High Altitude Pulmonary Edema at Moderate Altitude: Report of Two Cases and Review of Literature
High altitude pulmonary edema (HAPE) is a form of pulmonary edema following a rapid exposure to high altitudes over 2,500 meters (m). HAPE is essentially due to a persistent imbalance between the forces that drive water into the airspace and the biologic mechanisms for its removal. As pulmonary edema progresses, cough becomes aggravated and breathlessness is felt even at rest. Acute respiratory failure and gurgling sounds from the chest indicate advanced cases. The most effective and reliable treatment is immediate descent and/or adequate flow supplemental oxygen to maintain arterial saturation above 90%, accompanied by rest from strenuous physical activity. This pathological condition ca be extremely dangerous and, some cases, fatal. In presence of predisposing factors, HAPE can also occur at moderate altitudes. We based our work on two cases which we observed in our Unit.
Introduction
High altitude pulmonary edema (HAPE) is a non- cardiogenic form of pulmonary edema [1], that develops in susceptible individuals following their rapid exposure to high altitudes over 2,500 m [2]. High altitude is arbitrarily classified as high (1,500 to 3,500 m), very high (3,500 to 5,500 m), and extreme (above 5,500 m) [3]. The symptoms of HAPE are characterized early by cough, progressive dyspnea with exertion, decreased exercise tolerance and elevated body temperature (generally not exceeding 38.5° C), usually developing within two to four days after arrival at high altitude [4]. As pulmonary edema progresses, cough gets worse and worse and breathlessness appears even at rest. Chest gurgling sounds and pink frothy sputum along with cyanosis indicates advanced cases. Arterial blood gas measurements show hypoxemia and respiratory failure [5] and it is possible to find flocculent shadows on chest X-ray [6]. In advanced cases, HAPE may be associated with high altitude cerebral edema, characterized by swelling of brain tissue due to fluid leakage, and it shows symptoms as ataxia and decreased levels of consciousness. Studies have shown that the hypoxic environment at high altitudes impairs physical performance, sleep, and mental performance [7]. Two populations are affected by HAPE. The first involves well-acclimatized alpine residents returning from low altitudes (re-entry HAPE) and the second involves rapids ascent of unacclimatized lowlanders. Altitude, ascent rate and individual susceptibility are the major determinants of HAPE [8]. HAPE is rare after one week of acclimatization at a particular altitude [9]. This condition is based on physiological adaptations to high altitude, as polycythemia (which helps to increase oxygen carrying capacity of blood), hyperventilation (increasing alveolar ventilation), acid-base changes (renal excretion of bicarbonate to oppose the respiratory alkalosis) [10]. In a general alpine mountaineering population, the prevalence of HAPE was < 0.2% [11] and the incidence of HAPE among Himalayan trekkers and climbers in the Alps is around 4% depending on the rate of ascent [12]. Our hospital is in northern Italy, about 260 m, surrounded by the Alps and Dolomites with altitudes ranging to 3,905 m. During the year, seven million tourists come to play sports and spend their holidays in our region [13]. Many of them are “lowlanders” (natives from areas at sea level) and do not always have the opportunity or awareness to perform proper acclimatization. Here we describe the development of two patients affected by HAPE which were skiing in Winter in our country.
