Retrospective Analysis of Recipients after Kidney Transplantation from a Family Donor in the Lviv Regional Clinical Hospital
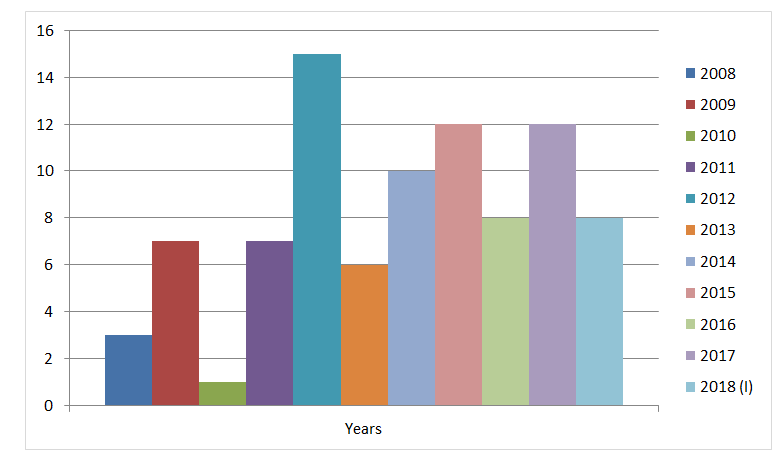
Introduction: Contemporary transplantology still faces many challanges, in particular due to the lack of living and inanimate donors, compared with the number of recipients; immaturity of immunodiagnostic and other diagnostic tools for the early prevention of acute rejection of graft; toxic effects and other imperfections of immunosuppressants. The Purpose: Of the work is to assess retrospectively аnalysis of recipients after kidney transplantation a family donor in the Lviv Regional Clinical Hospital. Materials and Methods: 89 medical histories of recipients undergoing in-patient treatment in the center of the kidney transplantation and chronic hemodialysis and the department of vascular surgery during the years 2008-2018 (Diagram 1) were analyzed retrospectively. 86 patients undergone one transplantation, 3 more than one. 47 (52.8%) were men and 42 (47. 2%) women. The age of the recipients ranged from 17 to 60 years. The median age of patients was 28.9 ± 1.2 years. Results: HLA-typing was performed in 38 (42.7%) pair of recipients and donors. There were 3 classical loci in 7 (18.9%) patients, 4in 15 (39.5%) recipients, and 5 in 16 (43.3%) patients. HLA matching by degree of match to 36 pairs. The crossmatch donor-recipient reaction was as follows: the absence of dead lymphocytes was observed in the 4donor-recipientpairs; 2 pairs had a dead lymphocyte count of 5%, 9pairs- 10%, 28 pairs - 15%, 45 pairs - 20% and 1 pair- 35%. Cross-matching is typically presented as negative is the 6 donor-recipient pair; indeterminate 37 pairs and positive 46 pairs.
Tolstyak Ya F*, Chopyak VV and Yakovlev IG
Clinical Immunology and Allergology Department, Lviv National Medical University named after Danylo Halytsky, Lviv Regional Hospital, Ukraine *Corresponding author: Tolstyak Ya F, Assistant professor of clinical immunology and Allergology Lviv National Medical University named after Danylo Halytsky, Lviv Regional Hospital, Ukraine, Tel: +38067902928; Email: tolstyakyaroslav@gmail.com
Introduction
The dynamic development of transplant ology in the world over the past decades has given a chance to prolong the lives of many patients. Contemporary transplant ology still faces many challenges, in particular due to the lack of living and inanimate donors, compared with the number of recipients; immaturity of immunodiagnostic and other diagnostic tools for the early prevention of acute rejection of graft; toxic effects and other imperfections of immunosuppressant’s. Other problems can be illustrated by the kidney transplant example, when 90-95% of kidney transplants function one year after transplantation, and 10 years just every second kidney from a living donor and every third from a dead donor [1, 2, 3, 4, 5].
Until 2019, Ukraine ranked last in Europe for organ transplantation. The number of organ transplants did not exceed 120 per year, only from family donors with posthumous transplantation accounting for 15%, and was carried out only abroad. Since 2019, on the basis of a new law of Ukraine, posthumous donation has been allowed in Ukraine. For example, already in 2022, despite the full-scale invasion of the Russian Federation, 384 organ transplants per year were performed, 55% of them from a deceased donor [2, 3, 4, 5, 6]. The importance of kidney transplantation is that it remains the only lifeline for many patients with end- stage chronic kidney disease and provides these recipients with a relatively normal lifestyle [3, 6].
The purpose
Of the work is to assess retrospectively analysis of recipients after kidney transplantation a family donor in the Lviv Regional Clinical Hospital.
