Primary Reconstruction of Bladder Neck Transection and Vaginal Laceration Post Blunt Abdominal Injury a Case Report
Blunt abdominal injury is not uncommon in the paediatric population. The presentation can be immediate or delayed, and if not promptly recognized may be attended with complications such as septicaemia, shock or death. Simple, readily available and cheap imaging techniques such as abdominal radiograph and ultrasound scan still remain relevant in the diagnosis of blunt abdominal injuries where abdominal computerized tomography is unavailable or unaffordable. This can expedite the decision for an early surgical exploration. In girls, complete bladder neck transection with vaginal wall injury is a rarely reported and unusual association of blunt abdominal injury more so with delayed presentation in the absence of an associated pelvic fracture. This rare trauma entity in a child can pose a diagnostic difficulty leading to delayed presentation. This is a case of 3 year old girl with 3 weeks history of trauma to the abdomen from collapsed building fence during a heavy downpour. She later developed progressive abdominal distension with pain, constipation, vomiting, fever and drainage of clear fluid per vaginam. She had visited several hospitals but was managed non-operatively. Over the period the patient had some relief of symptoms until she presented to our facility with poorly defined features of peritonitis following a referral from a peripheral hospital. Abdominal ultrasound scan revealed intraperitoneal fluid collection. She was resuscitated and had exploratory laparotomy with primary reconstruction of the bladder neck transection and vaginal wall laceration. She did well immediate postoperative except for the superficial surgical site infection and during follow-up visits. Primary repair of traumatic bladder neck transection and vaginal wall laceration in paediatric patients with delayed presentation of blunt abdominal injury is a feasible option of management. However, long term follow up is recommended as secondary procedures may become necessary.
Introduction
Abdominal injury is one of the organ-system injuries that can occur in the paediatric population. It is present in a quarter of children with major trauma and the most common cause of unrecognized fatal injury in paediatric patients [1]. Depending on the aetiological factor, children may present with blunt or penetrating abdominal injury. Paediatric abdominal trauma is typically blunt in nature with the spleen the most commonly affected viscera [1]. The timing of presentation of this injury to the health care facilities has a great impact on the overall management outcome. Most penetrating abdominal injury warrant emergency exploratory laparotomy due to associated major vascular or visceral injury as opposed to the blunt trauma where non-operative intervention is a common practice especially in the paediatric age group. Delayed presentation with blunt abdominal injury is not uncommon especially in the paediatric population and up to 19% of cases have been noted to present after three days following trauma [2]. The bladder involvement excluding bladder neck in blunt paediatric abdominal injury is uncommon and accounts for about 3% [2].
The delayed presentation may be attended by severe complications such as septicaemia, shock or death if not promptly recognized. In the absence of abdominal computerized tomography, the simple, readily available and cheap abdominal ultrasound scan or plain radiograph can aid the diagnosis and decision making for surgical exploration. Complex bladder neck, urethral and vaginal injuries particularly in girls following trauma excluding associated pelvic fracture are rarely reported by Pichler R, et al. [3]. Timely identification and management of these injuries can minimize associated potentially severe morbidity, which may include urinary incontinence and impaired sexual function. The rarity of this complex injury, difficulty in diagnosis and interestingly its late presentation makes it pertinent to report this case in a three year-old girl survivor with blunt abdominal injury and share our experience of her management.
Case Report
Chief Complaints
This is a three year-old girl who presented to the emergency room following a three week history of collapse of the wall around their home during a heavy rainfall.
History of Present Illness
She later developed progressive abdominal distension with pain, constipation, vomiting, fever, and altered level of consciousness. There was history of inability to pass urine per urethra immediate post trauma but later started draining clear fluid per vaginam. She was taken to a peripheral hospital where attempts at catheterization was successful however no drainage of urine. On account of this, she was taken to a number of hospitals but was managed non-operatively with antibiotics and analgesics. Over the period the patient had some relief of symptoms until lately when she presented to our facility with poorly defined features of peritonitis following a referral from a peripheral hospital.
History of Past Illness
There was no remarkable past medical or surgical history.
Personal and Family History
These were not remarkable.
Physical Examination
She was acutely ill-looking with Glasgow coma score of 12/15, pale, febrile (37.6°C), dehydrated and anicteric. Her vital signs were: temperature (38.2°C), respiratory rate (24 cycles/min), heart rate (160beats/min), and blood pressure 70/40 mmHg. The abdomen was intact but distended moderately without patterned sign or laceration with vague generalized tenderness, marked over suprapubic region. The vulva was soiled with clear fluid with a size 8Fr urethral catheter in situ which had drained a scanty purulent effluent. The other examinations findings were not remarkable.