Case description
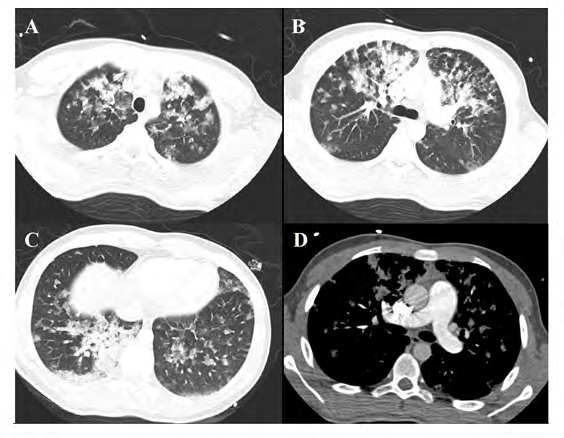
Case 1: this patient was a 16-years-old boy, in good health status. He started to feel breathless with dry cough and white frothy sputum, while he was skiing on the Alps glaciers (from 2000 to 3220 m) in South Tyrol, Italy. He was transported by helicopter into our hospital and during the flight he was treated with intravenous solumedrol 500 mg. Upon arrival in the Emergency Room, a blood gas analysis (BGA) was performed that showed acute respiratory failure (pO2 47 mmHg, pCO2 29 mmHg, pH 7.43, FiO2 21%). Blood analysis revealed D-dimer 464 ng/ml, Procalcitonin 0,16, WBC 26.61 x1000/μl, RCP 1,85 mg/dL. A Chest-X-ray documented multiple bilateral parenchymal thickenings (Figure 1A). He was admitted in Intensive Care Unit (ICU), subjected to Thorax CT, which documented several bilateral parenchymal opacities bilateral of uncertain nature with asymmetrical and heterogeneous distribution (Figure 2A-2C), increased pulmonary artery caliber compatible with pulmonary hypertension (Figure 2D), no signs of pulmonary embolism. During the hospitalization in ICU patient underwent non- invasive ventilation (NIV) for few hours and he got rapidly better. After 24 hours the patient was admitted in our Respiratory Intensive Care Unit (RICU). Patient underwent echocardiography that documented moderate pulmonary hypertension, a normal biventricular systolic function, not evidence of vegetations. Autoimmune screening and microbiological tests (blood culture, molecular screening of respiratory viruses) were performed and resulted negative. Patient received oxygen and steroids (methylprednisolone).
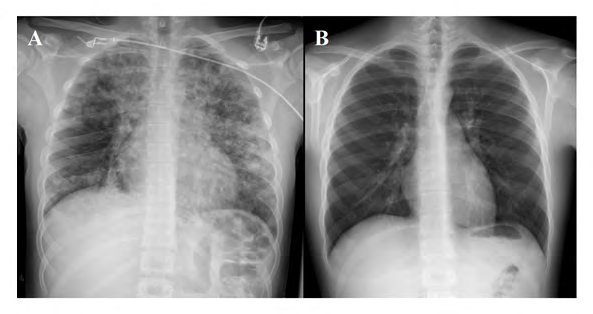
The subsequent radiographs documented the progressive disappearance of pulmonary thickenings (Figure 1B), and a new echocardiography had also documented the normalization of pulmonary pressure. The BGA documented the perfect normalization of the gas exchanges (pH 7.43, pO2117 mmHg, pCO2 35 mmHg, HCO3 3- 23 mmol/l, SpO2 99%). We discharged the patient without therapy, with the recommendation of observing a rest period of 10 days. We recommended further not to reach high altitude level (above 1,000 m) without a period of progressive acclimatization (for example 500 m per day).
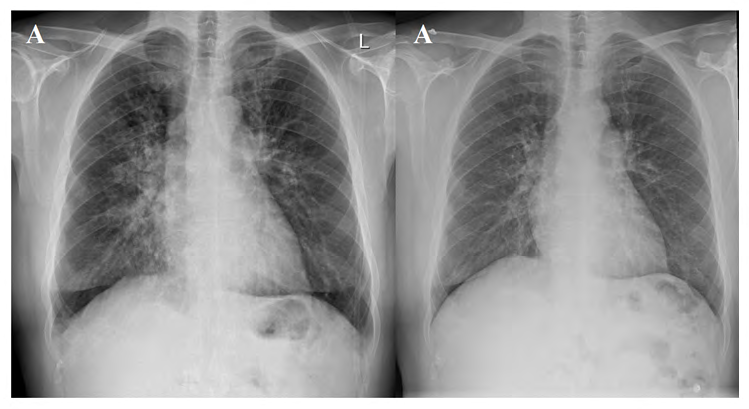
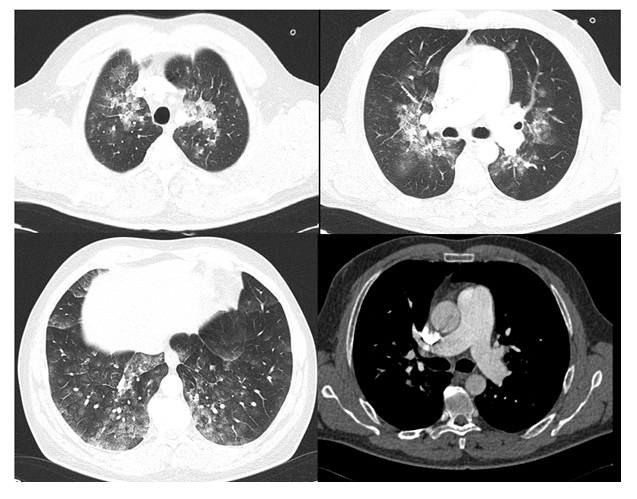
Case 2: the patient was a 47-years-old man, in good health status, no smoker. After 2 days spent in Dolomites (from 2,835 m to 3,269 m), the patient reported dyspnea and headache. During the night, he developed dry cough and hemoptysis. He was transported to ICU in our Hospital, where he undergone blood analysis (WBC 14.55 x1000/μl, D-dimer 0.42 mg/l, CRP 1.31 mg/dl, BNP 878 pg/dl), Chest X-ray (Figure 3A) and BGA that showed acute respiratory failure. Echocardiography demonstrated pulmonary hypertension (PAPs 70 mmHg) and CT-Thorax scan bilateral “ground-glass” thickenings (Figure 4A-4C), pulmonary artery enlargement (Figure 4D). Autoantibodies, blood cultures and molecular screening of respiratory viruses were negative. Oxygen therapy improved dyspnea and new blood analysis showed decreased BNP. After patient had been admitted in our RICU, he was treated with oxygen, oral corticosteroids, and antibiotics, with a rapid resolution of symptoms. The subsequent echocardiography showed a reduction of PAPs (39 mmHg). After three days Chest-X-ray was negative (Figure 3B) and the patient was discharged in good health status.
