Monoplanar Acces for Percutaneous Nephrolithotomy
Percutaneous Nephrolithotomy has undergone considerable evolution since its introduction in the 1970s, which has been driven by advances in access techniques, instrumentation and endoscopic technology. Renal access can be achieved by ultrasonography, fluoroscopy and computed tomography guidance. Access under fluoroscopy control can be performed under monoplanar or biplanar guidance. The biplanar access can be achieved by “triangulation†or “eye of the needle†(bull s eye) techniques. The monoplanar access is safe; decreases puncture and radiation time and has similar success rates as the biplanar access.
Introduction
Percutaneous Nephrolithotomy (PCNL) is the first-line treatment modality for the management of kidney stones larger than 2 cm in diameter [1, 2]. The creation of a percutaneous renal access is the most important step in PCNL and the adequacy of the access directly influences the success and complication rates of this procedure. Several techniques have been used for guidance for entrance to the collecting system, including fluoroscopy, computed tomography (CT), and ultrasonography (US), however access under fluoroscopy is the most commonly used [3, 4, 5, 6, 7, 8, 9, 10, 11, 12]. The aim of this mini review is to emphasize the importance of the renal access, mainly the monoplanar technique, during PCNL.
Access under fluoroscopy guidance
The access under fluoroscopy control can be performed either under biplanar or monoplanar guidance. Biplanar access (triangulation, eye of the needle "bull's eye"): Biplanar access is based on the cephalad- caudad and mediolateral movements of the needle; the depth of the needle is adjusted with using fluoroscopic imaging in 30 degree and vertical positions (Figure 1). Both techniques need a target, most commonly generated by opacification of the collecting system with iodinated contrast that is administered retrograde via a cystoscopically placed ureteral catheter. A caliceal entry point is selected to avoid the larger vascular structures that are found at the level of the infundibulum.

Bull’s-eye technique of caliceal targeting: The patient is positioned prone, on radiolucent chest rolls, with pressure points assessed and added. The ipsilateral flank is widely prepped and draped to maximize exposure for selecting an appropriate calix for access. The collecting system is opacified with diluted iodinated contrast, and a C-arm is used to monitor this fluoroscopically (Figure 2 & 3). The C-arm image is rotated 90 degrees from the standard (upright) projection. For right-sided renal access, the image is rotated clockwise, and for left-sided access, the image is rotated counterclockwise. This aligns the image with the patient’s position relative to the surgeon, and the surgeon’s maneuvers are accurately reflected fluoroscopically. The C-arm is then rotated 30 degrees toward the surgeon, along the axis of the posterior row of calices and the relatively vascular line of Brödel. A posterior calix may then be identified fluoroscopically, and the skin overlying this point is marked and incised. A 15-cm, 18-gauge two-part trocar needle is used to access the collecting system. It is preferable to mount the needle on a radiolucent platz needle holder, which serves to steady the needle while keeping the surgeon’s hands further removed from the radiation field. When the long axis of the needle is positioned over the targetedcalix at an angle of 30 degrees, the alignment of the needle, its hub, and the calix gives the characteristic bull’s-eye appearance. If a longitudinal segment of the needle shaft is visible fluoroscopically, the axis of entry is not at 30degrees and is thus adjusted as needed. Maintaining the bull’s-eye appearance, the needle is then advanced. The C-arm is rotated back to the AP projection to monitor the medial progression or ‘‘depth’’ of the puncture until the needle tip is seen to enter the calix.
Figure 2a: fluoroscopic image before rotating.
Figure 2b: fluoroscopic image after rotating.