Laboratory Examinations
The serum urea was 22.0 mmol/L, creatinine 2.5 mg/ dL, and electrolytes: Na+ 128 mmol/L, K+ 3.1 mmol/L, HCO3 - 16 mmol/L and Cl- 94 mmol/L. The complete blood cell count was 9.1 × 109/L and packed cell volumes of 26 %. The effluent (urine) culture yielded growth of Staphylococcus aureus sensitive to ceftriaxone & sulbactam.
Imaging Examinations
Abdominal ultrasound scan revealed intraperitoneal fluid collection with internal echoes but indistinct bladder probably due to suspected intraperitoneal bladder injury.
Diagnosis
The preoperative diagnosis of blunt abdominal injury with generalized peritonitis ? cause to rule out hollow viscera injury was made.
Resuscitation and Treatment
She was resuscitated with intravenous fluids, blood transfusion, broad-spectrum parenteral antibiotics with cover for anaerobes before the availability of culture result. Afterwards, the parent was counseled for emergency exploratory laparotomy which she had with primary reconstruction of the bladder neck transection and repair of the vaginal wall laceration. The intraoperative findings were encased pus about 15 mls anterior to the bladder, about a litre of free intraperitoneal fluid containing fibrinoid debris, an incidental intraoperative finding of a complete urethral transection from the bladder neck Figure 1A. The ureteric orifices were spared. There was also a transverse 2cm anterior vaginal wall tear but the cervical os, posterior vaginal and rectal wall were intact (Figure 1A).
The abdominal cavity was generously lavaged with five (5) litres of warm normal saline. The wounds edges were debrided. Then, the anterior vaginal wall laceration was sutured interruptedly using vicryl 3/0 sutures. The distal urethral stump was spatulated on one side and six interrupted vicryl 4/0 sutures were placed in the urethral stump and bladder neck at relative equidistance before tying each to effect end-to-end anastomosis or bladder neck-to- urethral reconstruction over size 10 fr silicon urethral stent/ catheter (Figure 1B). The bladder was closed water tight over 14fr latex suprapubic cystostomy (SPC) catheter. The abdominal wound was closed en-mass over a perivesical drain.
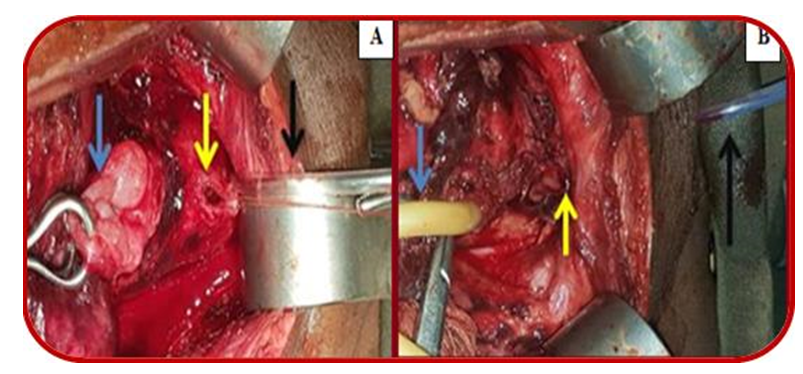
Figure 1: Intraoperative Images. A Intraoperative findings displaying transected oedematous bladder neck (blue arrow), feeding tube in distal urethral stump (black arrow), and anterior vaginal wall laceration (yellow arrow); B: Appearance after primary reconstruction of bladder neck and anterior vaginal wall showing suprapubic cystostomy catheter (blue arrow), silicon urethral stent (black arrow), and site of bladder neck reconstruction (yellow arrow).
