiopathic, heritable, drug and toxin induced, associated with connective tissue disorders, HIV infection, portal hypertension, congenital heart diseases, schistosomiasis, pulmonary veno occlusive disease/ pulmonary capillary hemangiomatosis, persistent pulmonary hypertension of the newborn.Specifically, PAHis defined as the presence of mean pulmonary pressure artery greater than 25 mm Hg at rest when the pulmonary capillary wedge pressure is less than 15 mm Hg and the pulmonary vascular resistance is greater than 3 Wood units [2]. Pharmacologic intervention in pulmonary hypertension has been primarily focused on targeting the physiological pathways involved in controlling pulmonary vasoreactivity. Consequently, Group I PH or PAH is where most of this therapeutic development has occurred. Drug therapy for PAH can be classified based on their mechanisms of action into phosphodiesterase 5 (PDE-5) inhibitors, guanylate cyclase stimulators, prostacyclin analogs, prostacyclin receptor agonists, endothelin receptor antagonists [1].
Keywords: Cyclic guanosine monophosphate (cGMP); Obstructive sleep apnea; Calcium channel blockers
Phosphodiesterase-5 Inhibitors
PDE-5 inhibitors inhibit phosphodiesterase-5 isoenzyme which is specific for breaking down cyclic guanosine monophosphate (cGMP). PDE-5 is found primarily in the smooth muscles of the pulmonary vasculature, the corpus cavernosum, other visceral smooth muscle tissue, platelets. Degradation of cGMP results in smooth muscle vasoconstriction. Therefore PDE-5 inhibitors increase the availability of cGMP which results in vasodilation [3]. Three PDE-5 inhibitors are currently being used and were studied in the past [4, 5, 6, 7, 8]. Sildenafil and Tadalafil are the two FDA approved PDE-5 inhibitors in the treatment of Group I PH or PAH to improve exercise capacity. SUPER-1 & SUPER -2 [4, 5] trials randomized 278 patients with symptomatic pulmonary hypertension to placebo or variable doses of oral sildenafil (20mg, 40mg or 80 mg) three times daily. The primary endpoint was improvement in six-minute walking distance (6MWD). 6MWD was improved in majority of the patients receiving sildenafil at both 1 year and 3 years. PHIRST6 and PHIRST -27 studies randomized patients with PH on background Bosentan therapy to placebo or increasing doses of oral tadalafil (2.5mg, 10mg, 20mg or 40mg) once daily. There was significant short term improvement in 6MWD and time to clinical deterioration in the therapy group [6, 7]. Even though vardenafil has been studied in the EVALUATION trial [8], it has not received FDA approval for the treatment of PAH yet. Sildenafil is available as Revatio [9] and Tadalafil is available as Adcirca in the United States [10]. Some of the common side effects of PDE-5 inhibitors include headache, flushing, dyspnea, epistaxis [9, 10].
Guanylate Cyclase Stimulators
Guanylate cyclase stimulators work by targeting the enzyme Guanyl cyclase in the nitric oxide pathway. Soluble guanylate cyclase serves as a catalyst to produce cGMP in the nitric oxide pathway, which then promotes vasodilation and indirectly inhibits deleterious downstream inflammatory effects resulting in vessel wall injury [11]. Riociguat is the first of its class that has been studied and FDA approved for the indication of improving exercise capacity in patient with Group I PH (PAH) and Group IV PH which is chronic thromboembolic pulmonary hypertension (CTEPH). PATENT-1 [12] randomized patients with PH (including those on stable doses of endothelin receptor antagonists or inhaled prostacyclin analogs) to either placebo or oral Riociguat up to 2.5 mg three times daily. Of note, patients who were already on intravenous prostacyclin analogs or PDE-5 inhibitors were excluded. 6MWD was the primary endpoint which improved significantly in the Riociguat group. Secondary endpoints such as pulmonary vascular resistance, hemodynamic parameters such as mean pulmonary artery pressure, cardiac output also improved in the Riociguat group [12]. Riociguat is currently the only available soluble guanylate cyclase stimulator available and approved for use in PH. It is available as a tablet, Adempas in the United States. It is contraindicated when other nitrate therapy, PDE-5 inhibitors are used. Most common side effects of Riociguat are headache, diarrhea, nausea, dyspepsia, constipation [13].