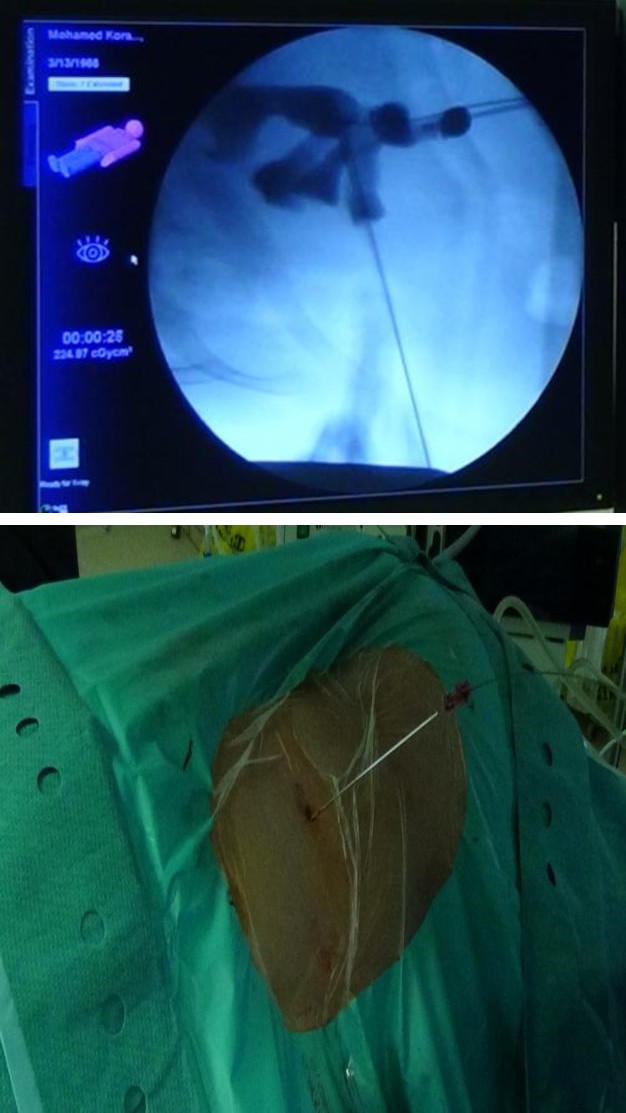
Figure 3a: fluoroscopic image showing the puncture through the base of the lower calyx.
Figure 3b: The needle and the guide wire through the skin.
Triangulation technique of caliceal targeting
The triangulation technique is based on simple geometric principles and is guided with biplanar fluoroscopy; one plane is AP to the line of puncture and the other is oblique. The AP view maybe considered to be in a plane parallel to the axis of puncture and is used to monitor medial-lateral (left-right) adjustments. The oblique view gives information regarding depth to the site of puncture and is used to monitor needle adjustments in the cephalad-caudad (up-down) orientation. The tip of the needle is oriented to the calix of puncture in both the AP and oblique planes. Left-right adjustments are limited to the AP view only, and cephalad-caudad adjustments are limited to the oblique view. When making adjustments in the mediolateral axis, care should be taken not to inadvertently move the needle in the cephalad-caudad axis; conversely, when making adjustments in the cephalad-caudad axis, care should be taken so as not to in advertently move the needle in the mediolateral axis. Once the needle is aligned with the targeted calix in both the mediolateral and cephalad-caudad orientations, it is advanced with radiographic guidance (continuous fluoroscopy). The needle should always be advanced in the oblique view, which will allow for the assessment of the depth of the needle’s penetration [9, 10].
Monoplanar access
Monoplanar access is based on the intensive movement of the kidney and the retraction of the targeted calyx under fluoroscopy on a vertical plane only. Patients are initially placed in lithotomy position under general anesthesia, and then a ureteral catheter is inserted. Percutaneous access is performed with the aid of C-arm fluoroscopy with the patients in prone position (Figure 4). The C-arm fluoroscope is brought into vertical position. The collecting system is visualized with the aid of a contrast agent injected through an ureteral catheter, and the most appropriate calyx is selected to extract the targeted stone. The needle is horizontally positioned on the skin surface, particularly toward the entry site on the same planeas that of the targeted calyxes. The needle is directed toward the desired calyx. Acurved renal appearance is observed during access into the kidney. If intervention fails, the needle do not draw back completely from the skin, only it is retracted approximately 1 cm intra corporeally, and its angle of entry is adjusted on the same vertical plane and reinserted [8].

Discussion
The Percutaneous renal access is performed by urologists or radiologists in different countries [13, 14, 15, 16]. Watterson and colleagues retrospectively compared accesses obtained by urologists versus those obtained by radiologists and concluded that urologist-acquired percutaneous access resulted in fewer access-related complications and improvements in stone-free rates [15]. Tomaszewski et al reported significantly higher stone- free rates in patients whose access was performed by urologists, but complication rates were reported similar between urologists and radiologists [14]. El-Assmy and his coworkers reported no significant differences between urologists and radiologists in terms of success and complication rates [16]. Although there is some controversy regarding the success and complications associated with percutaneous access obtained by urologists and radiologists, results indicate that urologists should direct the access for effective subsequent percutaneous procedures. US, CT and fluoroscopy guidance have all been described for percutaneous access, with the latter being the most commonly used in both prone and supine position [4, 5, 10, 17, 18, 19] (Figure 5).