Materials and Methods
In the case of family transplantation only parents, mothers, brothers and sisters, husband or wife and children can be donors. 89 medical histories of recipients undergoing in-patient treatment in the center of the kidney transplantation and chronic hemodialysis and the department of vascular surgery during the years 2008-2018 Figure 1 were analyzed retrospectively. 86 patients have undergone one transplantation, 3 more than one. 47 (52.8%) were men and 42 (47. 2%) women. The age of the recipients ranged from 17 to 60 years. The median age of patients was 28.9 ± 1.2 years.
Due to the high polymorphism in the HLA system and since some of the HLA antigens appear to be more immunogenic, this study was designed to detect the most common distribution of HLA alleles in Ukranian kidney transplant donors and recipients. The understanding of HLA subtype frequency has also permitted a better A, B, DR matching of donor and recipient and better clinical results. HLA-class I and II alleles typing by lymphocytotoxic test. In this retrospective analysis, history of renal dysfunction, and other participants data were obtained from personal historical disease. The study used a large cross-match according to the method complement dependent cytotoxicity [7, 8]. Viral infections were determined by the immune enzyme method and polymerase chain reaction.
All recipients with kidney transplant from a relative had a chronic kidney disease of V stage. Etiology is shown in Figure 2 chronic glomerulonephritis 65 (73.0%) patients, malformations of the urinary system - 10 (8.9%) patients, systemic disease of the connective tissue - 5 (5.6%) patients (systemic lupus erythematosus - 2, systemic scleroderma - 1, Sharpe disease - 1 and rheumatoid arthritis – 1), type 1 diabetes - 5 (5.6%) patients and chronic pyelonephritis - 4 (4.5%) patients.
Among 89 patients 71 (79.7%) were on chronic hemodialysis, 9 (10.1%) on peritoneal dialysis, and 9 (10.1%) without hemodialysis. I disability group had 59 (66.3%) patients, II group - 9 (10.1%) patients, no disability before transplantation - 21 (23.6%) patients.
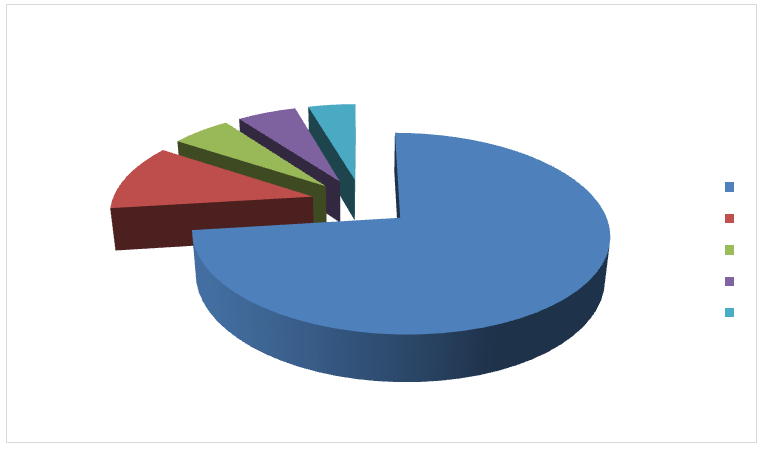
In accordance with the Law of Ukraine No. 1007-XIV dated 16.07.1999 “On Transplantation of Organs and Other Human Anatomical Materials”, only relatives can be donors in Ukraine. During 2008-2018 (1) years in the Center of organs and other anatomical materials transplantation of Lviv regional hospital: mother - 46 (51.7%) donors, father - 30 (33.7%), brother - 4 (4,5%), sister - 4 (4.5%), grandfather, aunt, uncle, husband, wife – 1 (1.1%) donor.
Results and Discussion
Due to the socio-economical situation in Ukraine these recipients received insufficient number of immunological examinations when selecting a couple recipient donor. Blood group and Rh factor were determined in all pairs:I (0) - 22 (24.7%) patients, II (A) - 43 (48.3%) patients, III (B) - 17 (19.1%)patients, IV (AB) - 7 (7.8%) patients In 79 (88.7%) pairs the blood groups were identical and in 10 (11.2%) we’re not:3 recipients with the III (B) group and 6 recipients with the II (B) group had donors with I (0) group and 1 recipient with IV (AB) group had a donor with II (A) group. Rhesus was positive in 82 (92.2%) recipients.
HLA-typing was performed in 38 (42.7%) pairs, due to the fact that during 2012-2016 years reagents were not covered by the state. There were 3 classical loci in 7 (18.9%) patients, 4in 15 (39.5%) patients, and 5 in 16 (43.3%) patients. HLA matching by degree of matched to 36 pairs.
The cross-match donor-recipient reaction was as follows: the absence of dead lymphocytes was observed in the 4 donor-recipient pairs; 2 pairs had a dead lymphocyte count of 5%, 9 pairs - 10%, 28 pairs - 15%, 46 pairs - 20%. In general, the cross-match was unfocused in 6 (6, 7%) patients, and positive in 83 (93,3%) patients. Cross-matching is typically presented as negative is the 6 donor-recipient pair; indeterminate 37 pairs and positive 46 pairs.