Discussion
HAPE is essentially due to a persistent imbalance between the forces that drive water into the airspace and the biologic mechanisms for its removal [14]. Hypoxia is the trigger that results in a complex cascade of events leading to HAPE [15]. The hallmark of this condition is hypoxic pulmonary vasoconstriction that exposes pulmonary capillaries to a high pressure, damaging their walls and leading to a high- permeability form of edema [16]. The hydrostatic stress causes dynamic changes in the permeability of the alveolar capillary barrier and mechanical injurious damage leading to leakage of large proteins erythrocytes into the alveolar spaces in the absence of inflammation. Broncho-alveolar lavage and hemodynamic pressure measurements in humans confirm that elevated capillary pressure induces a high-permeability non-inflammatory lung edema [17]. Exaggerated pulmonary hypertension is hallmark of HAPE and several observations indicate that it contributes to its pathogenesis [18].
Susceptible individuals exhibit a marked rise in pulmonary arterial pressure on exposure to hypoxia mediated by pulmonary arteriolar vasoconstriction and a greater rise in pulmonary arterial pressure on exercise in a normal oxygen environment, indicating a hyperactive pulmonary circulation [19]. Hypoxic pulmonary hypertension may be mediated via at least three potential mechanisms: defective pulmonary nitric oxide synthesis; exaggerated endothelin‐1 synthesis; and exaggerated sympathetic activation. A defect in alveolar transepithelial sodium transport has also been suggested [20]. Nitric oxide and endothelin-1 are important endothelial derived vasodilator and vasoconstrictor mediators, respectively, in the pulmonary circulation. To cause pulmonary edema, the elevated pulmonary artery pressure has to be transmitted to the capillaries. To explain this phenomenon, Scherrer U, et al. postulated that there exist pulmonary regions where capillaries are not protected by constricted resistance vessels. They demonstrated that the inhalation of nitric oxide, which induced a significantly greater reduction of the pulmonary-artery pressure in HAPE-prone than HAPE–resistant subjects, redistributed blood flow away from edematous regions of the lungs and toward non-edematous regions. This suggests that defective pulmonary endothelial nitric oxide synthesis is one of the mechanisms contributing to exaggerated hypoxic pulmonary hypertension in HAPE [20]. Talbot NB, et al. demonstrated that in human’s endothelin-1 infusion sufficient to raise circulating concentrations by tenfold have no effect on hypoxic pulmonary vasoconstriction after 2 hours. These data suggest that the early immediate rise in pulmonary arterial pressure with hypoxia may not be related to changes in circulating endothelin-1, but that with longer hypoxic duration differences in endothelin-1 synthesis and/or clearance may become more important [21]. Cardiovascular adjustments to hypoxia are mediated, at least in part, by the sympathetic nervous system. At high altitude, HAPE-prone mountaineers display exaggerated sympathetic activation that is directly related to exaggerated hypoxic pulmonary hypertension [22]. Most importantly, the sympathetic activation precedes the development of lung edema, suggesting that exaggerated sympathetic activity contributes to exaggerated hypoxic pulmonary hypertension and pulmonary edema in HAPE-prone subjects [23].