Prostacyclin Analogs
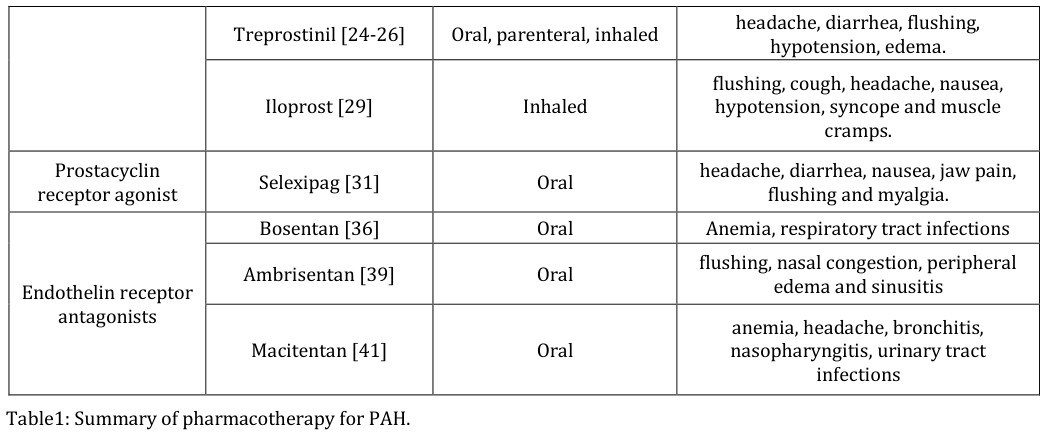
Prostacyclin is an endogenous substance produced by endothelial cells and produce smooth muscle vasodilatation. Prostacyclin analogs are synthetic equivalents of endogenous prostacyclin. In PAH, prostacyclin analogs help in improving the balance between vasoconstriction and vasodilation at the level of the pulmonary vasculature and thereby help reduce pulmonary vascular resistance [14]. Prostacyclin analogs or prostanoids are available in oral, inhaled and parenteral formulations. The current FDA approved prostanoids include epoprostenol, treprostinil and iloprost. Epoprostenol is available as Flolan [15] & Veletri [16] for parenteral administration in Group I PH or PAH. Barst et al randomized 81 patients with PH to receive intravenous epoprostenol versus conventional therapy. The group receiving intravenous epoprostenol showed improvement in 6MWD, hemodynamics and mortality [17]. Badesch, et al. [18] randomized 111 patients to receive epoprostenol versus conventional therapy. They demonstrated that the group receiving epoprostenol showed an improvement in 6MWD.Common side effects include dizziness, jaw pain, headache, musculoskeletal pain, flushing, hypotension, dyspnea. It is contraindicated in systolic heart failure [15, 16]. Simonneau, et al. [19] randomized 470 patients with primary PH to continuous subcutaneous treprostinil infusion vs placebo for 12 weeks and showed improved 6MWD among patients who received treprostinil. McLaughlin, et al. [20] randomized 235 patients with PH who were already on Bosentan or sildenafil to inhaled treprostinil vs placebo 4 times daily. Inhaled treprostinil improved 6MWD significantly but there was no improvement in time to clinical worsening. Jing, et al. [21] randomized 349 patients not on any background therapy to oral treprostinil (up to a maximum of 12 mg twice daily) as monotherapy versus placebo for a period of 12 weeks and found that oral treprostinil monotherapy significantly improved 6MWD and subjective symptoms. However, there was no significant difference in time to clinical worsening. Oral treprostinil as combination therapy was studied in patients with PH who were already on background therapy of endothelin receptor antagonists and or PDE-5 inhibitors in the FREEDOM-C & FREEDOM-C2 [22, 23] trials. Unfortunately, there was no significant difference between the treatment and placebo arms in the primary endpoint of exercise capacity or the secondary endpoints of symptoms, time to clinical worsening and hemodynamics.Treprostinil is available as oral tablets Orenitram, [24] parenteral infusion Remodulin [25] and inhaled oral solution Tyvaso [26]. Most common side effects include headache, diarrhea, flushing, hypotension, edema [24, 25, 26]. Iloprost is an inhaled prostacyclin which has shown improvement in exercise capacity in patients with PAH. Olschewski, et al. [27] randomized 203 patients with PH to receive inhaled iloprost monotherapy versus placebo and found that inhaled iloprost improved 6MWD, symptoms and hemodynamics [27]. Inhaled iloprost was also evaluated as combination therapy in addition to Bosentan background therapy in 67 patients versus placebo where it was found to improve 6MWD and time to clinical worsening [28]. Iloprost is marketed as Ventavis in the United states for use in patients with Group I PH or PAH to improve exercise tolerance and symptoms. Most common side effects include flushing, cough, headache, nausea, hypotension, syncope and muscle cramps [29].
