Improved Exercise Tolerance and Lung Function in Women with LAM Following Three Months of Exercise Training
Rationale: While exercise has been shown to improve respiratory symptoms, exercise tolerance, and bone mineral density in many populations, no supervised exercise training interventions have been undertaken in patients with lymphangioleiomyomatosis (LAM). Objectives: To assess the effects of a supervised exercise intervention on exercise tolerance, pulmonary function, and bone mineral density in patients with LAM. Methods: subjects with LAM (Sporadic LAM n=7; TS-LAM n=1) enrolled in the study. Subjects participated in two weekly supervised aerobic exercise training (50-60 minutes) at 80-85% heart rate max for 12 weeks. Heart rate and oxygen saturation levels were monitored throughout the intervention. Treadmill ergometry (VO2peak), spirometry (FEV1, FVC, FEV1/FVC, FEV1 predicted, peak flow), and bone mineral density assessments were performed prior to and 12 weeks after initiation of intervention. Measurements and Main Results: After 12 weeks of supervised aerobic exercise training, group mean improvements were seen in all outcomes including VO2peak, FEV1, FVC, FEV1/FVC, FEV1 predicted, peak flow, and whole body bone mineral density. Conclusions: Results from this study indicate that supervised exercise training can improve exercise tolerance, pulmonary function, and bone mineral density in patients with lymphangioleiomyomatosis. Further research is needed, including longitudinal studies with larger sample sizes, to determine long-term effects and consistency of these findings. Aerobic exercise may offer a viable alternative to, or work in conjunction with, pharmacological intervention in the treatment of lymphangioleiomyomatosis
Introduction
Lymphangioleiomyomatosis (LAM) is a rare, chronic disease that occurs almost exclusively in women. LAM is characterized by progressive, cystic lung lesions that may lead to respiratory failure and potentially lung transplantation [1, 2]. A decrease in maximal oxygen consumption (VO2max) and/or forced expiratory volume in one second (FEV1) are often seen [1, 3]. Lower VO2max scores indicate poor exercise tolerance and have been linked to disease severity by LAM histologic scores and have been used to predict mortality and time to transplant [4, 5]. A decrease in FEV1 indicates a decline in lung function and can help determine candidacy for lung transplantation, particularly when paired with a decrease in VO2max [2]. While up to 34% of LAM patients present with normal spirometric values patients also frequently present with deficits in other measures of pulmonary function including reduced forced vital capacity (FVC) and the FEV1/FVC ratio. While the majority of focus is understandably centered on lung pathology and pulmonary function, it is noteworthy that seventy percent of women with LAM have shown abnormally low bone mineral density (BMD) values, which are also correlated with disease severity and of course, age [6].
Aerobic exercise has been shown to improve exercise tolerance, pulmonary function, and bone mineral density in many populations, including those with chronic pulmonary disorders [7, 8, 9]. To our knowledge no long-term supervised exercise training interventions have been conducted in patients with LAM to determine the benefits for this patient population. Our lab is conducting a year-long supervised exercise training intervention in women with LAM to assess the impact of such an intervention on exercise tolerance, pulmonary function, and bone mineral density. Here we report on our first eight patients on the progress that has been made after three months of training.
Methods
Study Population
Eight participants were recruited from the University of Texas Health Science LAM Clinic (Dr. Khalid Almoosa, Director). Human subjects’ approval was granted by both The University of Houston and University of Texas Health Science Center. All patients gave informed consent before enrollment. All patients were women aged 27-59 (mean ± SD, 41.5 ± 11.9 years). Diagnosis of LAM was confirmed by CT scan with concurrent clinical presentation, or by lung biopsy. Patients had either sporadic (n=7) or TS-associated (n=1) LAM. Two patients were taking LAM-related medication (everolimus, sirolimus, and/or Affinitor) for three years and four years at the time of enrollment (beginning of study). None of the patients required oxygen for daily use or during exercise.
Tests and Measures
Patients performed a graded exercise test to volitional fatigue to determine VO2peak using a Woodway Desmo treadmill (Waukesha, WI, USA) and a Quark CPET metabolic cart (Cosmed, Rome, Italy). Briefly, patients ran or walked at a pace that was difficult but manageable (generally 3.5mph for those walking, 4.2-5.2mph for those who ran). While the pace (speed) remained the same throughout the test, the grade (elevation) of the treadmill was increased (0% for minute one, 4% for minute two, 6% for minute three, 8% for minute four, etc.). Patients reported their rate of perceived exertion (RPE) using Borg’s RPE scale [10]. Every minute heart rate and RPE was recorded and patients were asked as to whether or not they could continue to the next level. Patients ran or walked until volitional fatigue. Final (end of test) heart rates and RPE scores were recorded. All patients achieved or nearly-achieved their age-predicted maximum heart rate (220-age) during or near the end of their treadmill test [11].