The real challenge of these two cases was the diagnosis of HEPA. It is generally based on medical history, exposure at a consistent altitude, typical symptoms, and signs. These illnesses can occur in young and healthy individuals within the first few days of exposure to high altitude. In addition, high altitude may aggravate pre-existing illnesses or lead to a first manifestation of an illness that was asymptomatic at low altitude and therefore unknown [24]. Although we are in a mountainous region, it’s not usual for us to see such HEPA cases, probably because our mountain’s altitude is not so elevated as the one required to cause these disorders and people remain briefly at potentially dangerous altitudes. On the other hand, Gabry, et al. described a group of 52 patients, admitted into Emergency department of a community hospital in the French Alps, who acquired pulmonary edema at a moderate altitude of 1,400 to 2,400 m. They suggested that HAPE at moderate altitudes is more frequent than usually reported [25]. Otherwise, Schommer, et al. demonstrated that more intense physical activity associated with high altitude training or mountaineering does not increase prevalence or severity of AMS at these altitudes [26]. Other authors suggested that pulmonary edema tends to occur at lower altitudes when pulmonary circulation is abnormal: thromboembolic pulmonary hypertension, anomalous pulmonary venous drainage into the superior vena cava, and unilateral pulmonary artery occlusion from granulomatous mediastinitis [27, 28, 29, 30].
Furthermore, many differential diagnoses can be confused with HAPE. Pneumonia is the most frequent among these diagnoses. Other conditions are pulmonary embolism, acute heart failure, acute coronary syndrome, bronchitis, viral upper respiratory tract infection, bronchospasm, reactive airway disease, and exercise-associated hyponatremia [31, 32].
The history of the patients allowed us to exclude some conditions (e.g. coronary syndrome). The patient had no cardiological illness and they had good heart function after the cardiological evaluation, thus helping to confirm that the pulmonary edema was not the result of left ventricular failure. Pulmonary hypertension reduced quickly too, with a non-specific therapy (e.g. oxygen, NIV, diuretics). To achieve the aim, we have done an exclusion diagnosis: first of all we have excluded in both patients the presence of respiratory infections that could justify the clinical and radiological signs. In fact, blood cultures were in normality range, only the CRP and WBC in both patients were high. They had not strong evidences of infection and the rapid clinical and instrumental responses led us to different positions. The clinical and radiological presentation of the cases guided us to investigate the presence of any autoimmune conditions. The auto-antibody pattern was also negative for both patients.
Nevertheless, the most important diagnostic tools of HAPE are chest X-rays or CT scan. HAPE presents usually the following features: Chest X-rays findings including decreased pulmonary transmittance, increased or obscure lung markings, ground glass-like changes or patchy shadows in the lung; Lung-CT findings including increased and enlarged lung markings, ground glass-like changes, nodule-like shadows, scattered or isolated alveolar edema of terminal bronchioles and slim reticulate shadows [33]. Many acute lung diseases can occur with a prevailing pattern of multiple lobular opacities. The most frequent causes are infections (e.g. viral infections, pneumonia P. jirovecii or M. pneumoniae); sometimes from pulmonary edema. Rarely fat embolism syndrome in patients with polytrauma and multiple bone fractures [34].
When we investigated deeper the history of the patients, we have found two interesting news. Patient 1 suffered by a mild cold for the past three days before the ICU admission and Patient 2 said that he suffered in 2010 from a similar episode (cough, dyspnea, headache), while he was near to Stelvio mountain (3,000 m, Lombardia, Italy). In this case he did not need to be taken to the hospital.
Children may be more susceptible to HAPE because of increased vascular reactivity, immature control of breathing, and increased frequency of respiratory illnesses [35]. A high rate of preceding concurrent respiratory tract infection (RTI) was found in children who developed HAPE [36]. Moreover, upper respiratory symptoms have been associated with the development of acute mountain sickness (AMS) that includes headaches, vomiting, tiredness, trouble sleeping, and dizziness. [37]. Cold can lead to an increase in pulmonary intravascular pressure and may contribute to the development of AMS [38, 39]. Durmowicz, et al. showed a strong association between the presence of a preexisting illness and the development of HAPE in children visiting high altitude and also, but to a lesser extent, in adults. They suggested that though these illnesses with their subsequent release of inflammatory mediators may cause only mild discomfort at sea level. Instead, when superimposed on exposure to high altitude and perhaps exercise, a previous subclinical increase in capillary permeability may now predispose the child visiting high altitude to HAPE [40]. It is conceivable that any process enhancing the permeability of the alveolar-capillary barrier decreases the pulmonary capillary pressure threshold above which pulmonary edema develops [12]. Eichstead, et al. recently identified for the first time likely pathogenic variants in genes related to pulmonary arterial hypertension signaling pathways in HAPE susceptible mountaineers and in a HAPE susceptible family. These variants might be related to HAPE development indicating that HAPE susceptibility might be genetically determined at least in some subjects and could be inherited [41].