Prostacyclin Receptor Agonists
Use of prostacyclin analogs has led to research anddevelopment of other similar compounds that could be beneficial in treatment of pulmonary hypertension. Selexipag is the first of its kind and anoral, selective, non prostanoid prostacyclin receptor agonist which acts on prostacyclin receptors to reduce symptoms, delay disease progression and reduce hospitalization in patients with PAH. The GRIPHON study [30] randomized 1156 patients with PH with or without stable doses of endothelin receptor antagonists and or PDE-5 inhibitors to oral Selexipag versus placebo. The primary outcome was a composite of death, disease progression, worsening of PH, initiation of additional therapies, lung transplantation. There was a significant improvement in the primary endpoint amongst the Selexipag group. All-cause mortality or mortality due to PH was not significantly different between the groups. Selexipag is commercially available as Uptravi [31] in the United States [31]. It is approved for use in Group I PH or PAH to delay disease progression and reduce the risk of hospitalization. The common side effects include headache, diarrhea, nausea, jaw pain, flushing and myalgia [31].
Endothelin Receptor Antagonists
Endothelin – 1 is an amino peptide which is produced by the endothelial cells. It is a potent vasoconstrictor of arterial smooth muscle cells in the pulmonary vasculature. It appears to play an important role in the development of pulmonary vasculopathy in pulmonary arterial hypertension. There are two families of endothelin receptors, A (ETA) and B (ETB). ETA is primarily found in the pulmonary vascular smooth muscle cells and when activated mediates a vasoconstrictive response. ETB is primarily found on the endothelial cells and when activated result in vasodilation by producing nitric oxide and prostacyclin. Endothelin receptor antagonists (ETRA) block the actions of endothelin -1 on either endothelin receptors A, B or both [32]. Three ETRAs have been approved for use in PAH. They are Bosentan, ambrisentan and macitentan. Rubin, et al. [33] randomized 213 patients with PAH to receive Bosentan monotherapy versus placebo for a period of 16 weeks and the Bosentan therapy group showed a significant improvement in 6MWD and time to clinical worsening. Galiè N, et al. [34] randomized 185 patients with PAH to receive Bosentan as monotherapy versus placebo and demonstrated that there was a significant improvement in 6MWD and hemodynamics in the therapy group. Bosentan was also studied as combination therapy in 334 PAH patients who were on stable doses of sildenafil in comparison to placebo [35]. The primary endpoint was a composite measure of all-cause mortality, hospitalization for worsening PAH, intravenous prostanoid initiation, atrial septostomy, need for lung transplant. The addition of Bosentan to stable doses of sildenafil did not improve outcomes compared to placebo in this study [35]. Bosentan is available as Tracleer [36] in the United States and is approved for use in Group I PH or PAH patients to improve exercise tolerance and decrease clinical worsening. Common side effects include anemia and respiratory tract infections [36]. The ARIES 1 and 2 trials [37] randomized 202 and 192 PAH patients respectively to oral ambrisentan monotherapy versus placebo for 12 weeks. There was an improvement in 6MWD in both trials. In ARIES 2, a significant improvement was also noted in the time to clinical worsening of PAH but this was not observed in ARIES 1. In the AMBITION trial [38], Ambrisentan was studied in combination with tadalafil as initial therapy in functional class II and III. 500 patients were randomized to receive combination therapy, ambrisentan monotherapy or tadalafil monotherapy. Combination therapy reduced hospitalizations due to worsening disease and improved 6MWD. Ambrisentan is available as Letairis [39] in the United States and is indicated for use in patients with