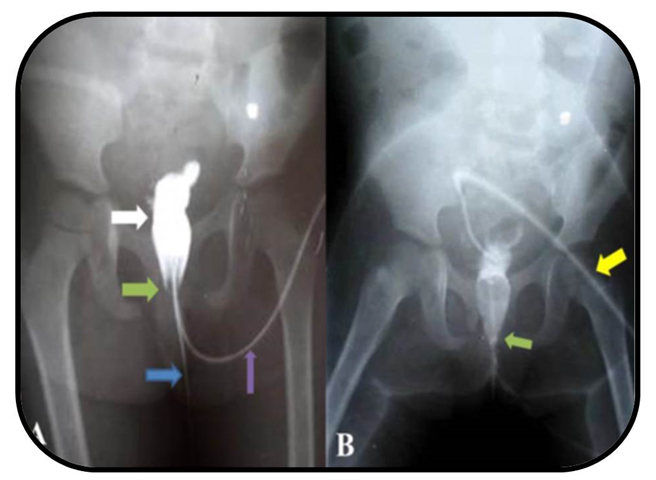
Figure 2: Postoperative contrast imaging studies at postoperative day 21. A Pericatheter RUCG showing the contrast filled bladder (white arrow), site of urethrovesical anastomosis demonstrating no contrast leak (green arrow), silicon urethral catheter/stent (blue arrow), and periurethral catheter for contrast administration (purple arrow) and B: VCUG (diluted contrast) site of urethrovesical anastomosis demonstrating no contrast leak (green arrow) and suprapubic cystostomy catheter (yellow arrow).
She did well immediate postoperative but developed superficial surgical site infection on the postoperative day seven which was managed with wound dressing. The serum biochemistry returned to normal within the first postoperative week. A pericatheter retrograde urethrograpy (RUCG) and voiding cystourethrography (VCUG) performed three weeks after surgery revealed an intact urethra and bladder neck without contrast leak (Figure 2A & B). She had delayed removal of the perivesical drain until 10 days postoperative because of the initial significant drainage before reduction (Figure 1). The SPC catheter was spigoted and urethral stent was removed on fourth postoperative week. SPC catheter was removed 6-weeks postoperative after satisfactory 2-weeks observation of urethral voiding. She had initial complaints of incontinence probably from prolonged indwelling catheter which improved during follow up visits (Figure 2).
Discussion
Pediatric urethral trauma poses a significant challenge for urologists due to its rarity and potentially serious consequences. In girls, this injury is more infrequent than in boys due to the short, mobile nature of the urethra, and its well-secured location behind the pubic bone [3]. Urethral injuries could result from blunt or penetrating trauma to the abdomen or perineum. Blunt injuries occur more frequently than penetrating trauma making up more than 80% of abdominal trauma [4]. Injuries in females are usually associated with pelvic fractures due to the anatomical relationship between the urethra and the bony arch of the pubis. The bladder in the index patient’s age is predominantly abdominal in location as opposed to older children or adult’s pelvic location. In blunt abdominal injury, this anatomical disposition makes it easy to appreciate the mechanism of injury here whereby a falling piece of brick crushes the bladder neck which is relatively abdominal and unprotected by the bony pelvis against the sacral bone or promontory.
Based on the degree of disruption and separation of the urethra on retrograde urethrography, the American Association of Surgery for Trauma (AAST) classified urethral injury into five grades of ascending severity [5]. Complete urethral transection with extension to the vagina as with our index patient is an AAST grade five urethral injury. There have been few cases of combined female urethral and vaginal injuries without associated pelvic fracture reported in literature. The first two cases were injuries following motor vehicle accidents with resultant complete disruption between the urethra and the distal bladder neck and longitudinal urethral tear with vaginal involvement respectively [6, 7]. The third and fourth cases were due to a straddle injury from sharp objects causing complete urethral avulsion with associated anterior vaginal wall laceration and complete transection respectively [8, 9]. In our patient the injury occurred as a result of wall collapse. The magnitude of force at impact and the close proximity of vagina to bladder and urethra explain the pathology of this complex injury.
The classical triad of blood at the urethral meatus, inability to pass urine and palpable bladder is the common presentation of urethral-injured patients [10]. These usually necessitate intervention in the form of urethral catheterization, suprapubic cystostomy and/or primary realignment. These classical features were absent in the index case, hence, the diagnostic challenges and delayed presentation. In the emergency room, lower genitourinary injuries may be overlooked by attending physician while attending to other potentially life threatening system injuries in a polytraumatized patient. Black, et al. [11] reported nearly 25% of urinary injuries accidentally diagnosed during surgical exploration for trauma. Delayed presentation as with our patient altered the clinical picture to those of sepsis, abdominal distension, a poorly draining urethral catheter and leakage of clear fluid per vaginum. Hence the diagnosis of complete urethral transection and anterior vaginal wall injury was only made by chance during surgical exploration.