Pulmonary functions tests (FEV1, FVC, FEV1/FVC ratio, FEV1 predicted, and peak flow) were assessed using the Quark CPET metabolic cart (Cosmed, Rome, Italy). A Discovery QDR-4500 for Windows (Hologic, Inc., Bedford, MA, USA) dual x-ray absorptiometry (DXA) scanner was used to assess whole body bone mineral density. All tests and measures were taken at baseline (prior to exercise training) and again after three months of intervention. All tests were completed on room air without the use of a bronchodilator.
Intervention
Patients reported twice per week for supervised aerobic exercise sessions lasting 50 to 60 minutes in duration. Exercise was performed at 80-85% heart rate max (HRmax) as determined by baseline graded exercise test using a Polar FT1 fitness monitor with the T31 transmitter (Lake Success, NY, USA). Oxygen saturation levels were maintained at ≥88% as per the Choicemed OxyWatch C20SM Pulse Oximeter (Bristol, PA, USA). Treadmill training (walking, jogging, sprints), aerobic exercise circuits (plyometrics, stadium stair running, various bodyweight drills), and strength training circuits (resistance training with free weights, bodyweight exercises) were all utilized during training with emphasis on using body weight resistance and minimal specialized equipment.
Statistics
Dependent t-tests were performed for group results in each category. Significance levels were set at p ≤ 0.05. Simple percentages were used to calculate both group mean and individual change. All data were analyzed using SPSS software version 17. Unless otherwise noted, results are reported as mean ± standard deviation (SD).
Results
After twelve weeks of supervised aerobic exercise training, patients experienced a group mean percent increase in all outcome measures. Exercise tolerance (VO2peak) improved by 13.3% (29.89 ± 9.9 mL/kg/min pre, 33.88 ± 9.53 mL/kg/min post; p=0.06; Figure 1a). Pulmonary function tests also improved, with FEV1 (2643.75 ± 814.9 mL pre, 2747.88 ± 886.13 mL post; p=0.19; Figure 1b), FVC (3560 ± 1266.36 mL pre, 3803.75 ± 1177.61 mL post; p=0.085;
Figure 1c), FEV1/FVC% (76.65 ± 8.26 pre, 77.41 ± 9.76 post; p=0.38; Figure 1d), FEV1 predicted (92.38 ± 29.97 % pre, 102.63 ± 26.4% post; p=0.11; Figure 1e), and peak flow (5.53 ± 2.02 L/sec pre, 6.20 ± 1.23 L/sec post; p=0.19; Figure 1f) all showing improvements. Whole body BMD improved slightly (1.16 g/cm2 pre, 1.178 ± 0.12 g/cm2 post; p=0.28; Figure 1g). Though we had a limited sample size of only eight patients and no group mean results were found to be significant at the p=0.05 level, patients improved in all areas.
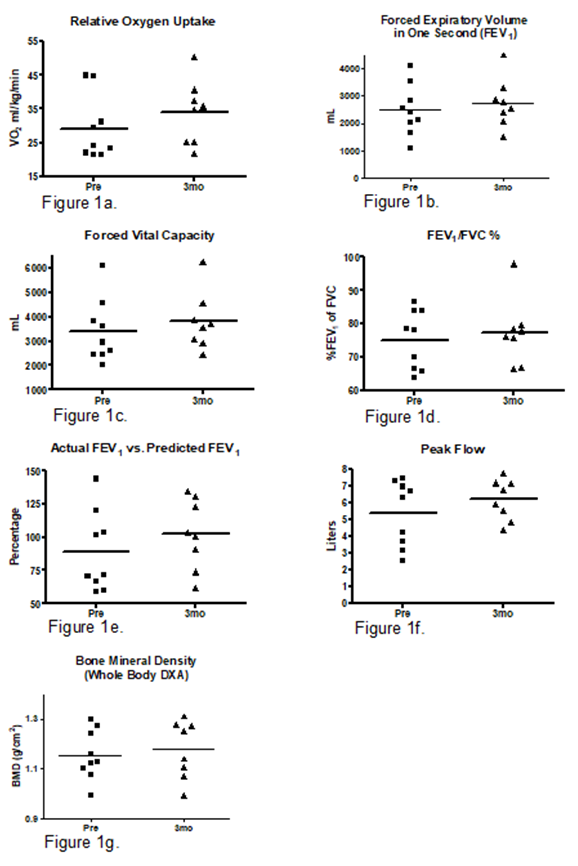
Figure1: Oxygen uptake, pulmonary function, and bone mineral density.