Group I PH or PAH to improve exercise tolerance and to delay disease progression. It is also indicated in combination with tadalafil to improve exercise tolerance, reduce the risk of disease progression and hospitalizations related to PAH. Common side effects include flushing, nasal congestion, peripheral edema and sinusitis [39]. Macitentan was evaluated in the SERAPHIN [40] study where PAH patients were randomized to receive either oral macitentan versus placebo. Patients were allowed additional PH therapy such as PDE-5 inhibitors, oral/inhaled prostacyclin analogs, calcium channel blockers. Macitentan improved symptoms and reduced risk of clinical disease progression in both the mono and combination therapy groups [40]. Macitentan is available as Opsumit [41] in the United States and is indicated in Group I PH or PAH patients to delay disease progression. Common side effects include anemia, headache, bronchitis, nasopharyngitis, urinary tract infection [41].
| Class of Drug | Agent | Route of Administration | Common Side Effects | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| PDE - 5 inhibitors | Sildenafil [9] | Oral | Headache, flushing, dyspepsia | ||||||||
| Tadalafil [10] | Oral | headache | |||||||||
| Guanylate cyclase stimulator | Riociguat [13] | Oral | Headache, diarrhea, nausea, dyspepsia, constipation | ||||||||
| Prostacyclin analogs | Epoprostenol [15,16] | parenteral | dizziness, jaw pain, headache, musculoskeletal pain, flushing, hypotension, dyspnea. |
Treprostinil [24, 25, 26] Oral, parenteral, inhaled headache, diarrhea, flushing, Prostacyclin receptor agonist Selexipag [31] Oral headache, diarrhea, nausea, jaw pain, The World Health Organization (WHO) classifies the severity of symptoms based on functional classes [42]. Class I refers to patients without any limitation of ordinary physical activity. Class II refers to patients with slight limitation of ordinary physical activity. Class III refers to patients with marked limitation of ordinary physical activity. Class IV refers to patients with PH who are unable to perform any physical activity without symptoms. The 2014 CHEST guidelines [43] recommend pharmacologic treatment of patient with PH based on their functional class. Patients who are in class I are generally monitored for disease progression and their underlying etiologies like obstructive sleep apnea (OSA) or systemic sclerosis should be treated. Calcium channel blockers (CCB) can be initiated in individuals who demonstrate pulmonary vasoreactivity on right heart catheterization. The approved pharmacotherapy for PH is recommended to be used in patients who fall under functional classes II, III and IV. The 2014 CHEST guidelines recommend monotherapy alone for functional class II and III. For patients in functional class II or III who have failed CCB, monotherapy with ETRA, PDE-5 inhibitors or soluble guanylate cyclase stimulators is recommended. However more recent literature suggests that combination therapy as an initial strategy could be beneficial even in patients with functional class II or III [38]. For patients in functional class III or IV who experience rapid progression of symptoms monotherapy directly with parenteral prostacyclin analogs can be considered. Infunctional class III or IV patients who are symptomatic on one class of PH therapy, combination therapy with a second class of agents can be considered. If symptoms persist despite two classes of PH therapy, a third class of agents can also be considered. Generally, in patients who are symptomatic on ETRA or PDE-5 inhibitor, inhaled prostacyclin analogs are recommended as additional therapy. In patients who are unable to tolerate intravenous or subcutaneous prostacyclin analogs as first line therapy the alternative is ETRA with an inhaled prostacyclin analog [43]. The available therapies and their usage in the different functional classes of PH patients is summarized based on the available literature.