Renal access has a direct effect on the success rate of the operation and on the occurrence of the complications. The success of the surgery is highly dependent on the understanding of renal anatomy to establish a safe transpapillar access to the collecting system and to avoid bleeding or injury of the adjacent organs [20]. Triangulation and eye of the needle techniques are two primary methods to achieve proper percutaneous renal access under biplanar fluoroscopic guidance [9]. Various other alternative access techniques are described in the literature. These include an access method that uses a locator by Lazarus et al., modified access technique by Li et al., all-seeing needle method by Bader et al. and blind puncture technique by Basiri et al. All of these methods have been used safely and efficiently [21, 22, 23, 24]. Mues et al. used fluoroscopic projections directed at an angle of 30o to the head of the patient for lower pole entries, and at 20o toward the opposite side of the surgeon for middle and upper pole entries [20]. Hatipoglu et al. in their study they identified the appropriate calyx, then they inserted and advanced the needle forward from a suitable skin entry site at an angle of nearly 30°, but parallel to the infundibulum to observe calyceal retraction and movements of the kidney [8].
Analysis of puncture times was conducted in various studies as a first step in renal access procedures. Li et al. compared a modified puncture technique and standard PCNL, and the puncture times they obtained were 7 and 17 min, respectively. A separate study compared learning curves and found that the puncture times ranged from 1 to 12 min even after 60 cases of PCNL [21, 23]. Hatipoglu et al. had a shorter puncture time than other authors, their average puncture time been 0.83 min (8 s to 5 min) [8]. Operation and fluoroscopy screening times vary according to factors such as number of accesses, stone burden, experience of the surgeon, and dilation method [25]. Radiation exposure is a major limitation of the access techniques performed under fluoroscopic guidance. This is especially true in biplanar accesses, where fluoroscopic projections are directed from both the vertical plane and at an angle of 30° to the horizontal plane. When images are taken from an angle of 30°, the surgeon is directly exposed to high doses of radiation, particularly to the upper part of the his/her body. Studies comparing anteroposterior or posteroanterior projections with lateral fluoroscopic projections indicate that the latter exposes the patient, the surgeon and the operating room staff to 3-7 times higher radiation doses than do the other techniques [11, 12]. Dede et al. [7] in their study found that the average fluoroscopy screening time and puncture times were comparatively shorter than those when they used the biplanar technique. They found significantly less operative time, less hematocrit drop and less auxiliary procedure in the monplanaraccess than in the biplanar one. Regarding other parameters like hospital stay, stone free rate and complications there was no significance difference between the two groups [7].
Conclusion
The monoplanar access technique is a safe method, it decreases puncture and radiation time, it minimizes the patient's, the surgeon's and stuff's direct exposure time to radiation and it has similar success rates as the biplanar access technique
References
-
Türk C, Knoll T, Petrik A, A Skolarikos, M Straub, et al. (2015) EAU guidelines on urolithiasis.
-
de la Rosette J, Assimos D, Desai M, Gutierrez J, Lingeman J, et al. (2011) The clinical research office of the endourological society percutaneous Nephrolithotomy global study: indications, complications, and outcomes in 5803 patients. J Endourol 25(1): 11-17.
-
Yang RM, Morgan T, Bellman GC (2002) Radiation protection during percutaneous Nephrolithotomy: A new urologic surgery radiation shield. J Endourol 16(10): 727-731.
-
Matlaga BR, Shah OD, Zagoria RJ, Dyer RB, Streem SB, et al. (2003) Computerized tomography guided access for percutaneous nephrostolithotomy. J Urol 170(1): 45-47.
-
Hosseini MM, Hassanpour A, Farzan R, Yousefi A, Afrasiabi MA, et al. (2009) Ultrasonography-guided percutaneous nephrolithotomy. J Endourol 23(4): 603-607.
-
Tepeler A, Armagan A, Akman T, Polat EC, Ersöz C, et al. (2012) Impact of Percutaneous Renal Access Technique on Outcomes of Percutaneous Nephrolithotomy. J Endourology 26(7): 828-833.