All donors and recipients under the protocol [9] were screened for various latent and chronic infections. Antibodies to HIV infection, syphilis, tuberculosis were absent in all patients. IgG antibodies to cytomegalovirus were present in 95.0% pairs, IgG antibodies to herpes virus type 1 and 2 - in 99.0% and to toxoplasma in 70.5% pair. IgM antibodies to cytomegalovirus were present in 2 (2.2%) recipients and to herpes virus type 1 in 1 (1.1%) recipient. Polymerase chain reaction to herpes viruses was negative in all patients. IgG antibodies to ureaplasma - 2 (2.2%) recipients, mycoplasma - 8 (8.9%), garden henna - five (5.6%), candida - 14 (15, 7%), chlamydia - eight (8.9%), among recipients with antibodies class Ig G to chlamydia, one had poorly positive antibodies of class M. IgM antibodies to trichomoniasis were determined in 3 (3,4%) recipients.
Markers of viral hepatitis B and C were detected in 20 (22.5%) recipients: HBcorAg - 17 (19.1%), HBsAg - 1 (1.1%), HbeAg- 2 (2.2%). Quantitative polymerase chain reaction (PCR) to hepatitis B virus was positive in 2 recipients (with antiviral treatment before transplantation and subsequent negative PCR). IgG antibodies to hepatitis C virus were in 5 (5.6%) patients. PCR to hepatitis C virus was negative in all patients.
Immunosuppressive therapy in all recipients was initiated before transplantation for induction of immunosuppression in order to prevent the acute rejection crisis. Often several immunosuppressive drugs were prescribed from different groups with different mechanisms of action: glucocorticosteroid (medrol), antiproliferative (seelsept) and calcium calcineurin inhibitor (sandimun- neoral or advargaf). After kidney transplantation all patients received supportive immunosuppressive therapy according to the protocol (medrol, advagraf, myfortic); 2 (2.2%) recipients - serticans. All patients received prophylactic antiviral therapy (herpevir, valciclovir).
Acute graft rejection crisis has developed in 12 (13.5%) recipients, which corresponds to the data of the literature, according to which acute rejection crises occur in 10-15% of the total number of transplants [5, 9]. Among whom 5 (5.6%) died and 7 (7.8%) were included into hemodialysis. In order to stop the acute crisis of rejection, all recipients received pulse therapy of methyl prednisolone and if pulse therapy was not effective they received sandimun neoral, timoglobulin, antimonocytic immunoglobulin. In 1 (1.1%) patient graft function was restored.
Our study described in more detail in our previous work showing the prediction of graft survival using Kaplan- Meier and machine learning methods for predicting graft survival after transplantation [10]. Also, our previous study can be compared with the studies of Iranian scientists, who concluded that the use of intellectual analysis methods can play a functional role in predicting the results of kidney transplantation [11].
Conclusion
The main problems of transplant ology in Ukraine and in particular in Lviv are the lack of funding for immunodiagnostic for transplantation. Solving these problems will improve the survival and life expectancy of the recipient with a transplant.
Conflict of Interest
This work has no conflict of interest.
References
-
Golab J, Jakobisiak M, Lasek W, Stoklosa T (2015) Immunologia. PWN Scientific Publishing House SA, Warszawa, Poland, pp: 498.
-
The Law of Ukraine (1999) On the Transplantation of Organs and Other Human Anatomical Materials.
-
Nikonenko AS (2011) State and prospects of transplantation development in Ukraine. Modern medical technologies 3-4: 12-15.
-
The Law of Ukraine (2018) About the use of transplants of human anatomical materials.
-
Lisovii VM, Andoniev NM (2013) Topical issues of kidney transplantation. Educational manual for interns, Kharkiv National Medical University, Kharkiv, pp: 184.
-
(2022) Ukrainian doctors performed 20% more organ transplants than in the pre-war year 2021.
-
Cao K, Hollenbach J, Shi X, Shi W, Chopek M, et al. (2001) Analysis of the frequencies of HLA-A, B, and C alleles and haplotypes in the five major ethnic groups of the United States reveals high levels of diversity in these loci and contrasting distribution patterns in these populations. Hum Immunol 62(9): 1009-1030.
-
Mulley WL, Canellis GN (2011) Understanding crossmatch testing in organ transplantation: A case- based guide for the general nephrologist. Nephrology (Carlton) 16(2): 125-133.
-
Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group (2009) KDIGO Clinical Practice Guideline for the Care of Kidney Transplant Recipients. Am J Transplant9(Suppl 3): S1-155.
-
Tolstyak Y, Zhuk R, Yakovlev I, Shakhovska N, Gregus M, et al. (2021)The Ensembles of Machine Learning Methods for Survival Predicting after Kidney Transplantation. Applied Sciences 11(21): 10380.
-
Aslani N, Galendar N, Garavand A (2023) A systematic review of data mining applications in kidney transplantation. Informatics in Medicine Unlocked 37: 101165.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report