| Functional class | Treatment recommendation | Treatment status | First line | Second line | Combination | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| therapy | therapy | therapy | ||||||||||
| I | Treat underlying conditions like OSA, systemic sclerosis. | Treatment naïve | CCB [43] | Not recommended [43] | Not recommended [43] | |||||||
| II | Approved pharmacotherapy | Failed CCB or treatment naive | ETRA, PDE -5 inhibitors, soluble guanylate cyclase stimulators | Tadalafil [38] | Ambrisentan +tadalafil [38] |
Table 2: Pharmacotherapy of PH based on WHO functional class.
| [43] | |||||
|---|---|---|---|---|---|
| III Stable symptoms | Approved pharmacotherapy | Failed CCB or treatment naive | ETRA, PDE -5 inhibitors, soluble guanylate cyclase stimulators [43] | Parenteral prostacyclin analogs – intravenous or inhaled [43] | 1/2 classes of oral agents + parenteral prostacyclin analogs [43] |
| III Rapid progression of symptoms | Approved pharmacotherapy | No prior therapy or symptomatic on PH pharmacotherapy | Parenteral prostacyclin analogs – intravenous or subcutaneous [43] | ETRA, PDE -5 inhibitors, soluble guanylate cyclase stimulators [43] | 1/2 classes of oral agents + parenteral prostacyclin analogs [43] |
| IV | Approved pharmacotherapy | No prior therapy or symptomatic on PH pharmacotherapy | Parenteral prostacyclin analogs – intravenous/subcutaneous OR ETRA + inhaled prostacyclin analog [43] | ETRA, PDE -5 inhibitors, soluble guanylate cyclase stimulators [43] | 1/2 classes of oral agents + parenteral prostacyclin analogs [43] |
Table 3: Pharmacotherapy of PH based on WHO functional class.
Conclusion
Pharmacotherapy for pulmonary hypertension is fast growing with pharmacologic agents targeting various facets of vasoreactivity and thereby affecting pulmonary vascular resistance. Despite numerous advances and new medical therapy being available for pulmonary hypertension, most of the available specific pharmacologic agents have been studied and approved for use only in Group I PH or PAH. In addition, Epoprostenol is the only approved agent even within the PAH subgroup which has thus far proven to improve survival. Significant research in pharmacologic and other interventions is required to improve long term outcomes and survival in patients with PAH.
1. Galie N, Humbert M, Vachiery JL, Gibbs S, Lang I, et al.
(2016) ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J 37(1): 67-119.
2. Simonneau G, Gatzoulis MA, Adatia I, Celermajer D,
Denton C, et al. (2013) Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol 62(25): 34-41.
3. Buckley MS, Staib RL, Wicks LM, Feldman JP (2010)
Phosphodiesterase-5 inhibitors in management of pulmonary hypertension: safety, tolerability, and efficacy Drug Health Patient Saf 2: 151-61.
4. Galie N, Ghofrani HA, Torbicki A, Barst RJ, Rubin LJ, et al. (2005) Sildenafil citrate therapy for pulmonary arterial hypertension. N Engl J Med 353(20): 2148- 2157.
5. Rubin LJ, Badesch DB, Fleming TR, Galie N,
Simonneau G, et al. (2011) Long-term treatment with sildenafil citrate in pulmonary arterial hypertension: the SUPER-2 study. Chest 140(5): 1274-1283.
6. Galie N, Brundage BH, Ghofrani HA, Oudiz RJ,
Simonneau G, et al. (2009) on behalf of the Pulmonary Arterial Hypertension and Response to Tadalafil (PHIRST) Study Group Tadalafil therapy for pulmonary arterial hypertension. Circulation 119(22): 2894-2903.
7. Oudiz RJ, Brundage BH, Galie N, Ghofrani HA,
Simonneau G, et al. (2012) Botros FT, et al. PHIRST study group. Tadalafil for the treatment of pulmonary arterial hypertension: a double-blind 52-week uncontrolled extension study. J Am Coll Cardiol 60(8): 768-774.