History of AMS is the most significant risk factor and best predictor of HEPA [42]. The risk is further increased among persons with a history of high-altitude pulmonary edema (e.g., the risk of recurrence is 60% among persons who ascend to 4,500 m in 2 days) [43]. A prior history of HAPE is a significant predisposing factor rendering an individual HAP susceptible and persons with a prior episode of high-altitude pulmonary edema may have a risk of recurrence as high as 60% if they abruptly ascend to an altitude of 4559 meters [44]. These persons are healthy but have a reduced ventilatory response to hypoxia [45, 46] and an exaggerated pulmonary pressor response to hypoxia and exercise [47, 48]. Although there is no simple method of predicting the risk of recurrence, high- altitude illness will generally recur in susceptible individuals during subsequent exposure to the same altitude at a similar ascent rate. Conversely, persons who tolerate a high altitude without symptoms will usually not experience symptoms on return visits to the same altitude at a similar ascent rate [49, 50]. Honigman B, et al. demonstrated that the strongest predictors for the development of AMS were permanent residence below 3,000 feet (ca. 914 m) and a history of AMS during previous altitude ascent [51].
Conclusion
The cases presented here describe the rapid development of pulmonary edema at moderate altitudes in two healthy patients, who had a rapid and complete response to medical therapy. The diagnosis of typical HAPE is based on medical history, permanence at a consistent altitude, typical symptoms (cough, progressive dyspnea with exertion, decreased exercise tolerance, fever) and signs (chest X-ray and CT Thorax findings, respiratory failure). Factors that increase the incidence of HAPE include a prior history of HAPE, faster rates of ascent, higher altitudes, male sex, cold ambient temperatures, preexisting respiratory infection, and intense exercise. An accurate collection of the patient’s previous clinical history allows the diagnosis to arrive earlier. The disease has a favorable prognosis. It requires simple treatment and a short hospital stay.
Our cases confirm that the predisposing factors for
HAPE contribute to the development of the disease even at moderate altitudes.
References
-
Pennardt A (2013) High-altitude pulmonary edema: diagnosis, prevention, and treatment. Curr Sports Med Rep 12(2): 115-119.
-
Palmer BF (2010) Physiology and pathophysiology with ascent to altitude. Am J Med Sci 340(1): 69-77.
-
Hackett PH, Roach RC (2007) High-Altitude Medicine. In: Auerbach PS (Ed), Wilderness Medicine. 5th(Edn.), Mosby, Philadelphia.
-
Hall DP, Duncan K, Baillie JK (2011). High altitude pulmonary oedema. J R Army Med Corps 157(1): 68-72.
-
Hackett PH, Roach RC (2001) High-altitude medicine. In: Auerbach PS (Ed.), Wilderness Medicine. St. Louis (MO), Mosby.
-
Zhou Q (2011) Standardization of methods for early diagnosis and on-site treatment of high-altitude pulmonary edema. Pulm Med 190648.
-
West JB (2004) The physiologic basis of high-altitude diseases. Ann Intern Med 141(10): 789-800.
-
Luks AM, Swenson ER, Bärtsch P (2017) Acute high- altitude sickness. Eur Respir Rev 26(143): 160096.
-
Maggiorini M (2010) Prevention and treatment of high- altitude pulmonary edema. Progress in Cardiovascular Diseases 52(6): 500-506.
-
Bhagi S, Srivastava S, Shashi BS (2014) High-altitude Pulmonary Edema: Review. J Occup Health 56(4): 235- 243.
-
Hochstrasser J, Nanzer A, Oelz O (1986) Altitude edema in the Swiss Alps. Observations on the incidence and clinical course in 50 patients 1980–1984. Schweiz Med Wochenschr 116(26): 866-873.