-
Dede O, Bas O, Sancaktutar A, Daggulli M, Utangac M, et al. (2015) Comparison of Monoplanar and Biplanar Access Techniques for Percutaneous Nephrolithotomy. J Endourology 29(9): 993-997.
-
Hatipoglu N, Bodakci M, Penbegu N, Bozkurt Y, Sancaktutar AA, et al. (2013) Monoplanar access technique for percutaneous nephrolithotomy. Urolithiasis 41(3): 257-263.
-
Miller NL, Matlaga BR, Lingeman JE (2007) Techniques for fluoroscopic percutaneous renal access. J Urol 178(1): 15-23.
-
Steinberg PL, Semins MJ, Wason SE, Davis JG, Smith BL, et al. (2009) Fluoroscopy guided percutaneous renal access. J Endourol 23(10): 1627-1631.
-
Miller ME, Davis ML, MacClean CR, Davis JG, Smith BL, et al. (1983) Radiation exposure and associated risks to operating-room personnel during use of fluoroscopic guidance for selected orthopaedic surgical procedures. J Bone Joint Surg Am 65(1): 1-4
-
Theocharopoulos N, Perisinakis K, Damilakis J, Papadokostakis G, Hadjipavlou A, et al. (2003) Occupational exposure from common fluoroscopic projections used in orthopaedic surgery. J Bone Joint Surg Am 85-A (9): 1698-1703.
-
Lashley DB, Fuchs EF (1998) Urologist-acquired renal access for percutaneous renal surgery. Urology 51(6): 927-931.
-
Tomaszewski JJ, Ortiz TD, Gayed BA, Smaldone MC, Jackman SV, et al. (2010) Renal access by urologist or radiologist during percutaneous nephrolithotomy. J Endourol 24(11): 1733-1737.
-
Watterson JD, Soon S, Jana K (2006) Access related complications during percutaneous nephrolithotomy: Urology versus radiology at a single academic institution. J Urol 176(1): 142-145.
-
El-AssmyAM, ShokeirAA, MohsenT, El-Tabey N, El- Nahas AR, et al. (2007) Renal access by urologist or radiologist for percutaneous nephrolithotomy- is it still an issue? J Urol 178(3 pt 1): 916-920.
-
Hoznek A, Ouzald I, Gettman M, Rode J, De La Taille A, et al. (2001) Fluorscopy-guided Renal Access in Supine Percutaneous Nephrolithotomy. Urology 78(1): 221-224.
-
Osman M, Wendt-Nordahl G, Heger K, Michel MS, Alken P, et al. (2005) Percutaneous nephrolithotomy with ultrasonography-guided renal access: experience from over 300 cases. BJU Int 96(6): 875-878.
-
Penbegul N, Tepeler A, Sancaktutar AA, Bozkurt Y, Atar M, et al. (2012) Safety and efficacy of ultrasound-guided percutaneous nephrolithotomy for treatment of urinary stone disease in children. Urology 79(5): 1015-1019.
-
Mues E, Gutierrez J, Loske AM (2007) Percutaneous renal access: a simplified approach. J Endourol 21(11): 1271-1275.
-
Lazarus J, Williams J (2012) The Locator: novel percutaneous nephrolithotomy apparatus to aid collecting system puncture-a preliminary report. J Endourol 25(5): 747-750.
-
Basiri A, Mehrabi S, Kianian H, Javaherforooshzadeh A (2007) Blind puncture in comparison with fluoroscopic guidance in percutaneous nephrolithotomy: a randomized controlled trial. Urol J 4(2): 79-83.
-
Li X, Liao S, Yu Y, Dai Q, Song B, et al. (2012) Stereotactic localisation system: a modified puncture technique for percutaneous nephrolithotomy. Urol Res 40(4): 395-401.
-
Bader MJ, Gratzke C, Seitz M, Sharma R, Stief CG, et al. (2011) The ‘‘all-seeing needle’’: initial results of an optical puncture system confirming access in percutaneous nephrolithotomy. Eur Urol 59(6): 1054-1059.
-
Negrete-Pulido O, Molina-Torres M, Castano-Tostado E, Loske AM, Gutiérrez-Aceves J, et al. (2010) Percutaneous renal access: the learning curve of a simplified approach. J Endourol 24(3): 457-460.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report