Systemic Lupus Erythematosus Female with (Diffuse Large BCell) Non-Hodgkin’s Lymphoma
Systemic lupus erythematosus (SLE) is an autoimmune disease with multisystem complications arising from both underlying disease activity and therapy-related side effects. SLE’s association with lymphoma is a well-established phenomenon. Studies have reported a higher incidence of lymphoma in the SLE population compared with healthy cohorts [1,2]. A 45-year-old woman with systemic lupus erythematosus (SLE) presented with fever, cough, sputum, loss of appetite and fatigue for 4 months. Before that time, her (SLE) symptoms had been well controlled on hydroxyl chloroquine, azathioprine, and small dose prednisone. Physical exam at initial evaluation was remarkable for bilateral inspiratory crackles. Laboratory investigations were normal. Computed tomography to chest showed bilateral cavitary pulmonary nodules and masses. Bronchoscopy with transbronchial biopsy was done. The histopathology showed diffuse large B-cell non-Hodgkin’s lymphoma. Patient referred to oncology service, where they started her on 4 cycles of R-CHOP, followed by 4cycles of high dose chemotherapy (HDCT). She underwent Hematopoietic stem cell transplantation, and achieved complete remissions.
Introduction
Presenting Concern
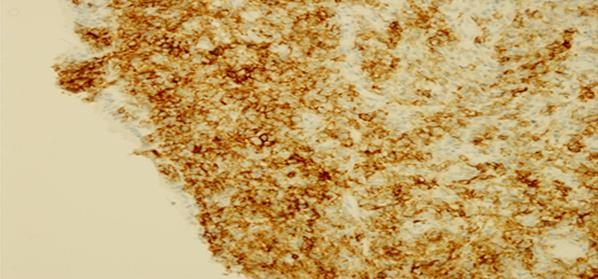
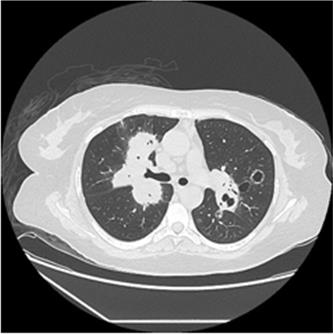
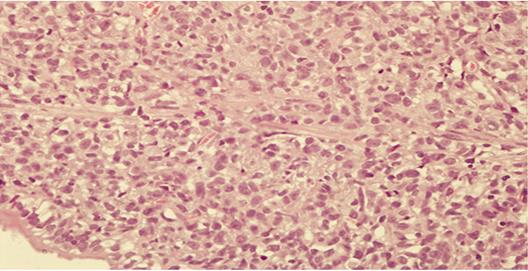
A 45 -year-old married, Saudi female, with a 4- year history of systemic lupus erythematosus (SLE), and chronic hepatitis B presented in February of 2017 with fever, cough, sputum, loss of appetite and fatigue for 4 months. Before that time, her (SLE) symptoms had been well controlled on hydroxyl chloroquine, azathioprine, and small dose prednisone. Physical exam at initial evaluation was remarkable for bilateral inspiratory crackles. Laboratory investigations were normal. Chest X- ray, and Computed tomography to chest showed bilateral cavitary pulmonary nodules and masses. Bilateral innumerable lung nodules and masses some of them shows cavitation and air bronchogram more predominant at the lower lobes bilaterally the largest one seen at the right middle lobe adjacent to the heart. There is a cyst in the left lower lobe multiple enlarged mediastinal lymph nodes. Bronchiectatic changes are appreciated at the left ligulae (Figure 1,2). Bronchoscopy was done. Bronchoalveolar lavage (BAL) for acid fast bacilli (AFB) and funguses two times were negative. The histopathology of trans bronchial biopsy showed proliferation of round to ovoid cells with scant cytoplasm, and dense nuclear chromatin showing prominent nucleoli, arranged as diffuse dyscohesive sheets. Immunohistochemistry done, tumor cells are positive for CD45, CD20, and bcl-2 negative pan for pan CK, CD 56, bcl-6, CD 10, and Tdt. CD 3 highlights the cell population. k67 index is >80 (Figure 3,4,5). Patient referred to oncology service, where they started her on 4 cycles of R- CHOP followed by 4 cycles of high dose chemotherapy (HDCT). She underwent Hematopoietic stem cell transplantation, and achieved complete remissions. After which she started to become neutropenic, and to have high grade fever. After mulltidisplinary discussion. She underwent Hematopoietic stem cell transplantation, and achieved complete.