The surgical treatment principles for pediatric urethral trauma are similar to those in adults due to the limited available data specific to children. The management in females is an evolving discussion with the argument on whether primary repair is favored over secondary delayed anastomosis and repair [12]. The treatment should depend on accurate diagnosis for the extent of the injuries which may be best achieved by endoscopic or direct examination of lower genitourinary tract. Our patient was successfully treated by primary spatulated end-to-end anastomosis of the urethra with both suprapubic and urethral catheters left in place for urinary diversion and to minimize postoperative urethral stenosis respectively. She also had primary repair of the anterior vaginal wall laceration. Although she had some degree of urinary incontinence initially, six months postoperative follow up showed no signs of long term genitourinary morbidity.
Conclusion
The delayed presentation of blunt abdominal injury with complete bladder neck transection and vaginal wall laceration in a child is rarely encountered but possible. Proper clinical evaluation in addition to the judicious use of readily available and cheap trans abdominal ultrasound scan as well as abdominal radiograph have their roles where abdominal computerized tomography is unavailable or unaffordable in the diagnosis and guiding decision for early surgical exploration. Exploratory laparotomy with generous lavage of the peritoneal cavity and primary reconstruction of the bladder neck and vaginal wall laceration is feasible following delayed presentation of blunt abdominal injury and associated with good outcome. Notwithstanding, we passionately call on the parents to safeguard their wards especially during heavy downpour. We also appeal and urge the government to enforce child rights laws as it applies to the safety of children and at the same time sanction erring parents according to the provisions of the laws.
Declarations
Ethics Approval and Consent To Participate
Consent for treatment obtained and institutional ethical standard adhered to with the Institutional Health Research Ethics Committee approval number (UDUTH/ HREC/2023/1333).
Consent for Publication
Consent was taken from the patient’s father.
Competing Interests
The authors declare that they have no competing interests.
Funding
This study received no funding from any funding agency in the public, commercial, and not-for-profit sectors.
Authors’ Contributions
AK, AY, OOG, OUE are responsible for the design and implementation of the research. AK, AY, and OUE acquired the data. AK, AY, and OOG, did literature search on the subject. AK, AY, OOG, and OUE contributed to the initial draft of this work. ANP and AAA did additional literature search on the subject and critically revised the initial draft of this manuscript. All authors read and approved the final manuscript.
Availability of Data and Materials
Data sharing is not applicable to this article as no dataset were generated or analyzed during this study.
Acknowledgements
Not applicable.
References
-
Lynch T, Kilgar J, Al SA (2018) Pediatric Abdominal Trauma. Curr Pediatr Rev 14(1): 59-63.
-
Divya G, Kundal VK, Addagatla R, Garbhapu AK, Debnath PR, et al. (2023) Spectrum of paediatric blunt abdominal trauma in a tertiary care hospital in India. Afr J Paediatr Surg 20(3): 191-196.
-
Pichler R, Fritsch H, Skradski V, Horninger W, Schlenck B, et al. (2012) Diagnosis and management of pediatric urethral injuries. Urologia internationalis 89(2): 136- 142.
-
Jullien S (2021) Prevention of unintentional injuries in children under five years. BMC Pediatr. 21(Suppl 1): 311.
-
Moore EE, Cogbill TH, Malangoni MA, Jurkovich GJ, Shackford SR, et al. (1995) Organ injury scaling. Surg Clin North Am 75(2): 293-303.
-
Podestá ML, Jordan GH (2001) Pelvic fracture urethral injuries in girls. J Urol 165(5): 1660-1665.
-
Mc CAC, Joseph DB (2001) Complete urethral disruption without pelvic fracture. J Urol 166(4): 1425.
-
Al-Asbahi WA (2015) Traumatic female urethral avulsion. Saudi Med J 36(3): 366-367.
-
Truong BT, Rich MA, Swana HS (2016) Complete traumatic transection of urethra and vagina in a child. J Pediatr Surg Case Rep 12: 6-8.
-
Kong JP, Bultitude MF, Royce P, Gruen RL, Cato A, et al. (2011) Lower urinary tract injuries following blunt trauma: a review of contemporary management. Rev Urol 13(3): 119-130.
-
Black PC, Miller EA, Porter JR, Wessells H (2006) Urethral and bladder neck injury associated with pelvic fracture in 25 female patients. J Urol 175(6): 2140-2144.
-
Hosseini J, Tavakkoli TK, Razi A (2009) Delayed retropubic urethroplasty of completely transected urethra associated with pelvic fracture in girls. Urol J 6(4): 272-275.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report