Discussion
In this study we demonstrate that supervised aerobic exercise training can markedly improve exercise tolerance and pulmonary function that are commonly exhibited in women with LAM. We also found a slight increase in bone mineral density (BMD), important as BMD has been shown to be affected to a greater extent in women with LAM when compared to otherwise healthy females [6]. We found that many of our patients achieved their highest VO2 levels prior to their last stage of the exercise test. This may have been due to air trapping, reduced diffusion capacity, a greater oxygen desaturation, or a combination of events that led to this ventilator limitation, as these have all been shown to be common in women with LAM during exercise [3]. The VO2 values reported here reflect maximal oxygen uptake values obtained during each single test but do not necessarily indicate the maximum value attainable by each participant. Accordingly, VO2peak was used as opposed to VO2max as VO2peak value has been shown to likely be a valid indicator of VO2max, even without the traditional VO2 plateau [12].
Patients showed the largest improvement in relative VO2 (mL/kg/min) with an improvement of 13.3% from baseline (29.89 ± 9.9 pre, 33.88 ± 9.53 post; p=0.06). This is not surprising, as all of our patients were not actively participating in regular exercise and their work capacity increased markedly over a very short period of time. With an initial intervention period of twelve weeks, this number corresponds to a mean increase of 4.43% per month. As an increased VO2 is indicative of an increase in function, this may translate into an improved quality of life in daily function. Though we did not assess any psychological variables, our patients reported having more energy and of “feeling better” throughout the day as well as at night. Four of our patients had undergone (prior to beginning exercise training) surgical interventions (pleurectomy, pleurodesis, removal of a kidney due to angiomyolipomas). None of our patients experienced any reportable events during their training or subsequent to the three month time point. FEV1 improved on average by 104mL over the twelve-week intervention (a 4% improvement, average of 1.33mL/month). Though small, this increase in FEV1 is 33% greater than the 1 mL/ month FEV1 increase seen in the intervention group of the Multicenter International LAM Efficacy of Sirolimus (MILES) Trial, and far exceeds the 12mL (± 2mL) decline of the control group from the same study [11]. Moreover, the 81.7mL per month increase in FVC seen in our study is a ten- fold improvement compared with the 8mL average monthly increases seen in the MILES Trial intervention group and a huge increase compared with the 11mL (±3 ) decrease seen in the control group [13]. Predicted FEV1 (%) improved by 11.1%, from 92.38 ± 29.97 to 102.63 ± 26.4, a level slightly above predicted. Peak flow improved markedly (12.3%), though not statistically significant (p=0.19), from 5.53 ± 2.02L/min to 6.2 ± 1.23L/min.
Bone mineral density (BMD) improved slightly. Patients’ overall BMD improved by 1.6%, from 1.159 ± 0.11 to 1.178 ± 0.12 g/cm2. While not a statistically significant improvement (p=0.13) this nonetheless shows promise. Women with LAM have been shown to have an accelerated bone loss (6); coupled with the normal loss of bone due to aging and osteoporosis, which affect all women irrespective of lung disease, exercise training may serve as a means of improving bone health in women with LAM. None of our patients was taking any prescribed medication for bone loss.
It must be noted that all of our patients were, aside from their disease, in relatively good health and were able to perform exercise training. At the onset of exercise training, none of our patients were able to run for more than five consecutive minutes (at a pace of 4.5-4.7mph) without stopping due to self-reported pulmonary fatigue. Three patients were not able to run for any length of time at the beginning of the study. At the end of three months all patients were able to run at a pace of at least 4.0mph. Six patients, including our oldest (59 years at the beginning of the study) have subsequently been able to run for more than two miles non-stop, with several completing up to four miles of treadmill running, a remarkable improvement in a very short time. These findings show definite promise for the use of supervised aerobic exercise as an effective treatment in women with LAM. While we do not know the effects of our intervention on lung pathology (i.e. cystic changes), our ongoing study hopes to determine if changes in the biology of the lung are evident.
Our patients varied in age from 27 to 59 years of age, with the mean age being 41.5 years, the approximate mean age at which LAM is clinically diagnosed. As is the case with many women with LAM, our patients exhibited clinical signs (pneumothoraces, angiomyolipomas, obstructed breathing) before diagnosis, in several cases years before a clinical diagnosis. With many cases of LAM being diagnosed earlier in the disease process, this finding could have important significance to optimize intervention, especially in those recently diagnosed.
Limitations of this study include the small sample size (n=8); this was an underpowered study in terms of sample size but we do not feel that this diminishes the positive impact that our intervention had on our patients. Because of this small sample size, the results of this study may have limited generalizability to the LAM population at large. However, as patients’ overall lung function improved and our patients were quite homogenous, with patients of differing ages and with a wide variety of symptoms, we believe that this study justifies a study with a larger patient cohort.