8. Jing ZC, Yu ZX, Shen JY, Wu BX, Xu KF, et al. (2011)
Vardenafil in pulmonary arterial hypertension: a randomized, double- - blind, placebo controlled study. Am J Respir Crit Care Med 183(12):1723-1729.
9. Revatio (2014) New York, (NY) Pfizer Inc; Package
insert.
10. Adcirca (2015) Indianapolis (IN) Eli Lilly and Company; Package insert.
11. Stasch JP, Evgenov OV (2013) Soluble guanylate cyclase stimulators in pulmonary hypertension. Handb Exp Pharmacol 218: 279-313.
12. Ghofrani HA, Galie N, Grimminger F, Grunig E,
Humbert M, et al. (2013) Riociguat for the treatment of pulmonary arterial hypertension. N Engl J Med 369(4): 330-340.
13. Adempas (2014) Whippany NJ, Bayer Healthcare;
Package insert.
14. LeVarge BL (2015) Prostanoid therapies in the management of pulmonary arterial hypertension. Ther Clin Risk Manag 11: 535-547.
15. Flolan (2008) Research triangle park NC, Glaxosmithkline; Package insert.
16. Veletri (2016) San Francisco CA, Actelion Pharmaceuticals US Inc; Package insert.
17. Barst RJ, Rubin LJ, Long WA, McGoon MD, Rich S, et al.
(1996) A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. N Engl J Med 334(5): 296-301.
18. Badesch DB, Tapson VF, McGoon MD, Brundage BH,
Rubin LJ, et al. (2000) Continuous intravenous epoprostenol for pulmonary hypertension due to the scleroderma spectrum of disease. A randomized, controlled trial. Ann Intern Med 132(6): 425-434.
19. Simonneau G, Barst RJ, Galie N, Naeije R, Rich S, et al.
(2002) Continuous subcutaneous infusion of treprostinil, a prostacyclin analogue, in patients with pulmonary arterial hypertension: a double-blind, randomized, placebo-controlled trial. Am J Respir Crit Care Med 165(6): 800-804.
20. McLaughlin VV, Benza RL, Rubin LJ, Channick RN,
Voswinckel R, et al. (2013) Addition of inhaled treprostinil to oral therapy for pulmonary arterial hypertension: a randomized controlled clinical trial. J Am Coll Cardiol 55(18): 1915-1922.
21. Jing ZC, Parikh K, Pulido T, Jerjes-Sanchez C, White RJ,
et al. (2013) Efficacy and safety of oral treprostinil monotherapy for the treatment of pulmonary arterial hypertension: a randomized, controlled trial. Circulation 127(5): 624-633.
22. Tapson VF, Torres F, Kermeen F, Keogh AM, Allen RP,
et al. (2012) Oral treprostinil for the treatment of pulmonary arterial hypertension in patients on background endothelin receptor antagonist and/or phosphodiesterase type 5 inhibitor therapy (the FREEDOM-C study): a randomized controlled trial. Chest 142(6): 1383-1390.
23. Tapson VF, Jing ZC, Xu KF, Pan L, Feldman J, et al.
(2013) Oral treprostinil for the treatment of pulmonary arterial hypertension in patients receiving background endothelin receptor antagonist and phosphodiesterase type 5 inhibitor therapy (the FREEDOM-C2 study): a randomized controlled trial. Chest 144(3): 952-958.
24. Orenitram (2016) Research triangle park, NC. United
therapeutics corp; Package insert.
25. Remodulin (2014) Research triangle park, NC. United
therapeutics corp; Package insert.
26. Tyvaso (2009) Research triangle park, NC. United
therapeutics corp; Package insert.
27. Olschewski H, Simonneau G, Galie N, Higenbottam T,
Naeije R, et al. (2002) Inhaled iloprost for severe pulmonary hypertension. N Engl J Med 347(5): 322- 329.