-
Maggiorini M (2006) High altitude-induced pulmonary oedema. Cardiovasc Res 72(1): 41-50.
-
Annuario Statistico (2017) Istituto provinciale di Statistica ASTAT, Bolzano.
-
Scherrer U, Rexhaj E, Jayet Allemann PY, Sartori C (2010) New insights in the pathogenesis of high-altitude pulmonary edema. Progress in Cardiovascular Diseases 52(6): 485-492.
-
Stream JO, Grissom CK (2008) Update on high-altitude pulmonary edema: pathogenesis, prevention, and treatment. Wilderness & Environmental Medicine 19(4): 293-303.
-
Maggiorini M, Mélot C, Pierre S (2001) High-altitude pulmonary edema is initially caused by an increase in capillary pressure. Circulation 103(16): 2078-2083.
-
Swenson ER, Bärtsch P (2012) High-Altitude Pulmonary Edema. Compr Physiol 2(4): 2753-2773.
-
Scherrer U, Sartori C, Lepori M (1999) High-altitude pulmonary edema: from exaggerated pulmonary hypertension to a defect in transepithelial sodium transport. Adv Exp Med Biol 474: 93-107.
-
Bärtsch P, Swenson ER (2013) Acute high-altitude illnesses. N Engl J Med 368: 2294-2302.
-
Scherrer U, Vollenweider L, Delabays A, Savcic M, Eichenberger U, et al. (1996) Inhaled nitric oxide for high-altitude pulmonary edema. N Engl J Med 334: 624- 630.
-
Talbot NP, Balanos GM, Robbins PA, Dorrington KL (2008) Can intravenous endothelin-1 be used to enhance hypoxic pulmonary vasoconstriction in healthy humans? Br J Anaesth 101: 466-472.
-
Duplain H, Vollenweider L, Delabays A, Nicod P, Bärtsch P, et al. (1999) Augmented sympathetic activation during short-term hypoxia and high-altitude exposure in subjects susceptible to high altitude pulmonary edema. Circulation 99(13): 1713-1718.
-
Sartori C, Lepori M, Scherrer U (2005) Interaction between nitric oxide and the cholinergic and sympathetic nervous system in cardiovascular control in humans. Pharmacol The 106(2): 209-220.
-
Rimoldi SF, Sartori C, Seiler C, Delacrétaz E, Mattle HP (2010) High-altitude exposure in patients with cardiovascular disease: risk assessment and practical recommendations. Prog Cardiovasc Dis 52(6): 512-524.
-
Gabry AL, Ledoux X, Mozziconacci M, Martin C (2003) High-Altitude Pulmonary Edema at Moderate Altitude (< 2,400 m; 7,870 feet)*A Series of 52 Patients. Chest 123(1): 5-7.
-
Schommer K, Menold E, Subudhi AW, Bärtsch P (2012) Health risk for athletes at moderate altitude and normobaric hypoxia. Br J Sports Med 46: 828-832.
-
Fiorenzano G, Rastelli V, Greco V, Stefano AD, Dottorini M (1994) Unilateral highaltitude pulmonary edema in a subject with right pulmonary artery hypoplasia. Respiration 61(1): 51-54.
-
Levine SJ, White DA, Fels AOS (1988) An abnormal chest radiograph in a patient with recurring high altitude pulmonary edema. Chest 94(3): 627-628.
-
Nakagawa S, Kubo K, Koizumi T, Kobayashi T, Sekiguchi M (19930 High-altitude pulmonary edema with pulmonary thromboembolism. Chest 103(3): 948-950.
-
Derks A, Bosh FH (1993) High altitude pulmonary edema in partial anomalous pulmonary venous connection of drainage with intact atrial septum. Chest 103(3): 973- 974.
-
Torrington KG (1989) Recurrent high altitude illness associated with right pulmonary artery occlusion from granulomatous mediastinitis. Chest 96(6): 1422-1424.
-
Hew Butler T, Rosner MH, Fowkes-Godek S, Dugas JP, Hoffman MD, et al. (2015) Statement of the Third International Exercise-Associated Hyponatremia Consensus Development Conference, Carlsbad, California 2015. Clin J Sport Med 25(4): 303-320.
-
Bennett BL, Hew-Butler T, Hoffman MD, Rogers IR, Rosner MH (2014) Wilderness Medical Society practice guidelines for treatment of hyponatremia: 2014 update. Wilderness Environ Med 25(4): S30-S42.