This is the first known study reporting effects of supervised exercise training on patients with LAM. The results from this study demonstrate that supervised exercise training can improve exercise tolerance, pulmonary function, and bone mineral density in patients with lymphangioleiomyomatosis in a relatively short time. Aerobic exercise may offer a viable alternative or addition to pharmacological intervention in the treatment of lymphangioleiomyomatosis.
At a Glance Commentary
Exercise has been shown to improve pulmonary function and quality of life in a variety of patient populations. An increase in pulmonary function and, in particular, exercise tolerance, can markedly improve daily living activities. To date, the benefits of a supervised exercise training program have not been studied in women with lymphangioleiomyomatosis (LAM), a devastating lung disease that has no cure and limited treatment options. Here we demonstrate that exercise training not only improves oxygen consumption (VO2) but also pulmonary function measures that are used to predict disease progression. This is the first study to show that exercise training can be used as a potential treatment for women with LAM.
References
-
Ryu JH, Moss J, Beck GJ, Lee JC, Brown KK, et al. (2006) The NHLBI lymphangioleiomyomatosis registry: characteristics of 230 patients at enrollment. Am J Respir Crit Care Med 173(1): 105-111.
-
Johnson SR, Cordier JF, Lazor R, Cottin V, Costabel U, et al. (2010) European Respiratory Society guidelines for the diagnosis and management of lymphangioleiomyomatosis. Eur Respir J 35(1): 14-26.
-
Baldi BG, Albuquerque AL, Pimenta SP, Salge JM, Kairalla RA, et al. (2012) Exercise performance and dynamic hyperinflation in lymphangioleiomyomatosis. Am J Respir Crit Care Med 186(4): 341-348.
-
Taveira DaSilva AM, Stylianou MP, Hedin CJ, Kristof AS, Avila NA, et al. (2003) Maximal oxygen uptake and severity of disease in lymphangioleiomyomatosis. Am J Respir Crit Care Med 168(12): 1427-1431.
-
Matsui K, Beasley MB, Nelson WK, Barnes PM, Bechtle J, et al. (2001) Prognostic significance of pulmonary lymphangioleiomyomatosis histologic score. Am J Surg Pathol 25(4): 479-484.
-
Taveira-Dasilva AM, Stylianou MP, Hedin CJ, Hathaway O, Moss J (2005) Bone mineral density in lymphangioleiomyomatosis. Am J Respir Crit Care Med 171(1): 61-67.
-
Aloia JF, Cohn SH, Ostuni JA, Cane R, Ellis K (1978) Prevention of involutional bone loss by exercise. Ann Intern Med 89(3): 356-358.
-
Serres I, Varray A, Vallet G, Micallef JP, Prefaut C (1997) Improved skeletal muscle performance after individualized exercise training in patients with chronic obstructive pulmonary disease. J Cardiopulm Rehabil 17(4): 232-238.
-
Blau H, Mussaffi-Georgy H, Fink G, Kaye C, Szeinberg A, et al. (2002) Effects of an intensive 4-week summer camp on cystic fibrosis: pulmonary function, exercise tolerance, and nutrition. Chest 121(4): 1117-1122.
-
Noble BJ, Borg GA, Jacobs I, Ceci R, Kaiser P (1983) A category-ratio perceived exertion scale: relationship to blood and muscle lactates and heart rate. Med Sci Sports Exerc 15(6): 523-528.
-
Karvonen J, Vuorimaa T (1988) Heart rate and exercise intensity during sports activities. Practical application. Sports Med 5(5): 303-311.
-
Day JR, Rossiter HB, Coats EM, Skasick A, Whipp BJ (2003) The maximally attainable VO2 during exercise in humans: the peak vs. maximum issue. J Appl Physiol 95(5): 1901-1907.
-
McCormack FX, Inoue Y, Moss J, Singer LG, Strange C, et al. (2011) Efficacy and safety of sirolimus in lymphangioleiomyomatosis. N Engl J Med 364(17): 1595-1606.
- Bedside Pulmonary Rehabilitation – Mandatory and Cost- Effective Tools
- The Role of Chest Radiology in Traumatic Injuries: A Comprehensive Narrative Review
- Pseudosepsis in Acute Inflammation of the Lung
- An Overview of Lung Injury in Covid-19: Evaluating the Impact of Re-Exposure and Emerging Variants
- Fibreoptic Bronchoscopy-its Role in Pulmonary Medicine-Current Trends in Intensive Care Unit
- Retrospective Study on the Efficacy of Homoeopathic Medicines in the Treatment of Acute Rhinitis