28. McLaughlin VV, Oudiz RJ, Frost A, Tapson VF, Murali
S, et al. (2006) Randomized study of adding inhaled iloprost to existing bosentan in pulmonary arterial hypertension. Am J RespirCrit Care Med 174(11): 1257-1263.
29. Ventavis (2013) San Francisco CA, Actelion Pharmaceuticals US Inc; Package insert.
30. Sitbon O, Channick R, Chin KM, Frey A, Gaine S, et al.
(2015) For the GRIPHON investigators. Selexipag for the Treatment of Pulmonary Arterial Hypertension. N Engl J Med 373(26): 2522-2533.
31. Uptravi (2015) San Francisco CA, Actelion Pharmaceuticals US Inc; Package insert.
32. Channick RN, Sitbon O, Barst RJ, Manes A, Rubin LJ
(2004) Endothelin receptor antagonists in pulmonary arterial hypertension. J Am Coll Cardiol 43(12): 62- 67.
33. Rubin LJ, Badesch DB, Barst RJ, Galie N, Black CM, et al. (2002) Bosentan therapy for pulmonary arterial hypertension. N Engl J Med 346(12): 896-903.
34. Galie N, Rubin L, Hoeper M, Jansa P, Al-Hiti H, et al.
(2008) Treatment of patients with mildly symptomatic pulmonary arterial hypertension with bosentan (EARLY study): a double-blind, randomised controlled trial. Lancet 371(9630): 2093-2100.
35. McLaughlin V, Channick RN, Ghofrani HA, Lemarie JC,
Naeije R, et al. (2015) Bosentan added sildenafil therapy in patients with pulmonary arterial hypertension. Eur Respir J 46(2): 405-413.
36. Tracleer (2016) San Francisco CA, Actelion Pharmaceuticals US Inc; Package insert.
37. Galie N, Olschewski H, Oudiz RJ, Torres F, Frost A, et al. (2008) Ambrisentan for the treatment of pulmonary arterial hypertension: results of the ambrisentan in pulmonary arterial hypertension, randomized, double-blind, placebo-controlled, multicenter, efficacy (ARIES) study 1 and 2. Circulation 117(23): 3010-3019.
38. Galie N, Barbera JA, Frost AE, Ghofrani HA, Hoeper
MM, et al. (2015) Initial Use of Ambrisentan plus Tadalafil in Pulmonary Arterial Hypertension. N Engl J Med 373(9): 834-844.
39. Letairis (2015) Foster city, CA. Gilead Sciences, Inc;
Package insert.
40. Mehta S, Sastry BK, Souza R, Torbicki A, Ghofrani HA,
et al. (2017) Macitentan Improves Health-Related Quality of Life for Patients with Pulmonary Arterial Hypertension: Results From the Randomized Controlled SERAPHIN Trial. Chest 151(1): 106-118.
41. Opsumit (2016) San Francisco, CA. Actelion Pharmaceuticals US Inc; Package insert
42. Barst RJ, McGoon M, Torbicki A, Sitbon O, Krowka MJ,
et al. (2004) Diagnosis and differential assessment of pulmonary arterial hypertension. J Am Coll Cardiol 43(12): 40-47.
43. Taichman DB, Ornelas J, Chung L, Klinger JR, Lewis S,
et al. (2014) Pharmacologic therapy for pulmonary arterial hypertension in adults: CHEST guideline and expert panel report Chest 146(2): 449-475.
- Bedside Pulmonary Rehabilitation – Mandatory and Cost- Effective Tools
- The Role of Chest Radiology in Traumatic Injuries: A Comprehensive Narrative Review
- Pseudosepsis in Acute Inflammation of the Lung
- An Overview of Lung Injury in Covid-19: Evaluating the Impact of Re-Exposure and Emerging Variants
- Fibreoptic Bronchoscopy-its Role in Pulmonary Medicine-Current Trends in Intensive Care Unit
- Retrospective Study on the Efficacy of Homoeopathic Medicines in the Treatment of Acute Rhinitis