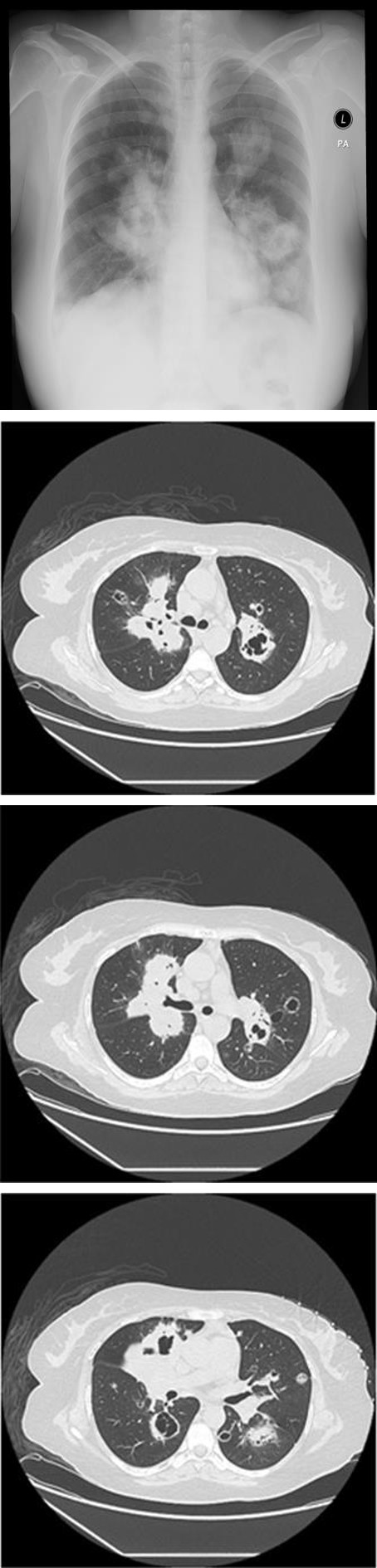
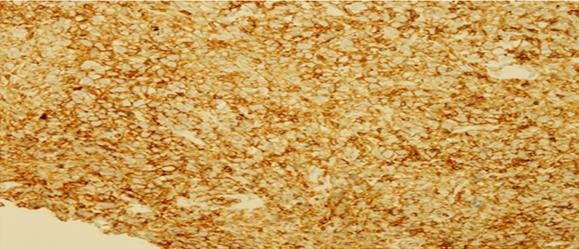
Figure 2A: Multiple enlarged mediastinal lymph nodes.
Figure 2B: Bilateral innumerable lung nodules, and masses some of them shows cavitation and air bronchogram.
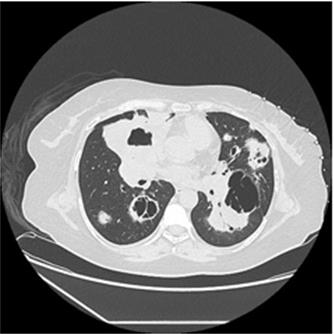
Figure 2C: Bronchiectatic changes are appreciated at the left ligula. There is a cyst in the left lower lobe.
Discussion
A recent meta-analysis which included 16 observational studies showed a mildly increased risk of overall cancer in SLE compared with the general population [3]. This risk is most pronounced in SLE related non-Hodgkin’s lymphoma with reported relative risk estimates ranging widely from 4.39 to 44.4 in various studies. NHL risk is determined by various factors, including age, sex, and race. NHL is more common in men, and among white subjects [4].
NHL can be divided into two general prognostic groups: indolent lymphomas and more aggressive (intermediate or high grade) lymphomas. (Diffuse large B cell and Burkitt’s) lymphoma. The diffuse large B cell subtype makes up about 30% of all NHL lymphomas in the general population [5].
There is genetic abnormalities association between SLE and NH. The presence of chromosomal abnormalities, represent common pathways linking SLE and lympho proliferative malignancies. Chromosomal translocations, which may result from uncontrolled lymphocyte activity in active SLE allow malignant transformation [6]. The effect of immunosuppressive agents and viral exposures had been evaluated.
In recent small case–control study from Sweden compared 16 cases of NHL arising in SLE with 26 cancer- free control patients with SLE, the use Cyclophosphamide or azathioprine did not elevate lymphoma risk [7] while in another study the relative risk of NHL after cyclophosphamide exposure was 1.1 (95% CI: 0.3–3.3) and after azathioprine was 0.9 (95% CI: 0.5–2.5). The histology of the NHL cases in SLE suggests that these lesions also are derived from a lymphocyte already been exposed to antigen [8].
The current treatment make the median survival for NHL exceeds 5 years [9]. Aggressive tumor types , late stage of presentation which more common in SLE, and therapeutic measures which maybe inappropriately withheld from patients with SLE who develop cancer ,these might lead to a lower than expected survival [10].
Diffuse large B-cell lymphomas (DLBCL) can be divided into germinal centre (GC-DLBCL) and post germinal centre (post GC-DLBCL) groups by applying Immunohistochemical antibodies. These subgroups respond differently to chemotherapy. GC-DLBCL group shows better response to CHOP chemotherapy regimen [11]. The R-CHOP regimen resulted in the cure of approximately 50% of patients [12]. Diffuse large B cell lymphoma (DLBCL) is a highly proliferative; this makes it a suitable target for high dose chemotherapy HDCT [13].