-
Li SZ, Wang YL, Yan CC (2010) Diagnostic criteria for high altitude pulmonary edema in the early stage. Military Medical Journal of South China 24(3): 161-165.
-
Webb WR (2006) Thin-section CT of the secondary pulmonary lobule: anatomy and the image – the 2004 Fleischner lecture. Radiology 239(2): 322.
-
Liptzin DR, Abman SH, Giesenhagen A, Ivy DD (2018) An Approach to Children with Pulmonary Edema at High Altitude. High Alt Med Biol 19(1): 91-98.
-
Goodman T, Basnyat B (2000) A tragic report of probable high-altitude pulmonary edema in the Himalayas: preventive implications. Wilderness & Environmental Medicine 11(2): 99-101.
-
Oliver SJ, Sanders SJ, Williams CJ, Smith ZA, Lloyd-Davies E, et al. (2012) Physiological and psychological illness symptoms at high altitude and their relationship with acute mountain sickness: a prospective cohort study. J Travel Med 19(4): 210-219.
-
Basnyat B, Murdoch DR (2003) High-altitude illness. Lancet 361(9373): 1967-1974.
-
Durmowicz AG, Noordeweir E, Nicholas R, Reeves JT (1997) Inflammatory processes may predispose children to high-altitude pulmonary edema. J Pediatr 130(5): 838-840.
-
Eichstaedt CA, Mairbäur H, Song J, Benjamin N, Fischer C, et al. (2020) Genetic Predisposition to High-Altitude Pulmonary Edema. High Alt Med Biol 21(1): 28-36.
-
Hackett PH, Roach RC, Schoene RB, Harrison GL, Mills WJ (1988) Abnormal control of ventilation in high-altitude pulmonary edema. J Appl Physiol 64(3): 1268-1272.
-
Bärtsch P, Maggiorini M, Mairbäurl H, Vock P, Swenson E (2002) Pulmonary extravascular fluid accumulation in climbers. Lancet 360(9332): 571-572.
-
Stream JO, Grissom CK (2008) Update on high-altitude pulmonary edema: pathogenesis, prevention, and treatment. Wilderness Environ Med 19(4): 293-303.
-
Bartsch P, Maggiorini M, Ritter M, Noti C, Vock P, et al. (1991) Prevention of high-altitude pulmonary edema by nifedipine. N Engl J Med 325(18): 1284-1289.
-
Hohenhaus E, Paul A, McCullough RE, Kucherer H, Bartsch P (1995) Ventilatory and pulmonary vascular response to hypoxia and susceptibility to high altitude pulmonary oedema. Eur Respir J 8(11): 1825-1833.
-
Grunig E, Mereles D, Hildebrandt W, Swenson ER, Kübler W, et al. (2000) Stress Doppler echocardiography for identification of susceptibility to high altitude pulmonary edema. J Am Coll Cardiol 35(4): 980-987.
-
Kawashima A, Kubo K, Kobayashi T, Sekiguchi M (1989) Hemodynamic responses to acute hypoxia, hypobaria, and exercise in subjects susceptible to high-altitude pulmonary edema. J Appl Physiol 67(5): 1982-1989.
-
Voelkel NF (2002) High-altitude pulmonary edema. N Engl J Med 346(21): 1606-1607.
-
Schneider M, Bernasch D, Weymann J, Holle R, Bartsch P (2002) Acute mountain sickness: influence of susceptibility, preexposure, and ascent rate. Med Sci Sports Exerc 34(12): 1886-1891.
-
Honigman B, Theis MK, Koziol-McLain J, Roach R, Yip R, et al. (1993) Acute Mountain Sickness in a General Tourist Population at Moderate Altitudes. Annals of Internal Medicine 118(8): 587-592.
- Bedside Pulmonary Rehabilitation – Mandatory and Cost- Effective Tools
- The Role of Chest Radiology in Traumatic Injuries: A Comprehensive Narrative Review
- Pseudosepsis in Acute Inflammation of the Lung
- An Overview of Lung Injury in Covid-19: Evaluating the Impact of Re-Exposure and Emerging Variants
- Fibreoptic Bronchoscopy-its Role in Pulmonary Medicine-Current Trends in Intensive Care Unit
- Retrospective Study on the Efficacy of Homoeopathic Medicines in the Treatment of Acute Rhinitis