Out of 258 patients with lupus and secondary ant phospholipid syndrome (APS), 6 developed lymphomas (4 DLCBL, 1 Hodgkin’s and 1 indolent lymphocytic lymphoma). The first 5 patients were treated with high dose chemotherapy (HDCT) and achieved complete remissions (CR) with a follow-up comprised between 13 and 172 months. One patient relapsed of lymphoma and died 15 months following CR, with persistent lupus serology. One patient achieved complete remission (CR) of both diseases [13].
Hematopoietic stem cell transplantation can be used for severe autoimmune diseases (SADS) to eradicate the last cancer stem cell [14].
Conclusion
Patients with systemic lupus erythematosus (SLE) are at increased risk of developing non-Hodgkin’s lymphoma (NHL). Patient with aggressive tumor types or late stage of presentation will have lower than expected survival. Active cancer screening is required in SLE patients with long disease duration.
References
-
Bernatsky S, Boivin JF, Joseph L, Rajan R, Zoma A, et al. (2005) An international cohort study of cancer in systemic lupus erythematosus. Arthritis Rheum 52(5):1481-1490. 2. Ramsey-Goldman R, Clarke A (2001) Double trouble: are lupus and malignancy associated? Lupus 10(6): 388-391. 3. Cao L, Tong H, Xu G, Liu P, Meng H, et al. (2015) Systemic lupus erythematous and malignancy risk: a meta-analysis. PLoS ONE 10(4): e0122964. 4. Skarin AT, Dorfman DM (1997) Non-Hodgkin’s lymphomas: current classification Skarin AT, Dorfman DM. Non-Hodgkin’s lymphomas: current classification and management. CA Cancer J Clin 47(6): 351-372. 5. Freedman A, Nadler L (2000) Non Hodgkin’s lymphomas. In: Bast R, Kufe W, Pollock R, Weichselbaum R, Holland J, Frei E (eds). Cancer medicine. Canada: BC Decker Inc. 6. Xu Y, Wiernik P (2001) Systemic lupus erythematosus and B-cell hematologic neoplasm. Lupus 10(12): 841- 850. 7. Lofstrom B, Backlin C, Sundstrom C, Ekbom A, Lundberg IE (2007) A closer look at non-Hodgkin’s lymphoma cases in a national Swedish systemic lupus erythematosus cohort: a nested case-control study. Ann Rheum Dis 66(12): 1627-1632. 8. Bernatsky S, Ramsey-Goldman R, Rajan R, Boivin JF, Joseph L, et al. (2005) Non-Hodgkin’s lymphoma insystemic lupus erythematosus. Ann Rheum Dis 64(10): 1507-1509. 9. Jemal A, Tiwari RC, Murray T, Ghafoor A, Samuels A, et al. (2004) Cancer statistics, 2004. CA Cancer J Clin 54(1): 8-29. 10. Benk V, Al-Herz A, Gladman D, Urowitz M, Fortin PR (2005) Role of radiation therapy in patients with a diagnosis of both systemic lupus erythematosus and cancer. Arthritis Rheum 53(1): 67-72. 11. Hassan U, Mushtaq S, Mamoon N, Hussain Asghar A, Ishtiaq S (2012) “Prognostic sub-grouping of diffuse large B-cell lymphomas into germinal centre and post germinal centre groups by immunohistochemistry after 6 cycles of chemotherapy”. Asian Pacific Journal of Cancer Prevention, 13(4): 1341-1347. 12. Zhang Q, Wang J, Yu Z (2009) The effect of subgroups of diffuse large B-cell lymphoma. Onkologie 32: 719- 723. 13. Rossi E, Catania G, Truini M, Ravetti GL, Grassia L, et al. (2011) Patients with systemic lupus erythematosus SLE) having developed malignant lymphomas. Complete remission of lymphoma following high-dose chemotherapy, but not of SLE. Clinical and Experimental Rheumatology 29(3): 555– 559.
-
Jayne D, Tyndall A, Marmont A, Farge D, Zhao X, et al. (2004) Autologous stem cell transplantation for systemic lupus erythematosus. Lupus 13(3): 168-176.
- Bedside Pulmonary Rehabilitation – Mandatory and Cost- Effective Tools
- The Role of Chest Radiology in Traumatic Injuries: A Comprehensive Narrative Review
- Pseudosepsis in Acute Inflammation of the Lung
- An Overview of Lung Injury in Covid-19: Evaluating the Impact of Re-Exposure and Emerging Variants
- Fibreoptic Bronchoscopy-its Role in Pulmonary Medicine-Current Trends in Intensive Care Unit
- Retrospective Study on the Efficacy of Homoeopathic Medicines in the Treatment of Acute Rhinitis